does lsd ude cause any retinopathies
LSD retinopathy lysergic acid diethylamide
PMID: 32064962
LSD retinopathy ocular effects lysergic acid diethylamide macular damage
https://en.wikipedia.org/wiki/Drug_abuse_retinopathy
LSD and Retinopathy
Does LSD directly cause retinopathy?
1. Solar / Phototoxic Maculopathy (most well-established)
- Small yellow or red foveolar spot shortly after exposure
- Evolves to a sharply defined foveolar defect with irregular borders or a lamellar hole
- OCT: foveal thinning with focal hyporeflective area involving photoreceptor inner and outer segments
- Variable reduction in visual acuity, with a small central scotoma
- No specific treatment; prognosis is generally good, with improvement over 6 months, though some patients retain permanent visual loss
2. Direct Retinal Toxicity (animal/experimental evidence)
- LSD administered intraperitoneally to C57 mice at escalating doses (0.2-1.2 mg/kg twice daily for 5 days) caused measurable retinal damage
- Electroretinography (ERG) showed decreased response
- Histology showed loss of photoreceptor cells
- The mechanism involved upregulation of p-JAK1/p-STAT1, promoting photoreceptor apoptosis via the JAK/STAT pathway
3. Hallucinogen-Persisting Perception Disorder (HPPD)
- Enhanced color sensitivity, halos around lights
- Trailing and stroboscopic perception of moving objects
- Afterimages, palinopsia, macropsia/micropsia
Summary Table
| Mechanism | Type of Damage | Evidence Level |
|---|---|---|
| Sun-gazing while intoxicated | Solar maculopathy (RPE + foveal photoreceptor damage) | Case reports in humans |
| Direct retinal toxicity via JAK/STAT apoptosis | Photoreceptor cell loss | Animal study (mouse) |
| HPPD (cortical, not retinal) | Persistent visual disturbances, no structural lesion | Clinical/observational |
Post viral retinopathies
post-viral retinopathy retinal
viral retinitis retina herpes CMV
PMID: 39770716
post viral retinopathy types causes mechanisms 2024
Post-Viral Retinopathies
