Yeach me a surgery topic- Disorders pf pancreas in a way like you are teaching a high school child. Use images illustrations and flowcharts to make me things remember and interesting
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
Generating Image
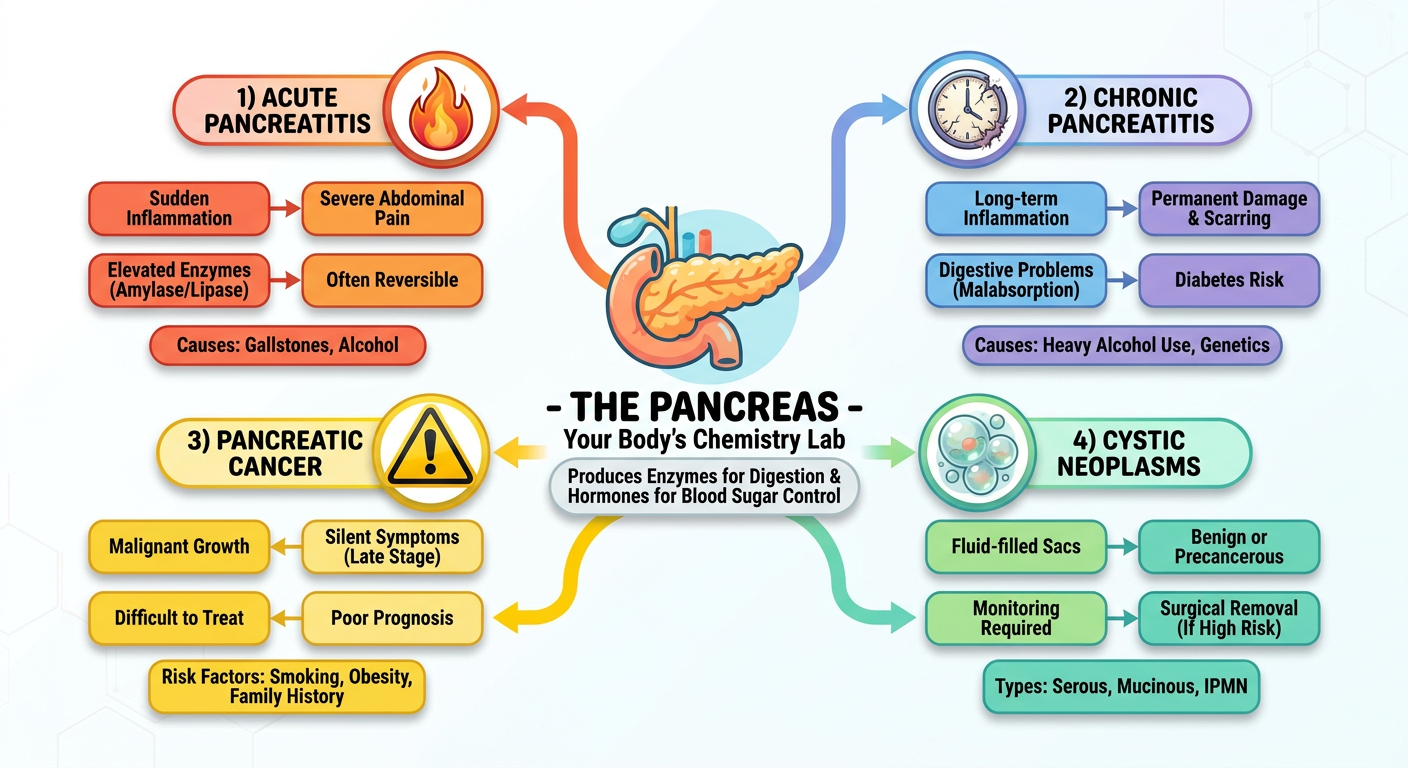
A colorful educational flowchart diagram for high school students showing the overview of pancreatic disorders. The pancreas is shown in the center labeled as "THE PANCREAS - Your Body's Chemistry Lab". Four branches spread out: 1) Acute Pancreatitis (fire/flame icon), 2) Chronic Pancreatitis (clock with scar tissue), 3) Pancreatic Cancer (warning sign), 4) Cystic Neoplasms (bubble/cyst). Each branch shows key features in simple colorful boxes. Clean, modern infographic style with bright colors on white background.
