Investigation for hyperaldostronism
Reading File
Finding Sources
Finding Sources
Searching PubMed
"primary aldosteronism" AND "diagnosis"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is a structured, evidence-based answer:
Investigation of Hyperaldosteronism
Hyperaldosteronism (primary/secondary) is the most common form of secondary hypertension. Investigation follows a structured three-stage approach: screen → confirm → subtype.
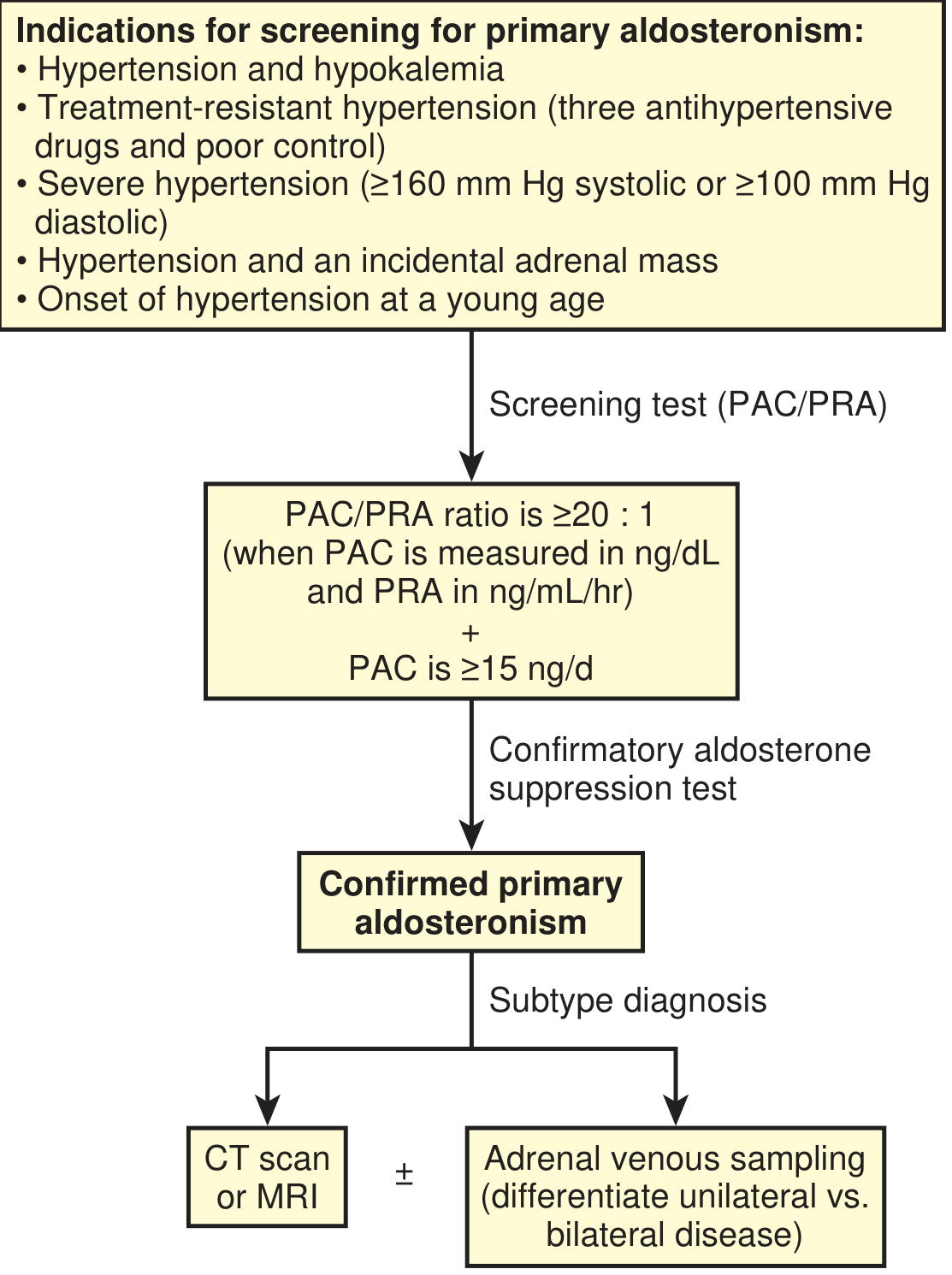
Stage 1: When to Screen (Indications)
Screen any hypertensive patient with:
| Indication |
|---|
| Hypertension + spontaneous or diuretic-induced hypokalemia |
| Treatment-resistant hypertension (≥3 antihypertensives + poor control) |
| Severe hypertension (≥160/100 mmHg) |
| Hypertension + incidental adrenal mass |
| Young-onset hypertension |
| Hypertension with a family history of PA or early stroke (<40 years) |
| Sleep-disordered breathing with hypertension |
Note: Hypokalemia is present in <50% of cases — eukalemic PA is now the majority. — Textbook of Family Medicine 9e
Stage 2: Screening Test — Aldosterone-to-Renin Ratio (ARR)
Test: Morning, ambulatory, paired plasma aldosterone concentration (PAC) and plasma renin activity (PRA) or plasma renin concentration (PRC).