- Direct viral invasion of retinal cells (necrotizing, cytolytic)
- Immune-mediated / inflammatory damage triggered by viral antigens (vasculitis, pigmentary changes, uveitis)
1. Herpetic Necrotizing Retinopathies
A. Acute Retinal Necrosis (ARN)
- One or more discrete foci of peripheral retinal necrosis with well-defined borders
- Rapid circumferential progression without antiviral therapy
- Occlusive vasculopathy with arterial involvement (retinal arteritis)
- Prominent anterior chamber and vitreous inflammation (panuveitis)
- Blurred vision, floaters, ocular pain, photophobia
- Deep yellow-white peripheral infiltrates
- Retinal haemorrhages (less prominent than CMV)
- Optic neuritis in some cases
- Secondary rhegmatogenous retinal detachment (RRD) in ~70% of cases - major cause of visual morbidity
- May involve the second eye in one-third of cases within weeks to months
- Oral valacyclovir 1-2 g TID or famciclovir 500 mg TID + supplemental intravitreal foscarnet or ganciclovir injections 1-2x/week
- Alternative: IV acyclovir 10 mg/kg TID for 5-14 days, then oral maintenance for minimum 2 months
- Topical cycloplegic + steroids for anterior inflammation
- Prophylactic barrier laser photocoagulation (efficacy unclear)
- Pars plana vitrectomy for associated complex RRD
- Systemic steroids (delayed at least 24 hours after antiviral initiation)
B. Progressive Outer Retinal Necrosis (PORN)
- Rapidly progressive, characterized by sheet-like opacification deep to normal-looking retinal vessels
- Vitreous is clear (minimal vitritis) - key distinguishing feature from ARN
- Macula involved early (unlike ARN where it is spared early)
- Pain and anterior uveitis are minimal
- Frequently leads to rapid bilateral blindness due to retinal detachment
- Prompt diagnosis and treatment is critical
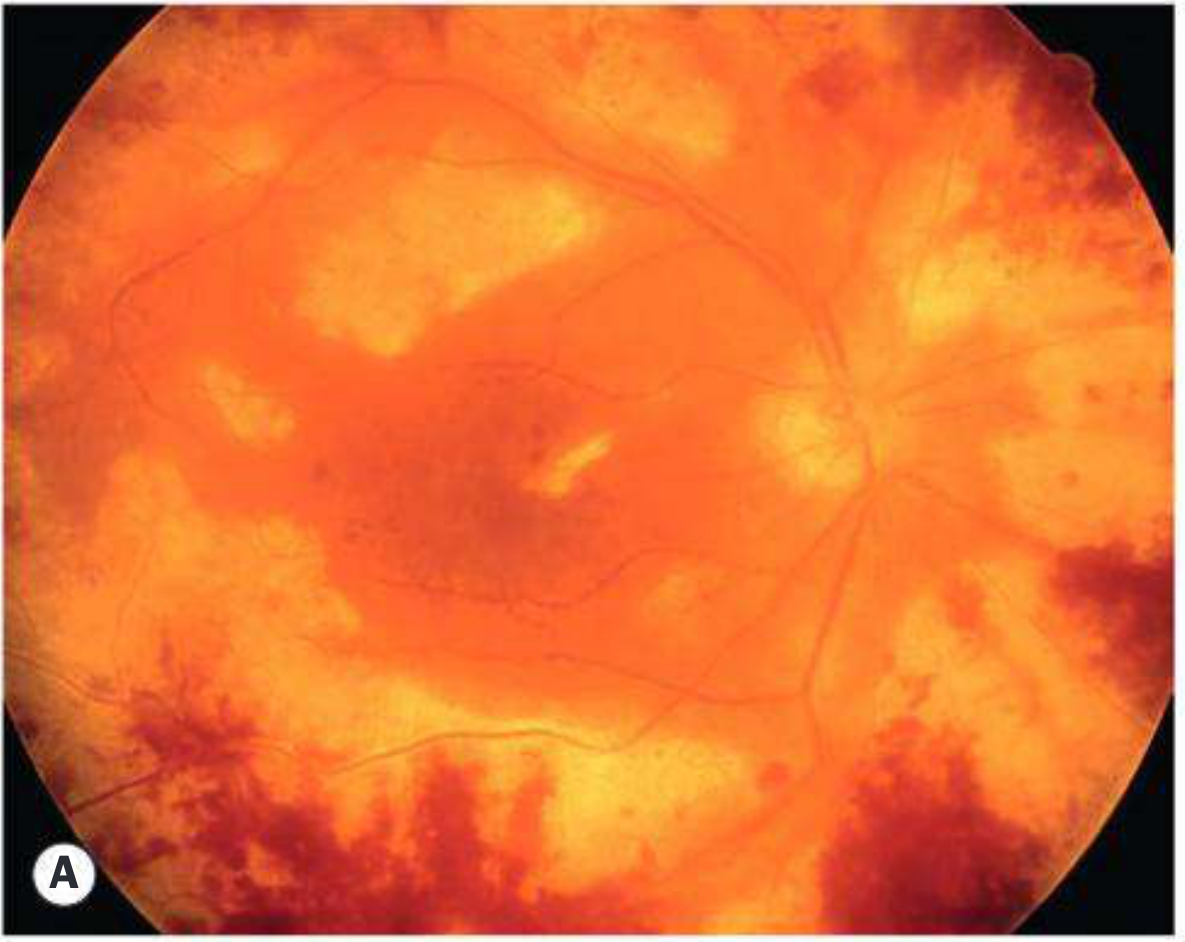
C. CMV Retinitis
- Indolent form: Peripheral granular opacities ± hemorrhage