I now have everything I need. Let me write the comprehensive, fun, high-school-friendly lesson on Disorders of the Pancreas.
🥞 Disorders of the Pancreas - The Full Story!
🎓 Welcome, Student! Let's Start With the Basics
🏭 What Is the Pancreas? (Your Body's Secret Chemistry Lab)
Think of the pancreas as TWO factories packed into one organ:
| Factory | Name | Job |
|---|---|---|
| 🏭 Big Factory (98%) | Exocrine Pancreas | Makes digestive juices (enzymes) to break down food |
| 🧪 Mini Lab (2%) | Endocrine (Islets of Langerhans) | Makes hormones: insulin (lower blood sugar) & glucagon (raise blood sugar) |
The pancreas lives behind the stomach (retroperitoneal - meaning "behind the belly lining"), shaped like a tadpole with a head, body, and tail.
🔑 Key Analogy: The pancreas is like a factory that makes dangerous acid in locked containers. If those containers break open inside the factory - boom! The acid destroys the factory itself. That's basically pancreatitis!
🛡️ The Pancreas's Own Safety System (Before We Talk About Failure!)
The pancreas is actually quite smart - it stores its own enzymes in locked, inactive form (called proenzymes or zymogens). They only get "unlocked" (activated) after safely reaching the small intestine. Here's why that matters:
NORMAL:
[Locked enzymes in acinar cell] → Released into duct → Travel to intestine → Activated → Digest food ✅
PANCREATITIS:
[Locked enzymes] → Something goes WRONG → Enzymes activate INSIDE the pancreas → Pancreas digests ITSELF ❌
🔥 DISORDER #1: ACUTE PANCREATITIS
"The Pancreas Attacks Itself!"
What Is It?
Acute pancreatitis is when the pancreas suddenly becomes inflamed and starts self-digesting. The good news: if you fix the cause, the pancreas can completely recover.
🎯 The Two Big Causes (Remember: GET SMASHED)
💡 Memory Trick: Gallstones and Ethanol (alcohol) = 80% of all cases!
| Cause | How It Causes Pancreatitis |
|---|---|
