Stridor
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Find recent clinical guidelines on stridor management
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Periotic labyrinth
Reading File
Finding Sources
Searching the Web
periotic labyrinth anatomy bony osseous labyrinth
Reading File
Reading File
Reading File
Loading Image
Excellent - I have comprehensive information from the textbooks and a great anatomical diagram. Here is a thorough answer.
The Periotic (Bony/Osseous) Labyrinth
The term periotic labyrinth refers to the bony shell - also called the osseous labyrinth or otic capsule - that houses and protects the membranous labyrinth of the inner ear. It sits within the petrous part of the temporal bone, one of the densest bones in the body.
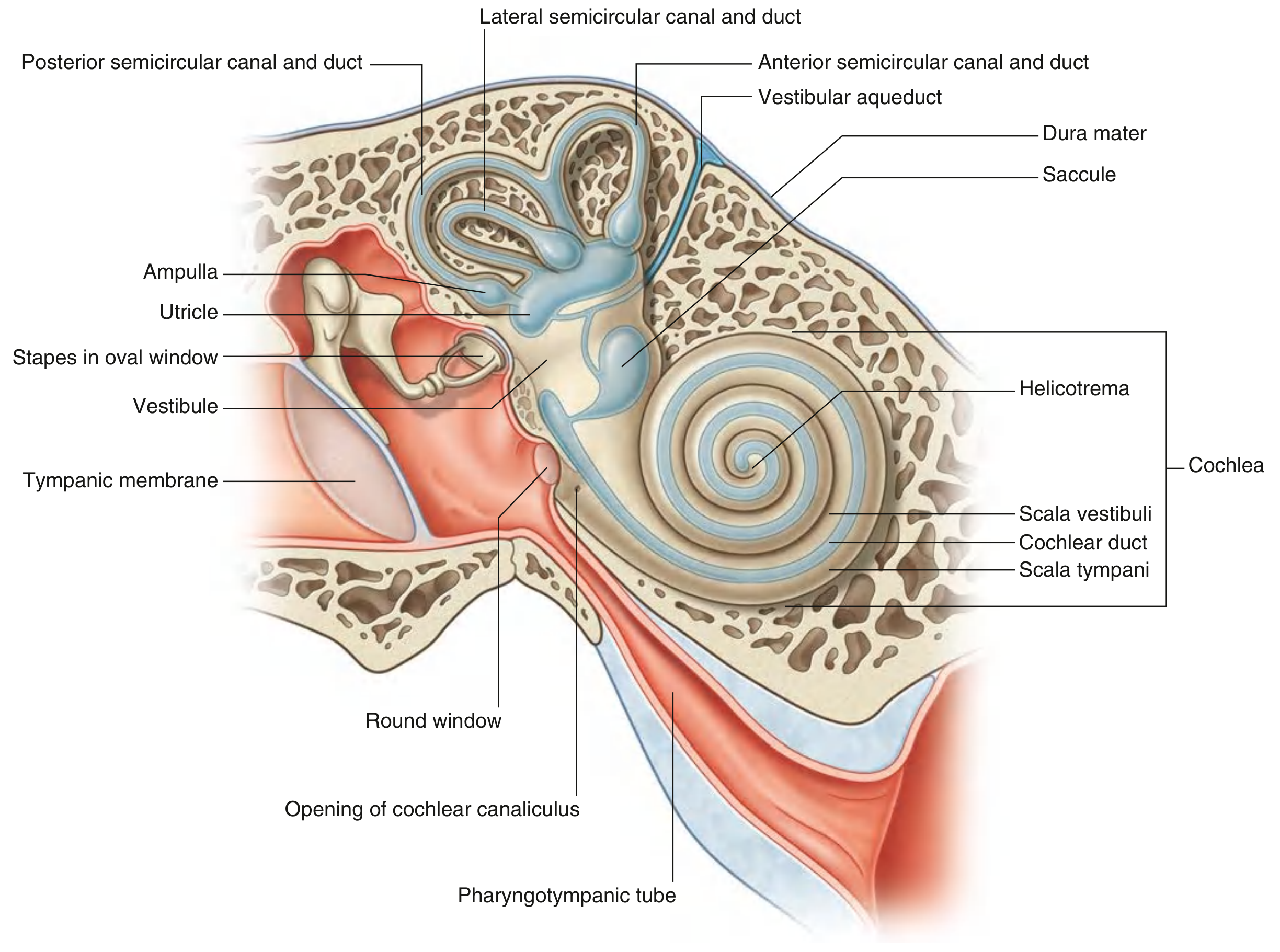
Parts of the Bony Labyrinth
The bony labyrinth has three main subdivisions:
1. Vestibule
- The central part of the bony labyrinth
- Contains the oval window in its lateral wall (where the stapes footplate transmits sound vibrations into the perilymph)
- Communicates anteriorly with the cochlea and posterosuperiorly with the semicircular canals
- Houses two sacs of the membranous labyrinth: the saccule and utricle (the otolith organs for linear acceleration and gravity detection)
- The vestibular aqueduct (endolymphatic duct) exits the vestibule and passes through the petrous bone to the posterior cranial fossa
2. Semicircular Canals
- Three canals - anterior (superior), posterior, and lateral - project posterosuperiorly from the vestibule
- Each canal forms two-thirds of a circle and opens at both ends into the vestibule
- The canals are oriented at right angles to each other, maximizing sensitivity to rotational movement in any plane
- One end of each canal is dilated to form the ampulla, which contains the crista ampullaris (sensory receptor for angular acceleration)
3. Cochlea
- Projects anteriorly from the vestibule
- A bony, snail-shaped structure that spirals 2.5 turns around a central bony axis called the modiolus
- The base faces posteromedially (near the internal acoustic meatus, where CN VIII enters)
- The osseous spiral lamina extends from the modiolus and, together with the cochlear duct (membranous labyrinth), divides the cochlear canal into:
- Scala vestibuli (superior) - continuous with the vestibule
- Scala tympani (inferior) - separated from the middle ear by the round window membrane
- The two scalae communicate at the apex via the helicotrema
- The round window (cochlear fenestra) is sealed by the secondary tympanic membrane
Fluid Compartments
| Compartment | Location | Fluid | Ionic Character |