| Parameter | Threshold for Positive Screen |
|---|---|
| PAC/PRA ratio (ARR) | ≥20–30 (ng/dL ÷ ng/mL/hr) |
| PAC (to reduce false positives) | ≥15 ng/dL |
| PAC <10 ng/dL | PA is rare |
Key pre-test conditions:
- Correct hypokalemia before testing (hypokalemia falsely lowers aldosterone)
- Can be performed on most antihypertensives except mineralocorticoid receptor antagonists (spironolactone, eplerenone) — stop ≥6 weeks before
Drugs causing false-positive ARR (raise ARR):
- Beta-blockers, central α₂-agonists (e.g., clonidine), NSAIDs, direct renin inhibitors, chronic kidney disease, sodium loading
Drugs causing false-negative ARR (lower ARR):
- Diuretics, ACE inhibitors, ARBs, dihydropyridine CCBs, sodium depletion
Safe drugs during screening (minimal effect on ARR): sustained-release verapamil, hydralazine, peripheral α₁-blockers (e.g., doxazosin)
— Brenner and Rector's The Kidney, Table 46.7
Stage 3: Confirmatory Tests
At least one confirmatory test is required before proceeding to imaging/AVS. Choose based on patient suitability:
| Test | Protocol | Positive Criterion |
|---|---|---|
| IV Saline Loading | 2 L 0.9% NaCl over 4 hours | PAC >10 ng/dL post-infusion (indeterminate 5–10) |
| Oral Sodium Loading | High-Na diet (~6 g/day × 3–5 days | 24-hr urinary aldosterone >12–14 µg/day |
| Fludrocortisone Suppression Test (FST) | Fludrocortisone 0.1 mg q6h × 4 days | Standing PAC >6 ng/dL with suppressed renin & cortisol |
| Captopril Challenge Test | 25–50 mg oral captopril; PAC at 0, 1, 2 hours | PAC remains elevated/unchanged from baseline |
Saline loading is contraindicated in heart failure, CKD, or uncontrolled hypertension. — Brenner and Rector's The Kidney
Stage 4: Subtype Differentiation — Imaging + AVS
Once PA is confirmed biochemically:
CT Adrenals (First-line Imaging)
- Detects large masses (>4 cm) suggesting adrenal carcinoma
- APA: typically small (<2 cm), hypodense, unilateral
- Idiopathic hyperaldosteronism (bilateral): normal or mildly nodular adrenals
- MRI offers no advantage over CT
- Limitations: CT sensitivity 78%, specificity 75% for lateralization — misses microadenomas and may misclassify bilateral disease
Adrenal Venous Sampling (AVS) — Gold Standard for Lateralization
- Sensitivity 95%, specificity 100% for detecting unilateral aldosterone production