| 🪨 Gallstones | A stone blocks the "exit door" (ampulla of Vater), backing up enzymes |
| 🍺 Alcohol | Directly injures acinar cells; alters enzyme activation |
| 💊 Drugs | Certain medications (thiazides, azathioprine) |
| 🦠 Infections | Mumps virus, coxsackievirus |
| 🏋️ Trauma | Direct injury to the abdomen |
| 🧬 Genetics | Mutations in PRSS1 (trypsinogen gene) or SPINK1 (trypsin inhibitor gene) |
| ⬆️ Hypertriglyceridemia | Very high blood fats (>1000 mg/dL) |
⚙️ How It Works - The Pathogenesis Flowchart
Here's the ACTUAL textbook diagram from Robbins Pathology showing exactly how acute pancreatitis develops - 3 pathways, all converging on one disaster:
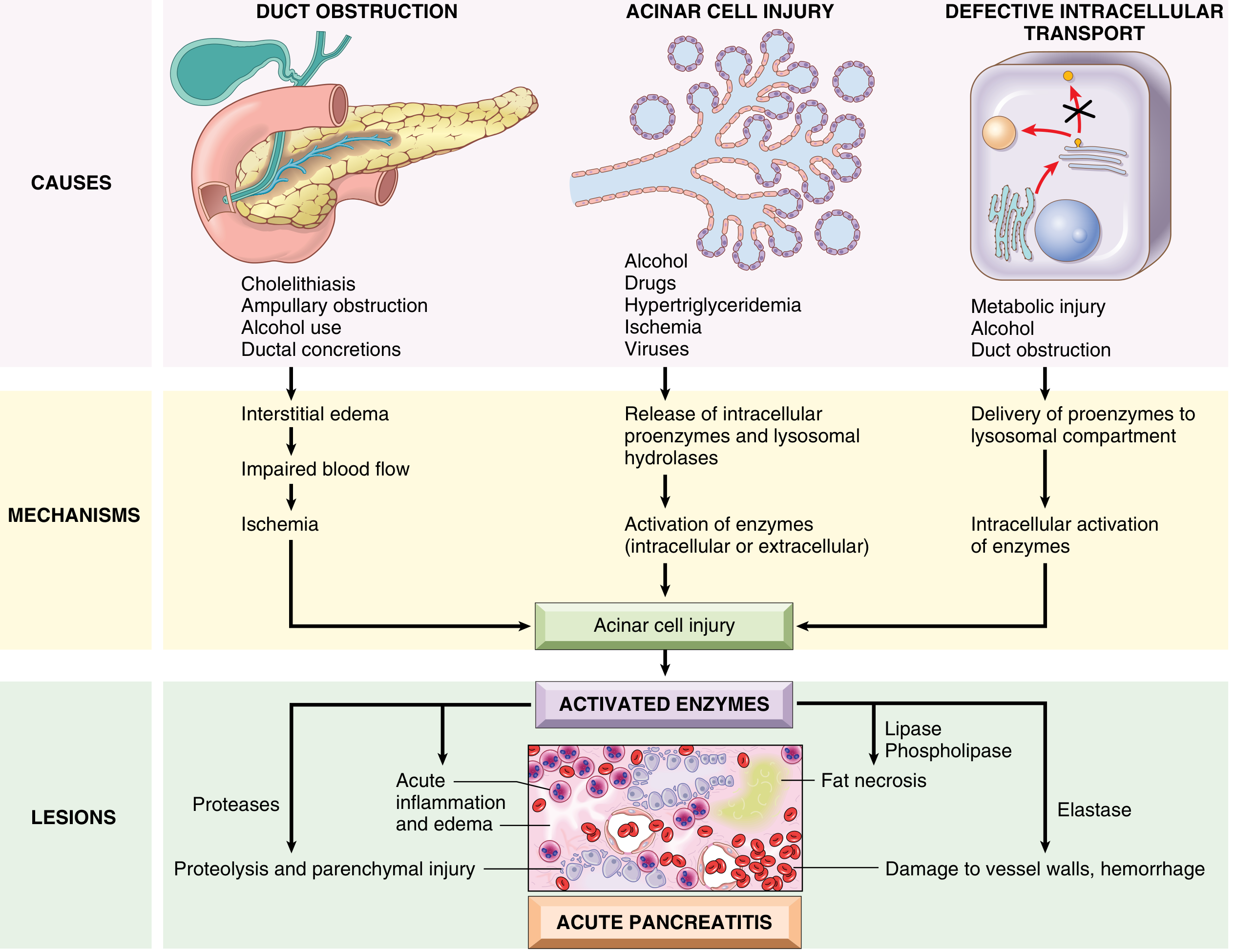
In plain English:
PATH 1: Blocked Duct
Gallstone blocks duct → Pressure builds up → Enzymes spill into tissue → FAT NECROSIS 🔥
PATH 2: Direct Cell Injury
Alcohol/drugs/virus → Damages acinar cells directly → Enzymes leak out → Inflammation cascade 🔥
PATH 3: Wrong Packaging
Proenzymes end up in lysosomes (wrong bag) → Prematurely activated → Self-digestion begins 🔥
ALL THREE PATHS → Activated Trypsin → Destroys everything:
- PROTEASES → Destroy protein (tissue death)
- LIPASE → Destroy fat (fat necrosis = chalky white spots)
- ELASTASE → Destroy blood vessels (hemorrhage = bleeding)
🩺 Signs & Symptoms
⬆️ Serum AMYLASE & LIPASE
(lab test diagnosis)
↑
ACUTE EPIGASTRIC PAIN ──────────────────── NAUSEA/VOMITING
(radiates to back,
like a belt tightening)
↓
WORSE AFTER EATING
(especially fatty food)
↓
In severe cases:
- CULLEN'S SIGN: bruising around the navel 👁
- GREY TURNER'S SIGN: bruising on flanks
(Both = internal bleeding from destroyed vessels)
🏥 What Happens to the Pancreas? (Morphology)
Mild cases: Edema + small white chalky spots = fat necrosis (lipase digesting fat, calcium deposits form - "saponification")
Severe cases: The whole pancreas turns into a bloody, necrotic mess = hemorrhagic pancreatitis - this is life-threatening!
