Give me long answer in Myocardial infarction like different types , different artery blocks everything and also include the ECGs
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
ECG ST elevation myocardial infarction STEMI leads
Searching Images
coronary artery territories myocardial infarction diagram
Reading File
Reading File
Searching Images
inferior STEMI ECG II III aVF ST elevation right coronary artery
I now have comprehensive material. Let me compile the full answer with ECG images:
Myocardial Infarction — Comprehensive Review
1. Definition & Overview
Myocardial infarction (MI), commonly called a "heart attack," is necrosis of cardiac muscle resulting from ischemia. The 2018 joint U.S./European Cardiology task force defines it as "the presence of acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia."
The major underlying cause is atherosclerotic coronary artery disease (CAD). About 10% of MIs occur before age 40, and 45% before age 65. Men are at greater risk, though the gap narrows after menopause in women. — Robbins & Kumar Basic Pathology
2. Types of Myocardial Infarction
A. By Depth of Injury
| Type | Description | Classic ECG Marker |
|---|---|---|
| Transmural (STEMI) | Full-thickness necrosis through all myocardial layers | ST elevation → Q waves |
| Subendocardial (NSTEMI/Non-Q-wave) | Inner layers only; incomplete occlusion | ST depression / T-wave changes, no persistent ST elevation |
STEMI results from acute, total occlusion of an epicardial coronary artery. NSTEMI arises from partial occlusion — subtotal thrombosis or transient total occlusion that restores before full-thickness necrosis occurs. — Washington Manual of Medical Therapeutics
B. Universal Classification (Thygesen 2018) — MI Types 1–5
| Type | Mechanism |
|---|---|
| Type 1 | Spontaneous MI from atherosclerotic plaque rupture/erosion with thrombosis |
| Type 2 | Secondary to supply-demand mismatch (e.g., tachyarrhythmia, spasm, severe anemia, hypotension) — no plaque rupture |
| Type 3 | Sudden cardiac death before biomarkers can be drawn |
| Type 4a | Periprocedural MI related to PCI |
| Type 4b | MI related to in-stent thrombosis |
| Type 5 | MI related to CABG surgery |
C. By Underlying Mechanism (Rare Causes)
In ~10% of MIs, transmural infarction occurs without obstructive atherosclerosis. Causes include:
- Coronary artery vasospasm (Prinzmetal's angina)
- Embolism from mural thrombi (e.g., in atrial fibrillation) or valve vegetations
- Vasculitis, amyloid deposition, sickle cell disease (small intramyocardial arterioles)
- Spontaneous coronary artery dissection (SCAD) — more common in young women
- Takotsubo syndrome (stress cardiomyopathy)
3. Pathogenesis — Sequence of Events
The typical sequence (Robbins):
- An atheromatous plaque is eroded or suddenly disrupted by endothelial injury, intraplaque hemorrhage, or mechanical forces — exposing subendothelial collagen and necrotic plaque contents.
- Platelets adhere, aggregate, and release thromboxane A₂, ADP, and serotonin → further platelet aggregation + vasospasm.
- Tissue factor activates coagulation → growing thrombus.
- The enlarging thrombus completely occludes the coronary artery within minutes.
Angiography within 4 hours of MI shows coronary thrombosis in ~90% of cases. — Robbins & Kumar Basic Pathology
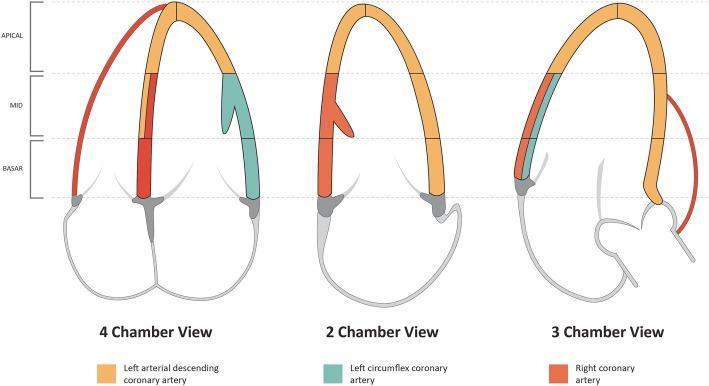
4. Coronary Artery Territories & MI Location
Each coronary artery supplies a distinct myocardial territory. Blockage produces a characteristic infarct pattern.