|---|---|---|---|
| Perilymph | Between bony and membranous labyrinth | Similar to ECF / CSF | High Na⁺, low K⁺ |
| Endolymph | Inside membranous labyrinth | Unique | High K⁺, low Na⁺ |
The perilymph fills the space between the bony and membranous labyrinths (periotic space). It is in communication with CSF via the cochlear aqueduct (canaliculus cochleae), which connects the scala tympani to the subarachnoid space.
Development (Embryology)
- Around day 22-23, an ectodermal thickening called the otic placode forms on the side of the embryonic head
- It deepens to form the otic pit, then pinches off as the otocyst (otic vesicle)
- The surrounding mesenchyme chondrifies to form the otic capsule, which then expands as the membranous labyrinth grows
- Ossification of the cartilaginous otic capsule begins at approximately week 16 from multiple centers, eventually fusing into the extremely dense petrous bone - notably without suture lines
- The perilymphatic spaces form by dedifferentiation (resorption) of the cartilaginous otic capsule surrounding the membranous labyrinth
Clinical Relevance
- Otosclerosis: Abnormal remodeling of the otic capsule bone, typically at the oval window, causing conductive (and later sensorineural) hearing loss
- Labyrinthine fistula: Abnormal communication between perilymph and middle ear, causing fluctuating sensorineural hearing loss and vertigo
- Cochlear aqueduct patency: Important during intracranial surgery - raised ICP can transmit to the perilymph
- Temporal bone fractures: Transverse fractures (cutting across the petrous bone) can disrupt the bony labyrinth, causing profound sensorineural hearing loss and vertigo
Sources: Gray's Anatomy for Students, p. 1106; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, p. 586
Development ofinnerear
Finding Sources
Searching the Web
development of inner ear embryology otic placode otocyst membranous labyrinth
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive, well-sourced material from two authoritative ENT textbooks. Here is the full answer.
Development of the Inner Ear
Phylogenetic Background
The mammalian inner ear evolved from the lateral line system of fish - a water-motion detection system of fluid-filled pits innervated by cranial nerves VII, IX, and X. This system used hair cells and surrounding fluid (seawater), features recapitulated in the modern inner ear. The vestibular apparatus (phylogenetically older) develops before the cochlear structures, and this seniority explains the relative resistance of the semicircular canals and utricle to developmental malformations compared with the cochlea.