🫧 Complications: The Pancreatic Pseudocyst
Sometimes, after acute pancreatitis, fluid and debris collect into a sac. It's called a pseudocyst because it has NO epithelial lining (a real cyst does). Look at what it looks like:
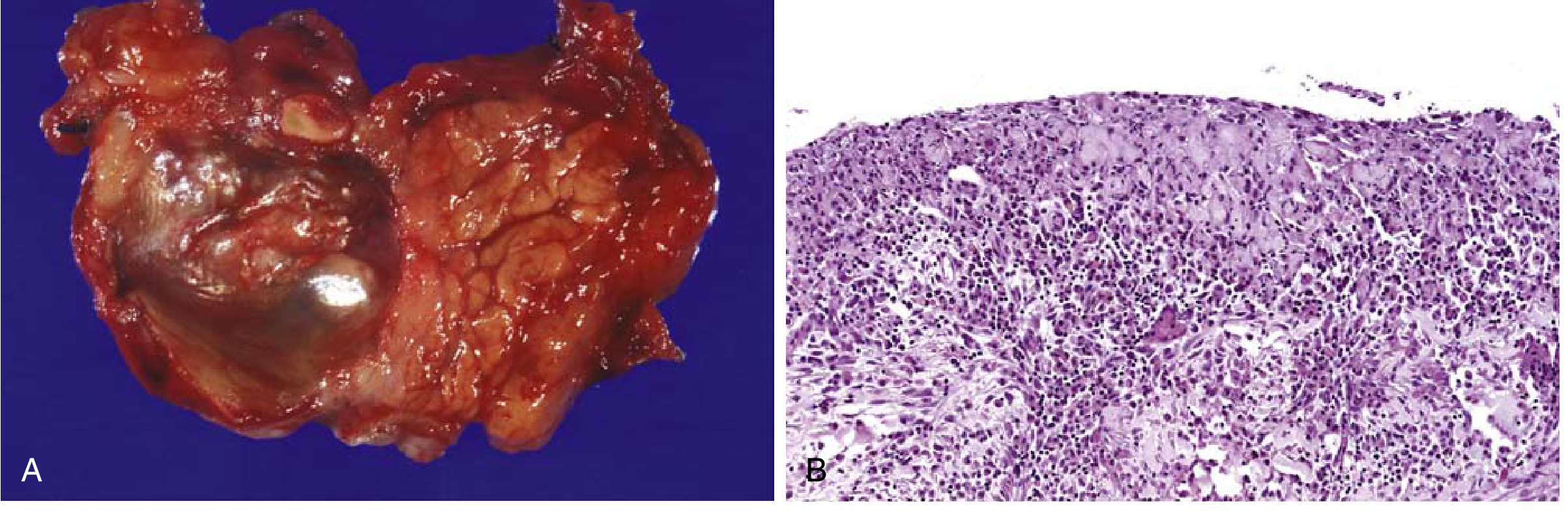
🔑 Remember: "PSEUDO" = FAKE. A pseudocyst has no epithelial lining - just fibrin and granulation tissue!
⏳ DISORDER #2: CHRONIC PANCREATITIS
"The Slow Burn That Scars Everything"
What Is It?
Unlike acute pancreatitis (which is reversible), chronic pancreatitis causes permanent destruction of the pancreas. The exocrine tissue gets replaced by scar tissue (fibrosis). Eventually, the endocrine islets also get destroyed → diabetes!
Comparison Table:
| Feature | Acute Pancreatitis | Chronic Pancreatitis |
|---|---|---|
| Reversibility | ✅ Reversible | ❌ Irreversible |
| Scarring | No | Yes (fibrosis) |
| Diabetes | Rare | Common (late stage) |
| Main cause | Gallstones / Alcohol | Alcohol (chronic) |
| Enzyme levels | Very HIGH | May be NORMAL (too scarred to produce!) |
| Calcifications | Absent | ✅ Calcium deposits in duct (on CT!) |
🧬 Causes of Chronic Pancreatitis
Most Common: Chronic Alcohol Use 🍺 (especially middle-aged men)
Others:
- Genetic: CFTR mutations (same gene as cystic fibrosis!)