The Three Major Coronary Arteries
| Artery | Territory Supplied | Infarct Type |
|---|---|---|
| Left Anterior Descending (LAD) | Anterior LV wall, anterior septum, apex, RBB | Anterior / Anteroseptal / Anterolateral MI |
| Right Coronary Artery (RCA) | Inferior LV wall, posterior septum, RV, SA & AV nodes (in ~90%) | Inferior MI; ± RV infarction; ± heart block |
| Left Circumflex (LCx) | Lateral & posterior LV wall | Lateral / Inferolateral / Posterior MI |
| Left Main (LMCA) | Most of the LV (supplies LAD + LCx) | Massive anterior + lateral — cardiogenic shock |
5. ECG Changes — The Electrical Basis
The three major ECG abnormalities in acute MI (Ganong's Physiology):
| Defect in Infarcted Cells | Current Flow | ECG Change in Overlying Leads |
|---|---|---|
| Rapid repolarization (accelerated K⁺ channel opening) | Out of infarct | ST elevation |
| Decreased resting membrane potential (K⁺ loss) | Into infarct | TQ depression → manifested as ST elevation |
| Delayed depolarization | Out of infarct | ST elevation |
The net result: ST-segment elevation in leads overlying the infarcted area, with reciprocal ST depression in opposite leads. After days to weeks, the dead muscle becomes electrically silent → pathological Q waves appear.
Evolutionary ECG Changes in STEMI
| Time After Onset | ECG Finding |
|---|---|
| Minutes–hours | Hyperacute T waves (tall, broad, peaked) |
| Hours | ST elevation (convex/tombstone shape) |
| 6–24 hours | Q waves begin to appear |
| Days | ST elevation normalizes; T-wave inversions |
| Weeks–months | Persistent Q waves (scar); T waves may normalize |
6. ECG Localization by Infarct Territory
(From Tintinalli's Emergency Medicine, Table 49-4)
| Infarct Location | ST Elevation in These Leads | Culprit Artery |
|---|---|---|
| Anteroseptal | V₁, V₂ (± V₃) | Proximal LAD |
| Anterior | V₁–V₄ | LAD |
| Anterolateral | V₁–V₆, I, aVL | Proximal LAD |
| High Lateral | I, aVL | LCx or 1st Diagonal |
| Lateral | I, aVL, V₅, V₆ | LCx |
| Inferior | II, III, aVF | RCA (90%) or LCx (10%) |
| Inferolateral | II, III, aVF, V₅, V₆ | LCx or RCA |
| True Posterior | Tall R in V₁–V₂ (mirror image); ST elevation V₇–V₉ | RCA posterior descending or LCx |
| Right Ventricular (RV) | II, III, aVF + ST elevation V₃R–V₄R | Proximal RCA |
| Left Main (LMCA) | ST elevation aVR > V₁; diffuse ST depression | LMCA or severe multivessel |
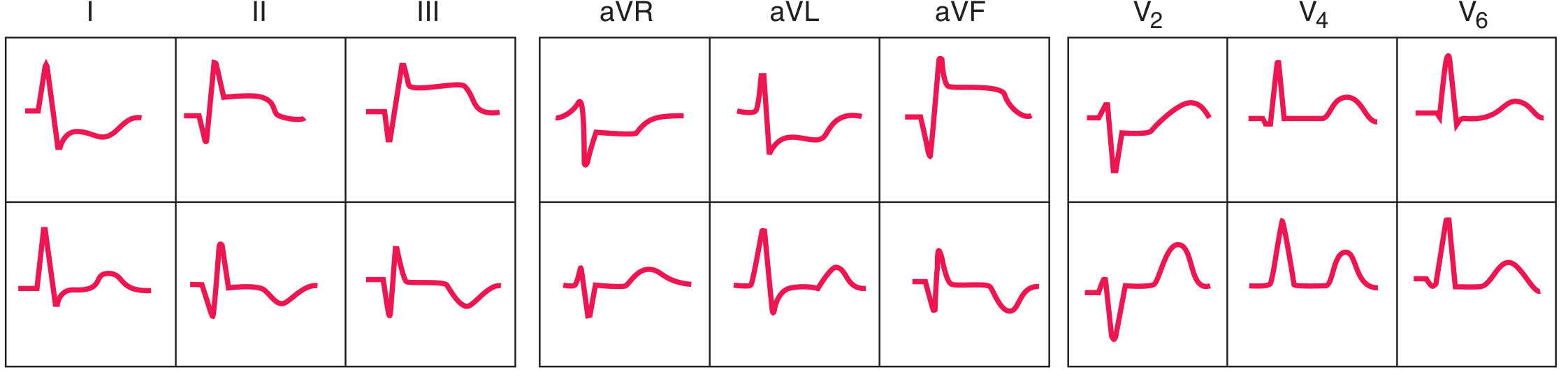
7. ECG Images
Anterior STEMI (LAD Occlusion)
Classic tombstone ST elevation in V₂–V₄, ± leads I and aVL. Reciprocal depression in II, III, aVF.