- Recommended by Endocrine Society for most surgical candidates
- Performed at 8 AM with continuous cosyntropin infusion; simultaneous bilateral adrenal vein and IVC cortisol + aldosterone measured
- Cutoff: Cortisol-corrected aldosterone ratio (dominant:contralateral side) ≥4:1 = positive lateralization
When to proceed directly to adrenalectomy without AVS:
- Age <40 years + biochemically proven PA + single hypodense unilateral nodule on CT (some centres)
When to offer AVS:
- All surgical candidates >35 years
- Any case with discordance between imaging and biochemistry
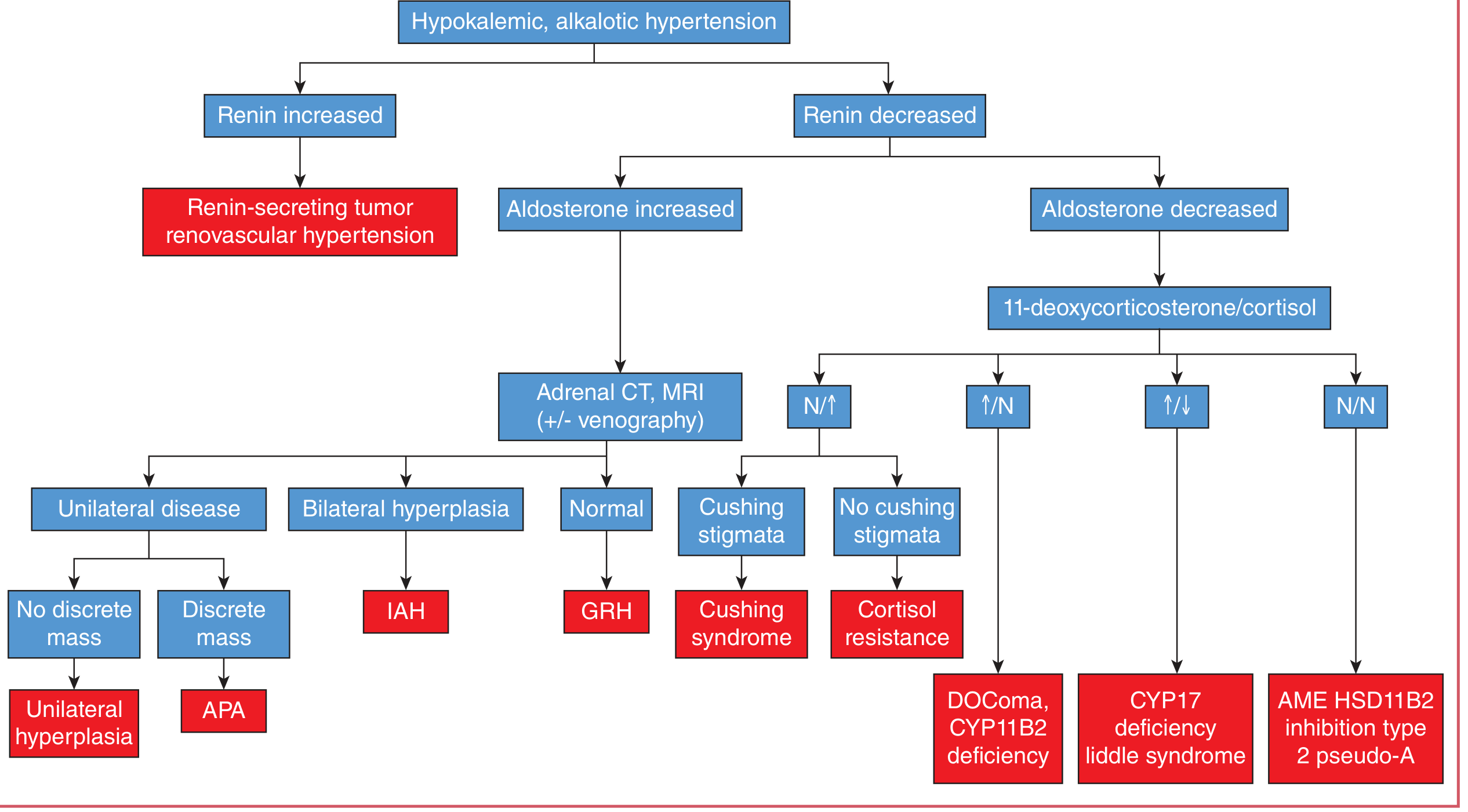
Diagnostic Flowchart
Additional / Special Investigations
| Situation | Test |
|---|---|
| Secondary hyperaldosteronism (elevated renin) | Renal Doppler/CTA for renal artery stenosis; renin-secreting tumour workup |
| Suspected familial hyperaldosteronism (age <20, family history) | Genetic testing (Southern blot or long PCR for CYP11B1/CYP11B2 chimeric gene — FH-I/GRA) |
| Suspected FH-I before genetic testing | Empiric dexamethasone suppression: aldosterone <4 ng/dL = positive |
| Distinguish APA from bilateral hyperplasia | PAC ≥100 ng/dL favours APA; <100 ng/dL favours IAH |
| Postural stimulation test (older/backup test) | Plasma aldosterone lying vs. standing: APA retains diurnal variation; IAH shows paradoxical rise with standing (accuracy ~85%) |
| Iodocholesterol scintigraphy | Limited utility (correlates with tumour size, poor for microadenomas) |
| 18-hydroxycorticosterone (8 AM recumbent) | >100 ng/dL suggests APA (less reliable) |
Subtypes & Prevalence Summary
| Subtype | Prevalence |
|---|---|
| Bilateral adrenal hyperplasia (IAH) | ~60% |
| Aldosterone-producing adenoma (Conn) | ~35% |
| Unilateral adrenal hyperplasia | ~2% |
| Familial hyperaldosteronism | <2% |
| Adrenal carcinoma | Rare |
| Ectopic aldosterone | <0.1% |
Sources: Brenner & Rector's The Kidney; Tietz Textbook of Laboratory Medicine 7e; Textbook of Family Medicine 9e; Current Surgical Therapy 14e
Recent evidence note: A 2025 Endocrine Society systematic review (PMID 40658500) supports the above stepwise approach, and a 2025 meta-analysis (PMID 40304781) highlights emerging CXCR4-targeted PET-CT as a potential localisation tool for PA, though it is not yet standard practice.
This is a shared conversation. Sign in to Orris to start your own chat.