PRSS1, SPINK1 mutations
- Autoimmune Pancreatitis (IgG4-positive plasma cells infiltrate)
- Ductal obstruction
- 40% = Idiopathic (unknown cause)
🔬 What It Looks Like Under the Microscope:
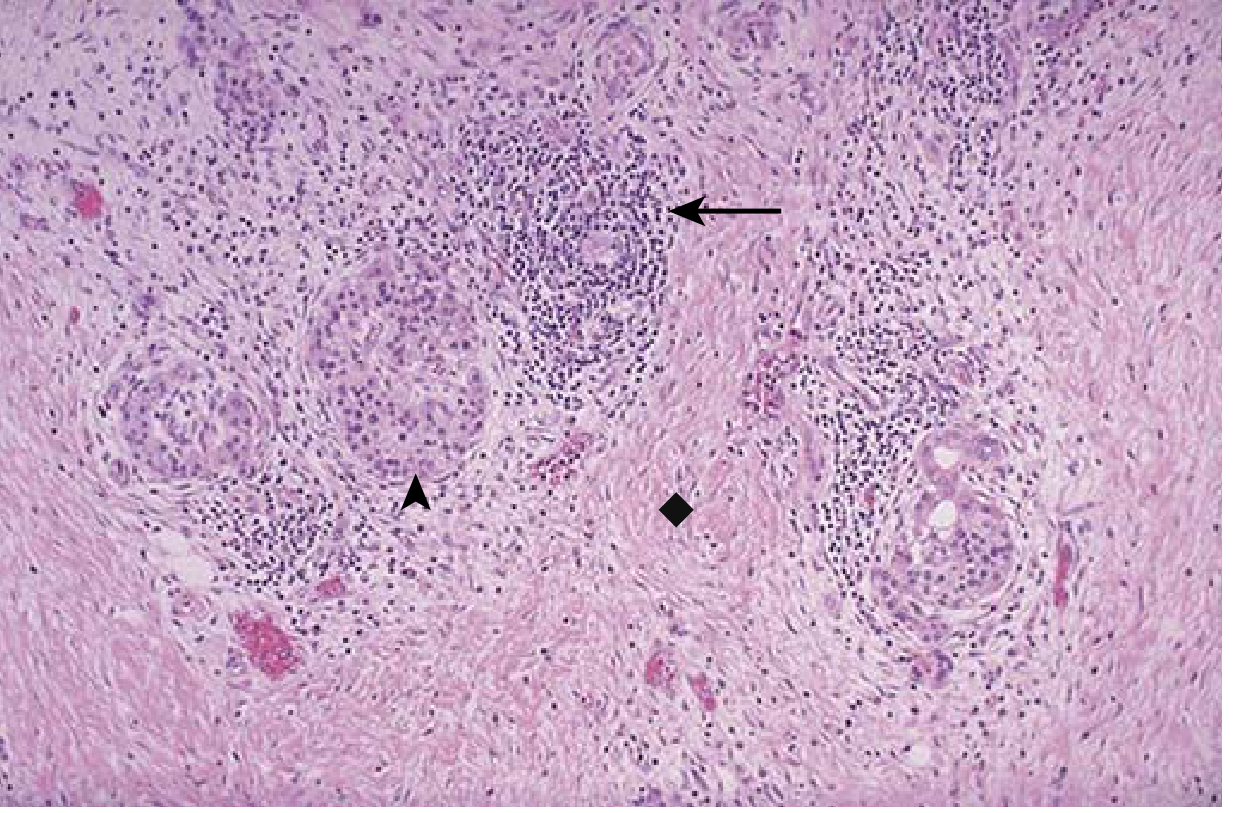
Notice: The acini (enzyme-making cells) are GONE, replaced by collagen scar tissue. Only a few islets of Langerhans survive - and eventually they go too!
🩺 Symptoms
Chronic Abdominal Pain → (dull, recurring, relieved by leaning forward)
↓
Steatorrhea → ("fatty stools" - foul-smelling, greasy = can't digest fats)
↓
Weight Loss → (can't absorb nutrients = malabsorption)
↓
Vitamin D deficiency → Osteoporosis
↓
Diabetes → (when islets finally destroyed)
↓
❗ RISK OF PANCREATIC CANCER ❗
(40% lifetime risk with PRSS1 hereditary type!)
🦀 DISORDER #3: PANCREATIC CANCER
"The Silent Killer"
Why Is It So Deadly?
Pancreatic cancer has one of the worst prognoses of all cancers because:
- The pancreas is hidden deep behind the stomach (no easy physical exam)
- Symptoms appear only LATE (when cancer has spread)
- Less than 20% are resectable (surgically removable) at diagnosis
🗺️ Where Does It Arise?
- 60% - Head of pancreas (most common!)