Stage 1 - Otic Placode Formation (~Day 22-23)
The process begins with a plaquelike thickening of surface ectoderm (dorsal to the first branchial groove) on the sides of the embryonic head, close to the developing neural tube and neural crest cells.
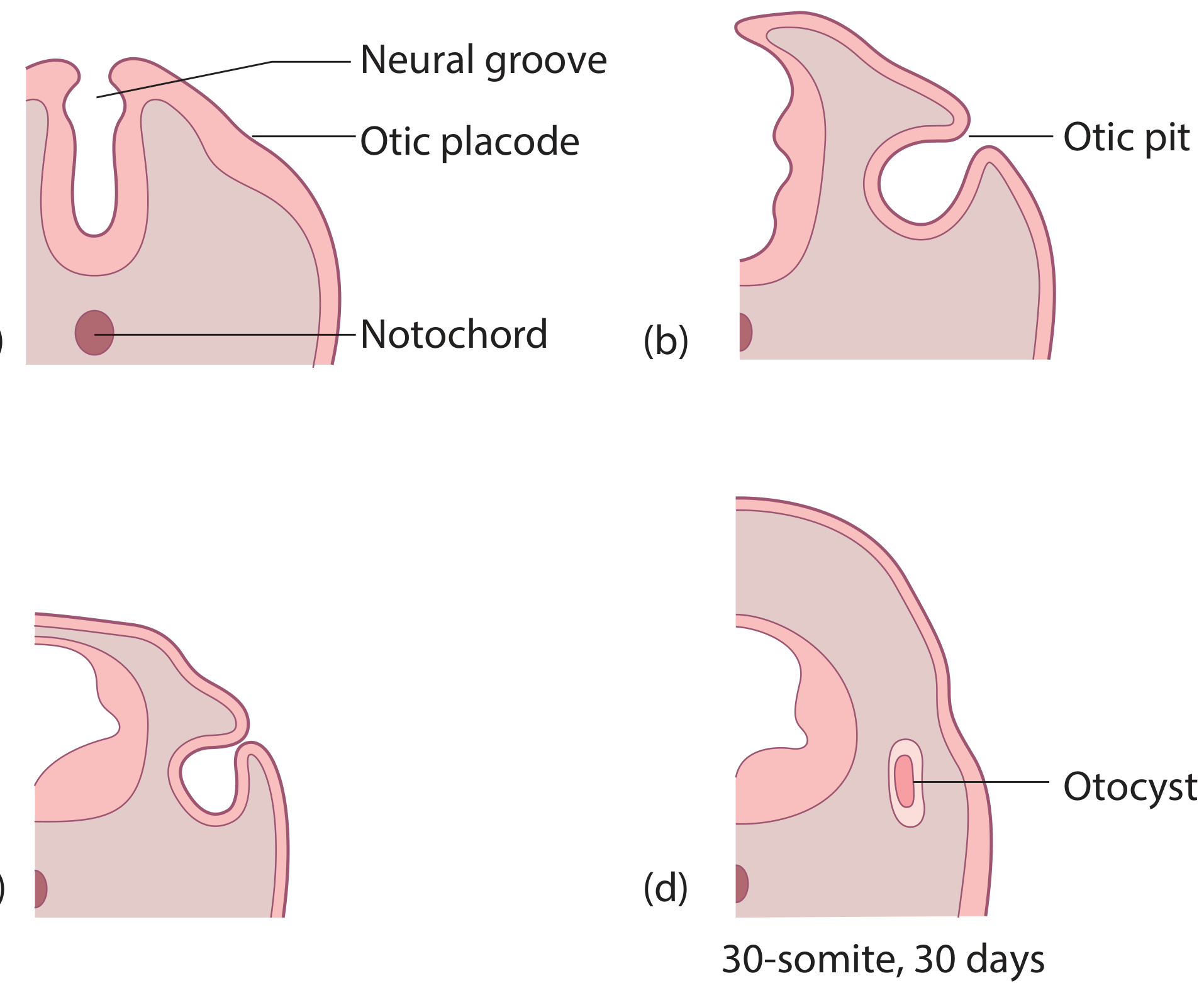
- The placode deepens into an otic pit (auditory pit) by invaginating into the underlying mesenchyme
- The pit closes off to form the otocyst (otic vesicle) - a fluid-filled sac completely separated from the surface by ~day 30
- Associated with the otocyst is a cluster of neural crest cells that will become the:
- Facial (geniculate) ganglion
- Auditory (spiral/cochlear) ganglion
- Vestibular (Scarpa's) ganglion
- The endolymphatic appendage appears at this stage, ahead of the semicircular or cochlear structures
Stage 2 - Otocyst Differentiation (Weeks 4-8)
Three deepening folds (I, II, III) indent the otocyst and demarcate its compartments:
| Fold | Gives rise to |
|---|---|
| Fold I | Utricle and semicircular ducts |
| Fold II | Endolymphatic duct and sac |
| Fold III | Saccule and cochlear duct; also forms the utriculoendolymphatic valve of Bast |
By week 4: Two flanges emerge as the future semicircular ducts
By week 6:
- Lumina of all three semicircular ducts have formed
- The macula communis (primordial sensory patch) divides into superior and inferior segments:
- Superior segment → maculae of utricle + cristae of superior and lateral semicircular ducts
- Inferior segment → macula of saccule + crista of posterior semicircular canal
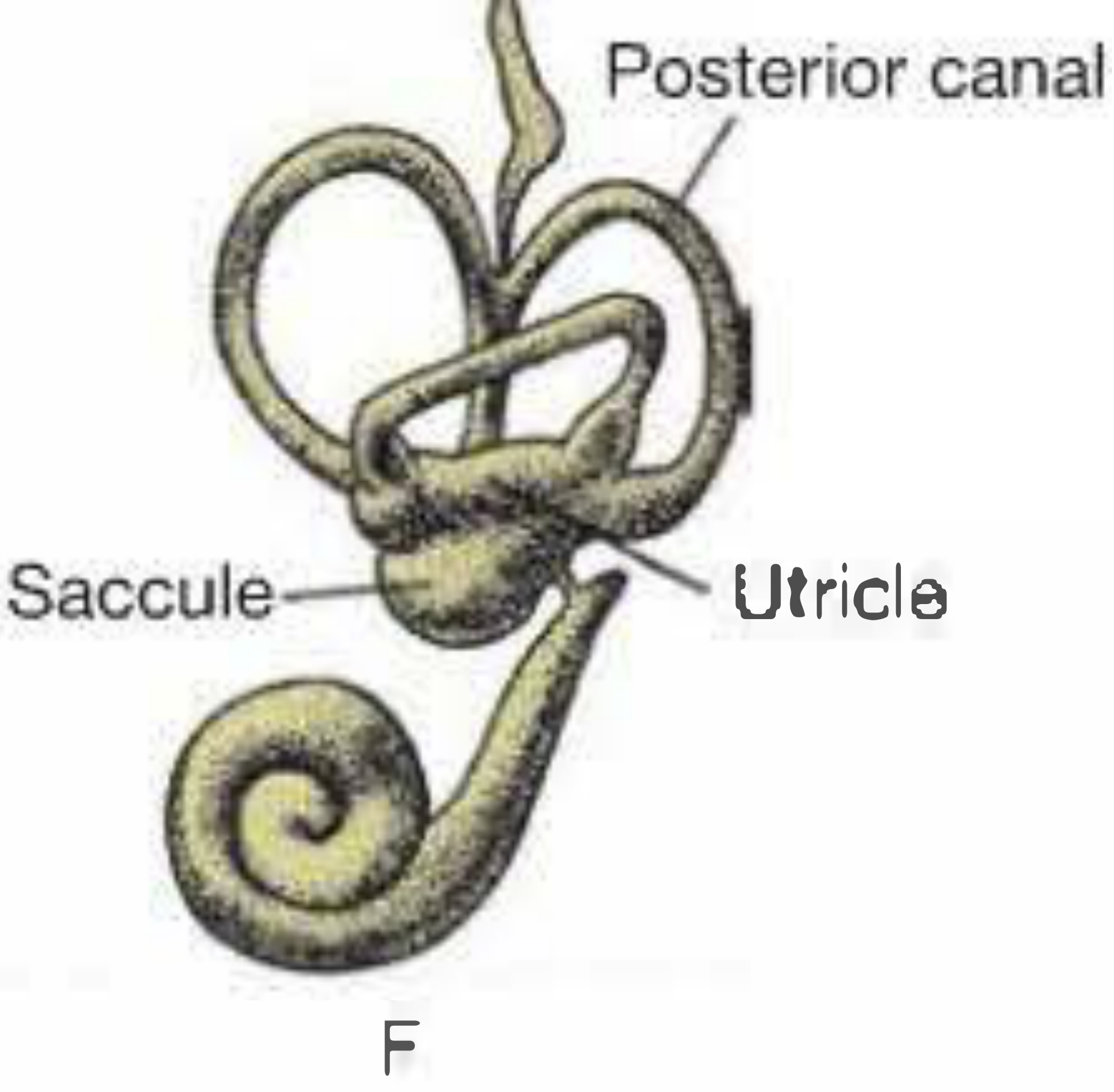
- The cochlear duct has extended from the saccule and completed 1 turn