- Fulminant form: Confluent areas of necrosis with prominent hemorrhage, starting along the major vascular arcades ("brushfire" or "pizza pie" pattern)
| Drug | Induction | Maintenance |
|---|---|---|
| Ganciclovir (IV) | 5 mg/kg IV BID x 14 days | 5 mg/kg IV daily |
| Valganciclovir (oral) | 900 mg PO BID x 21 days | 900 mg PO daily |
| Foscarnet | 90 mg/kg IV BID | 90-120 mg/kg IV daily |
| Cidofovir | 5 mg/kg IV weekly x 2 | 5 mg/kg IV every 2 weeks |
2. Congenital Viral Retinopathies (Pigmentary)
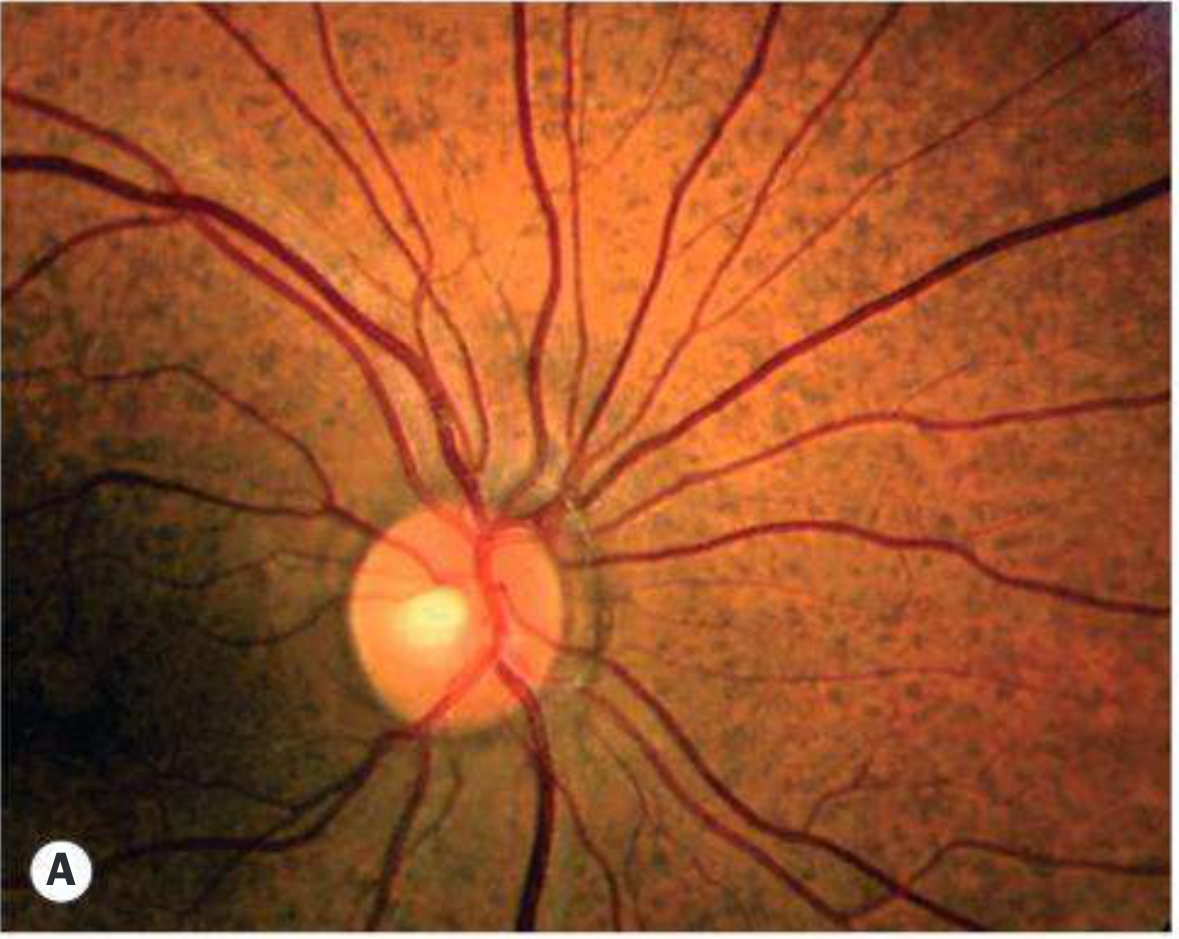
A. Rubella Retinopathy
- "Salt and pepper" pigmentary retinopathy - the hallmark finding, caused by irregular RPE pigmentation across the posterior pole
- Cataract, anterior uveitis, glaucoma, microphthalmos
- Latent rubella can cause chronic anterior uveitis (Fuchs uveitis syndrome association)
B. Congenital CMV Retinopathy
C. Congenital Zika Virus
- Microcephaly and CNS malformations in neonates
- Ocular effects: chorioretinal and macular atrophy, focal pigmentary macular changes, optic nerve abnormality, glaucoma
- In adults with acute infection: conjunctivitis (most common), then uveitis
- Virus persists in the lacrimal gland and retinal pigment epithelium
3. Post-Viral Immune-Mediated Retinopathy
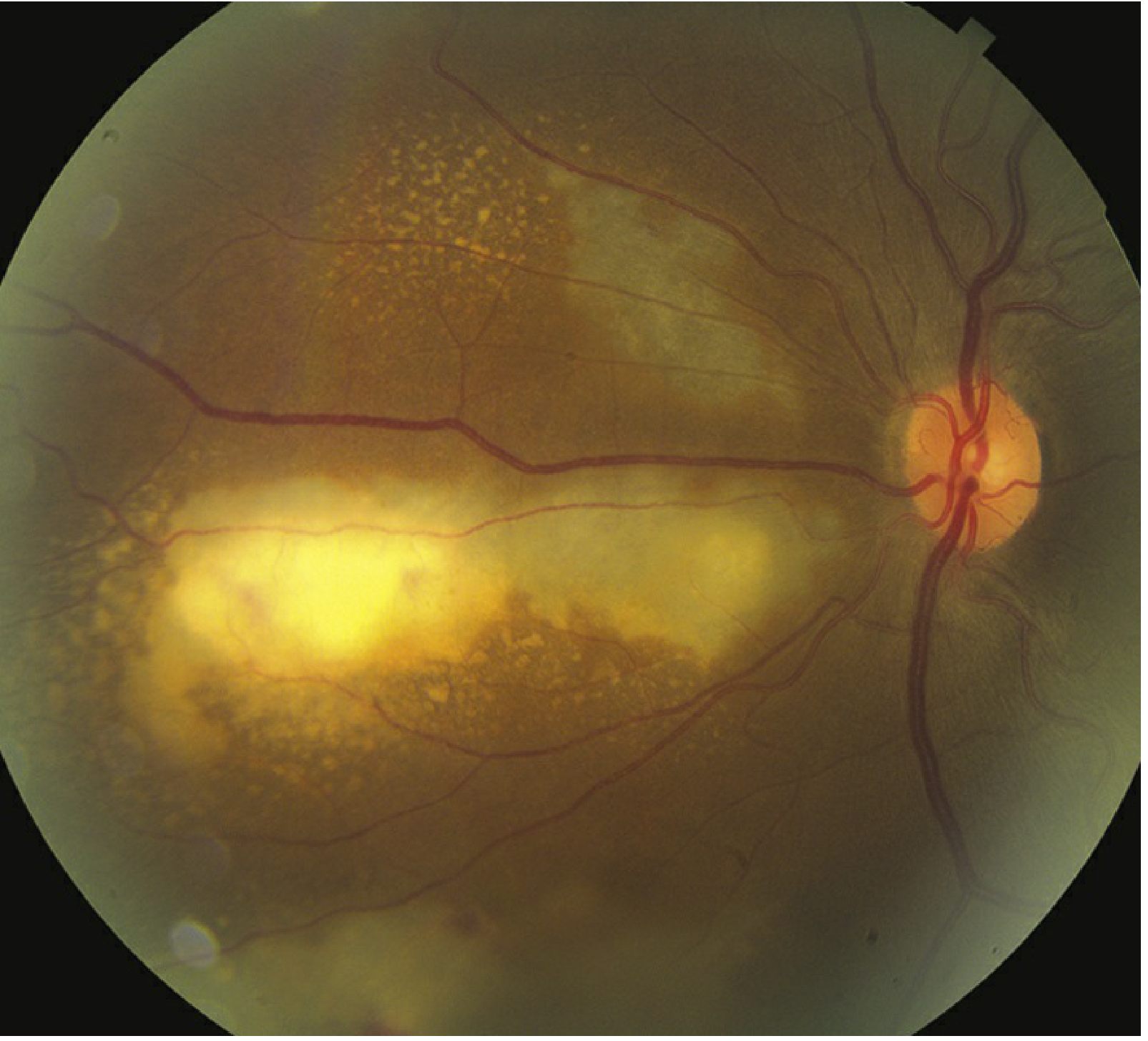
A. Subacute Sclerosing Panencephalitis (SSPE) - Measles
- Progressive neurological degeneration (personality change → choreoathetosis → myoclonus → death)
- Ocular: posterior uveitis, papilloedema, optic neuritis, nystagmus
- Ischaemic retinal vein occlusion secondary to vasculitis (rare)
- Classical macular lesion: white/grey-white patch resolving to macular scarring and RPE atrophy
B. Ebola Virus Disease
- Uveitis in up to 1/3 of survivors, occurring within 2 months of discharge
- Anterior, posterior, or panuveitis
- Up to 15% develop cataract
- Optic nerve swelling in 10%
- Ebola virus detected in aqueous and can infect and persist in RPE cells
- Treatment: topical + oral corticosteroids; must start early to prevent permanent visual loss