- 15% - Body
- 5% - Tail
- 20% - Diffuse
🔑 Why does location matter? Cancer in the HEAD obstructs the bile duct → causes JAUNDICE (yellow skin/eyes). Cancer in the TAIL stays silent for much longer!
🧬 How Does Pancreatic Cancer Develop? (Step by Step)
This is one of the coolest diagrams in all of pathology - watch the normal duct cells slowly transform into cancer:
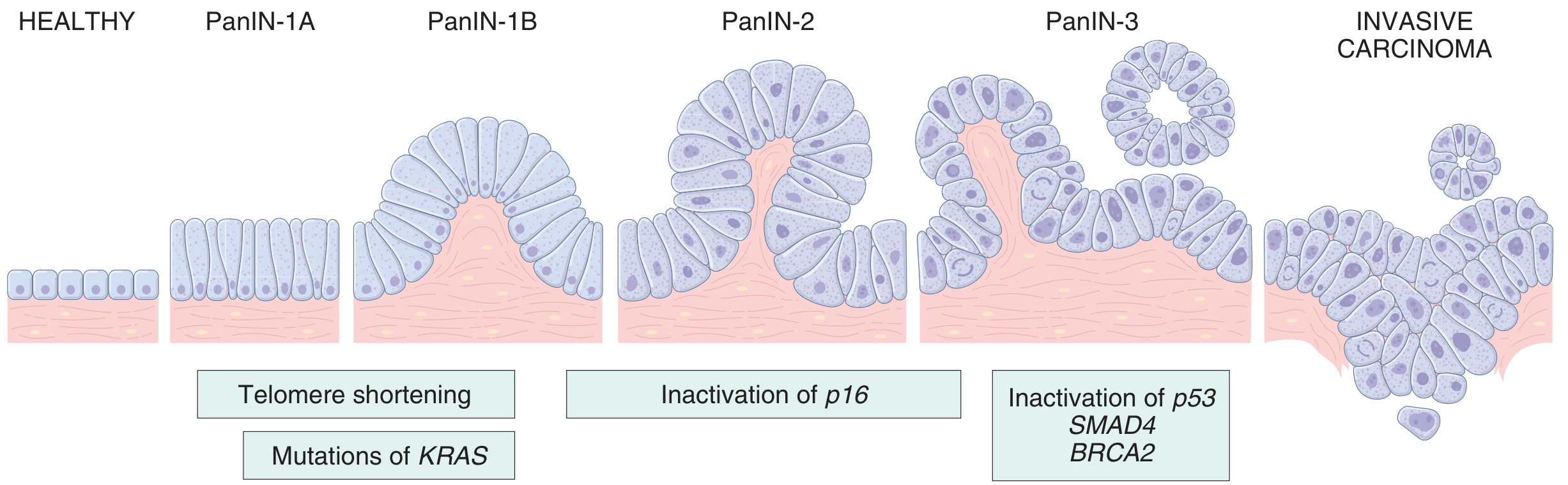
Reading the diagram:
HEALTHY DUCT
↓ (KRAS mutation + telomere shortening)
PanIN-1A → PanIN-1B [cells start piling up]
↓ (p16 gene deleted)
PanIN-2 [cells look abnormal]
↓ (p53, SMAD4, BRCA2 mutations)
PanIN-3 [cells very abnormal - "carcinoma in situ"]
↓
INVASIVE CARCINOMA [cancer breaks through - the point of no return]
The Key Mutations (just remember these 4!):
| Gene | What It Normally Does | What Mutation Does |
|---|---|---|
| KRAS (90%!) | Controls cell growth signal | Gets stuck in "ON" position → cells grow without stop |
| p16/CDKN2A (95%) | Applies the cell cycle "brake" | Brake removed → cells divide faster |
| TP53 (70-75%) | DNA guardian / apoptosis trigger | Guardian gone → broken cells don't die |
| SMAD4 (55%) | Transmits "stop growing" signal | Signal lost → cells ignore "stop" messages |
🔍 What Pancreatic Cancer Looks Like:
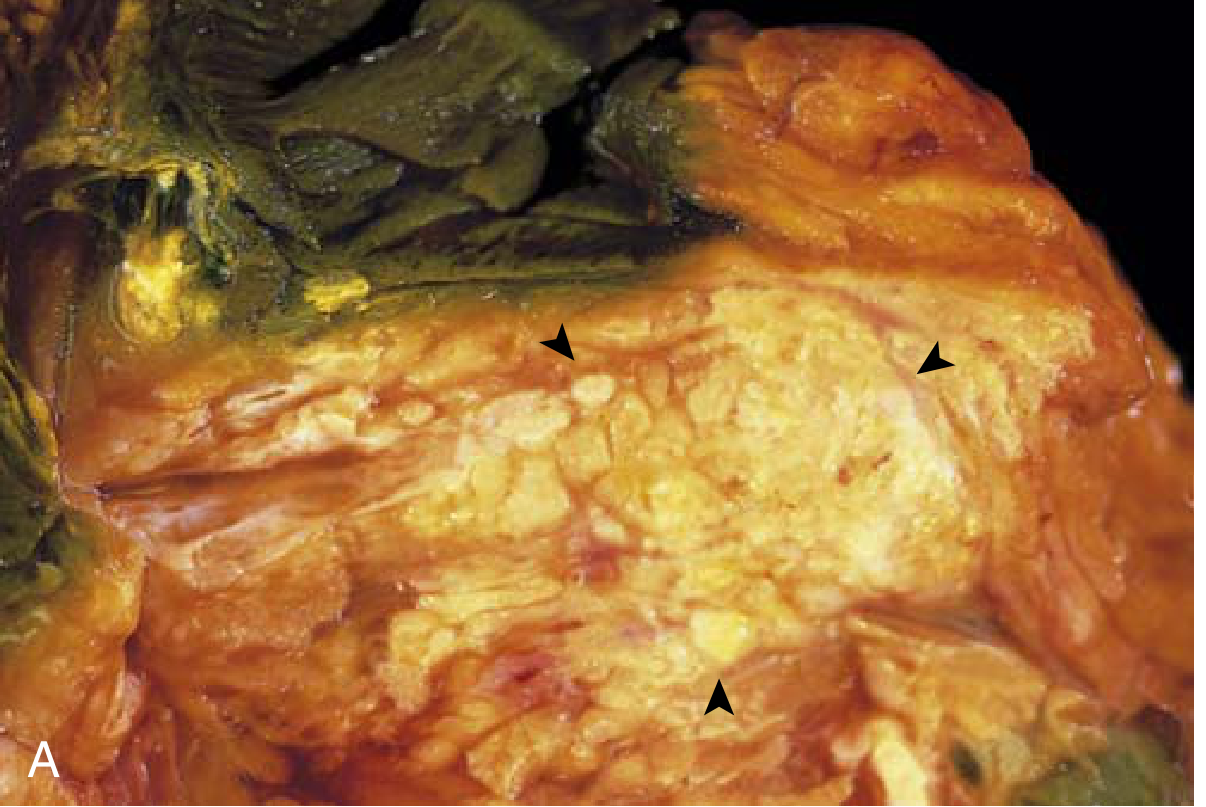