By week 8: The cochlear duct completes its full 2.5 turns
Stage 3 - Sensory Differentiation (Weeks 8-20)
Weeks 8-16: The labyrinth approaches its adult configuration
- Cristae ampullares of the semicircular ducts develop hair cells and gelatinous cupula
- Maculae of the otolithic organs (utricle and saccule) develop hair cells and otolithic membranes
- The proximal endolymphatic sac develops a rugose epithelium (resorptive/immune function)
- The cochlear duct changes from a circular to triangular outline as the basal turn begins differentiating into the organ of Corti
By week 20:
- The superior semicircular duct reaches adult size; posterior and lateral follow
- All cristae ampullares are fully differentiated
- The endolymphatic duct begins to develop a bend as it is dragged inferiorly/laterally by growth of the sigmoid sinus
- The organ of Corti is sufficiently differentiated that the fetus can respond to fluid-borne sounds
By week 25:
- Organ of Corti approximates adult structure
- Full 2.5-coil outline of the membranous labyrinth is established
Stage 4 - Bony Labyrinth (Otic Capsule) Formation
| Event | Timing |
|---|---|
| Mesenchyme surrounding otocyst chondrifies | Weeks 5-8 |
| Cartilaginous otic capsule formed | ~Week 8 |
| Perilymphatic spaces form (dedifferentiation of cartilage) | Weeks 8-16 |
| Ossification begins | ~Week 16 |
| Ossification complete, dense petrous bone formed | ~Week 23 |
- The perilymphatic spaces arise by selective resorption (dedifferentiation) of the cartilaginous otic capsule - this does NOT occur where nerves enter sensory regions