Summary Comparison
| Virus | Population | Retinal Pattern | Key Feature |
|---|---|---|---|
| HSV/VZV (ARN) | Immunocompetent | Peripheral necrotizing retinitis | Occlusive arteritis, RRD in 70% |
| VZV/CMV (PORN) | Immunocompromised | Outer retinal necrosis, starts posteriorly | Clear vitreous, rapid blindness |
| CMV | AIDS/transplant | Vascular-arcuate necrosis + haemorrhage | "Pizza pie" pattern, minimal inflammation |
| Rubella (congenital) | Neonates | Diffuse RPE pigmentary changes | "Salt and pepper" fundus |
| Measles/SSPE | Children/teens | Macular scarring, vasculitis | Delayed CNS + retinal disease |
| Zika (congenital) | Neonates | Macular/chorioretinal atrophy | Optic nerve anomalies |
| Ebola (post-infectious) | Survivors | Uveitis, RPE involvement | Virus persists in RPE |
Does cannabis usage cause retinopathies
cannabis marijuana retina retinopathy
cannabis cannabinoids retinopathy retinal damage ocular effects 2024
PMID: 30773228
cannabis THC CBD ocular retinal function electroretinogram
https://pmc.ncbi.nlm.nih.gov/articles/PMC11613704
cannabis marijuana retinal vascular occlusion macular
PMID: 32947368
cannabis electroretinogram retinal function neurotoxicity
https://www.mdpi.com/2813-2564/4/4/22
cannabis retinal artery occlusion vasospasm young
Cannabis Use and Retinopathy
1. The Endocannabinoid System in the Retina
2. Neuroretinal Dysfunction (Functional Damage)
Electroretinographic (ERG) Changes
- Delayed implicit times in photopic (cone-driven) responses
- Increased retinal background noise - a 2019 study found elevated ERG noise in co-users of cannabis and alcohol (PMID 30292729, Lucas et al., Progress in Neuropsychopharmacology)
- Abnormal electrooculography (EOG) and electrically evoked phosphene thresholds in a heavy cannabis user later diagnosed with HPPD, suggesting direct cannabinoid effects on the retinal pigment epithelium (RPE) function (Zobor et al., 2015, cited in Bondok et al., Clin Ophthalmol 2024)