Notice the hard, gray-white, stellate (star-shaped) mass - and the green bile duct showing total obstruction!
🩺 Symptoms (Why They Appear So Late!)
⚠️ CANCER IS GROWING FOR MONTHS/YEARS SILENTLY...
↓
Eventually compresses surrounding structures:
HEAD CANCER: BODY/TAIL CANCER:
- Obstructive Jaundice - Back pain (invades nerves)
- Dark urine - Weight loss
- Pale stools - New-onset DIABETES
- Pruritus (itching) (may be first symptom!)
↓
Advanced stage: Trousseau Syndrome
(migratory blood clots = cancer releasing clotting factors)
↓
Weight loss, anorexia, weakness
⚠️ Risk Factors:
🚬 SMOKING → doubles the risk (strongest environmental factor!)
🍺 Chronic pancreatitis
🩸 Diabetes (both a cause AND a result!)
🧬 Genetics: BRCA2 mutation, Lynch syndrome
👴 Age: 80% of cases between ages 60-80
💉 Tumor Marker: CA 19-9
(Not sensitive/specific enough for screening, but used to monitor treatment response)
🔧 Treatment Options:
- Whipple procedure (Pancreaticoduodenectomy) - for resectable head cancers - major surgery removing head of pancreas + duodenum + part of bile duct
- Chemotherapy (FOLFIRINOX or Gemcitabine-based) - for non-resectable
- Overall 5-year survival: ~12% (improving slowly with newer agents)
🫧 DISORDER #4: CYSTIC NEOPLASMS OF THE PANCREAS
"Bubbles with Different Personalities!"