- Ossification proceeds from multiple centers that fuse without suture lines, forming the exceptionally dense petrous bone
- The cochlear aqueduct develops to connect the scala tympani to the posterior cranial fossa (CSF-perilymph communication)
- At the oval window, part of the otic capsule becomes the stapes footplate and annular ligament
Summary Timeline
| Week | Key Event |
|---|---|
| 3 (day 22-23) | Otic placode appears |
| 4 | Otic pit forms; endolymphatic appendage appears |
| 4-5 | Otocyst separates from surface |
| 6 | Semicircular duct lumina formed; cochlear duct 1 turn |
| 8 | Cochlear duct completes 2.5 turns |
| 8-16 | Sensory neuroepithelium differentiates; otic capsule ossification begins (week 16) |
| 20 | Fetus responds to sound; superior SCC reaches adult size |
| 25 | Organ of Corti adult-like; membranous labyrinth full size |
Clinical Relevance of Developmental Timing
- Mondini malformation: Cochlear development arrested at ~7 weeks (1.5 turns instead of 2.5) - associated with enlarged vestibular aqueduct
- Michel aplasia: Complete failure of otocyst development - total absence of inner ear structures
- Enlarged vestibular aqueduct (EVA): Abnormal endolymphatic duct/sac development; most common inner ear malformation causing sensorineural hearing loss
- Rubella embryopathy: Damage at 6-10 weeks targets cochlear hair cells before full differentiation
- Superior SCC dehiscence: Failure of otic capsule bone formation over the superior canal
Sources: Shambaugh - Surgery of the Ear, pp. 33-35; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, p. 585
This is a shared conversation. Sign in to Orris to start your own chat.