3. Vascular Retinopathy - Retinal Artery Occlusion
- A 21-year-old healthy male with no systemic risk factors
- Smoking ~15 g/day of cannabis during COVID-19 lockdown
- Acute branch retinal artery occlusion (BRAO) with right inferotemporal retinal whitening
- OCT showed paracentral acute middle maculopathy (PAMM) - ischaemic hyperreflectivity of inner and middle retinal layers
- OCT-angiography: flow signal loss in the deep capillary plexus
- Fluorescein angiography and full systemic workup: unremarkable (no other cause found)
- Proposed mechanism: transient arterial vasospasm induced by cannabis
4. Retinal Vascular Changes with Chronic Use
5. The THC:CBD Ratio - Neuroprotective vs. Neurotoxic
| THC:CBD Ratio | Retinal Effect |
|---|---|
| Low THC + adequate CBD (older strains, ~10:1) | Neuroprotective - reduces oxidative stress, protects photoreceptors |
| High THC + low CBD (modern strains, ~100:1) | Neurotoxic - promotes photoreceptor apoptosis, oxidative damage |
6. Potential Therapeutic Effects (Context)
- IOP reduction - THC lowers IOP by 25-30% (transient, lasting 3-4 hours; not a substitute for sustained glaucoma therapy)
- Diabetic retinopathy - preclinical evidence that CBD reduces retinal inflammation, neurotoxicity, and blood-retinal barrier breakdown
- Ischaemia - cannabinoid receptor agonists reduce retinal ischaemia-reperfusion injury in animal models
Summary
| Effect | Evidence | Mechanism |
|---|---|---|
| ERG dysfunction (delayed responses, increased noise) | Human studies | Disrupted dopaminergic/glutamatergic synaptic transmission |
| RPE dysfunction (EOG changes) | Case reports | Direct cannabinoid effect on RPE |
| Retinal artery occlusion / PAMM | Case reports (young adults) | Vasospasm, haemodynamic instability |
| Haemorrhagic macular infarction | Case reports | Vascular occlusion |
| Wider arteriolar diameter | Observational study | Residual vasodilation |
| Neurotoxicity (high-THC strains) | Animal/lab data | Oxidative stress, apoptosis - dose-dependent |