There are THREE main types. Think of them as a traffic light:
🟢 GREEN (BENIGN) 🟡 YELLOW (WATCH OUT!) 🔴 RED (DANGEROUS!)
Serous Cystadenoma Mucinous Cystic Neoplasm Pancreatic Adenocarcinoma
+ IPMN (can become cancer) (already covered above)
1. 🟢 Serous Cystadenoma - "The Honeycomb"
- Looks like: A honeycomb of tiny cysts filled with CLEAR watery fluid
- Who gets it: Mostly older women (F:M = 2:1), detected by accident
- Genetics: VHL gene mutation
- Behavior: Almost always BENIGN - surgery is curative!
- Lining cells: Cuboidal cells (small, square cells - no atypia)
2. 🟡 Mucinous Cystic Neoplasm - "The Slimy One"
- Looks like: Large cysts filled with THICK, STICKY MUCIN
- Who gets it: Women, tail of pancreas
- Behavior: PRECANCEROUS - can progress to cancer if not removed!
- Lining cells: Columnar mucinous epithelium + "ovarian-type" stroma underneath
- Treatment: Surgical resection recommended
3. 🟡 IPMN (Intraductal Papillary Mucinous Neoplasm) - "The Duct Clogger"
- What it is: Mucin-secreting tumor that grows INSIDE the pancreatic duct, forming finger-like (papillary) projections
- Behavior: Also PRECANCEROUS - risk of progression
- Feature: Can be seen as a dilated main pancreatic duct on imaging
📊 MASTER OVERVIEW CHART
🧠 QUICK MEMORY TRICKS
| Disease | Memory Hook |
|---|---|
| Acute pancreatitis causes | "GET SMASHED" - Gallstones, Ethanol, Trauma, Steroids, Mumps, Autoimmune, Scorpion, Hyperlipidemia, ERCP, Drugs |
| Cullen's sign | CULlen = navel (C = circle = belly button) |
| Grey Turner's sign | TURNER = flanks (sides) |
| Pseudocyst | PSEUDO = FAKE - no epithelial lining |
| Pancreatic cancer location | "60-15-5" = Head-Body-Tail |
| Serous vs Mucinous | Serous = CLEAR = SAFE; Mucin = THICK = TRICKY |
| KRAS | Think of KRAS as a stuck accelerator pedal on a car - can't turn OFF |
🔄 FINAL FLOWCHART: How Acute Pancreatitis Leads to Everything Else
GALLSTONES / ALCOHOL
↓
ACUTE PANCREATITIS
↙ ↘
Resolves Recurs repeatedly
(recovery) ↓
CHRONIC PANCREATITIS
↙ ↘ ↘
Pain/ Exocrine Endocrine
disability insufficiency destruction
↓ ↓ ↓
Steatorrhea Malnutrition DIABETES
↓
(long term risk)
↓
PANCREATIC CANCER
(especially with
PRSS1 mutations)
📝 EXAM RAPID REVIEW
| Question | Answer |
|---|---|
| Most common cause of acute pancreatitis? | Gallstones (then alcohol) |
| Key lab finding in acute pancreatitis? | ↑ Serum amylase + lipase |
| What is a pseudocyst? | Fluid collection with NO epithelial lining |
| Cause of fat necrosis + calcium deposits? | Lipase activity (saponification) |
| Most common cause of chronic pancreatitis? | Chronic alcohol use |
| What does chronic pancreatitis look like on CT? | Calcifications in pancreatic duct |
| What's the most common mutation in pancreatic cancer? | KRAS (>90% of cases) |
| Where does 60% of pancreatic cancer arise? | Head of the pancreas |
| Why does head cancer cause jaundice? | Obstructs the common bile duct |
| What's Trousseau syndrome? | Migratory thrombophlebitis in cancer |
| Most benign cystic neoplasm? | Serous cystadenoma |
| Precancerous cystic neoplasms? | Mucinous cystic neoplasm + IPMN |
| CA 19-9 is used for? | Monitoring pancreatic cancer (not screening) |
| 5-year survival of pancreatic cancer? | ~12% |
Sources: Robbins & Kumar Basic Pathology, Current Surgical Therapy 14e, Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.