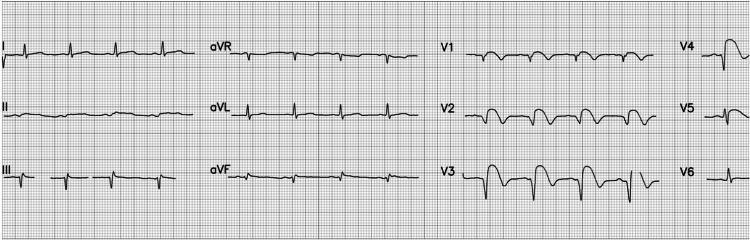
Anterolateral STEMI (Proximal LAD)
ST elevation V₁–V₆, leads I and aVL. Reciprocal depression in II, III, aVF.

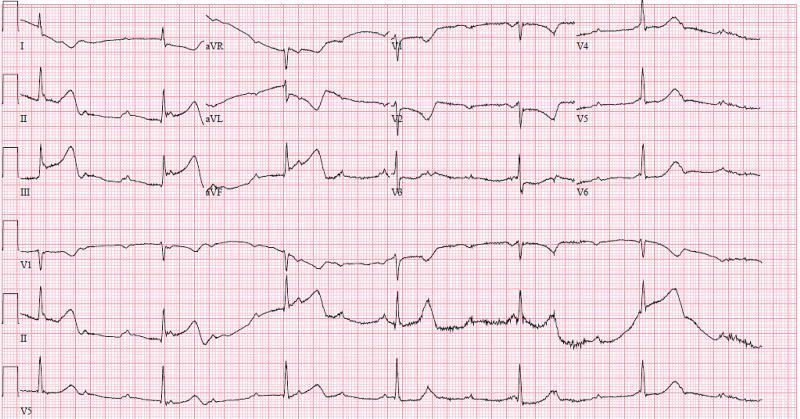
Inferior STEMI (RCA Occlusion)
ST elevation II, III, aVF (elevation greater in III than in II = 90% sensitive for RCA). Reciprocal depression in I and aVL.
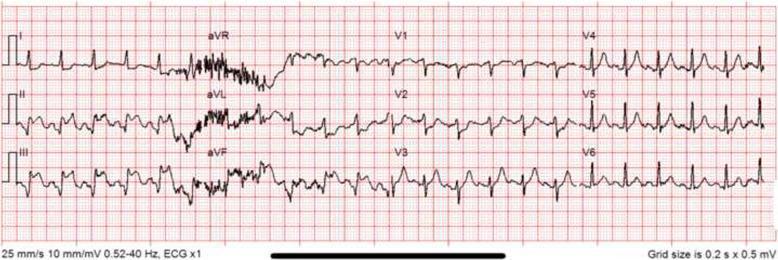
Inferior STEMI with Complete Heart Block (Proximal RCA)
When the proximal RCA is occluded, the AV node (supplied by RCA in 90%) is ischemic → complete AV block can complicate inferior STEMI.
Harrison's Anterior vs Inferior STEMI Sequence
8. Special ECG Patterns
Wellens Syndrome
- Deep symmetric T-wave inversions in V₁–V₄ (sometimes I and aVL)
- Indicates critical proximal LAD stenosis — often pain-free when ECG is taken
- High risk of imminent massive anterior MI
- Harrison's 22E
de Winter Pattern
- J-point depression + upsloping ST depression in precordial leads + prominent tall T waves
- ST elevation in aVR
- Represents proximal LAD occlusion — STEMI-equivalent that may not progress to classic ST elevation
- Rosen's Emergency Medicine
Posterior MI (Mirror Pattern)
- No direct leads overlie the posterior wall on standard 12-lead
- Reciprocal changes in V₁–V₃: tall broad R waves, ST depression, upright tall T waves
- Use posterior leads V₇–V₉ to confirm: ST elevation ≥0.5 mm = posterior STEMI
- Culprit: RCA posterior descending or LCx
- Rosen's Emergency Medicine, Tintinalli's Emergency Medicine
Right Ventricular MI
- Always obtain right-sided leads (V₃R, V₄R) in all inferior STEMIs
- ST elevation ≥1 mm in V₄R = RV MI (90% specificity)
- Critical because these patients are preload-dependent — nitroglycerin and diuretics are contraindicated (cause severe hypotension)
9. ECG vs Culprit Artery — Key Differentiators
(Tintinalli, Table 49-5)
| ECG Finding | Culprit |
|---|---|
| III elevation > II elevation + ST depression in I/aVL | RCA (Sens 90%, Spec 71%) |
| Above + ST elevation V₁/V₂R | Proximal RCA (Spec 100%) |
| Inferior ST elevation but III ≤ II; isoelectric/elevated aVL | LCx (the "silent" inferior STEMI) |
| V₁–V₃ elevation + RBBB + Q wave or ST > 2.5 mm V₂ | Proximal LAD |
| aVR elevation > 0.5 mm + diffuse ST depression | LMCA or severe multivessel |
| Wellens T-waves V₁–V₂ | LAD (proximal) |
10. Morphological Evolution (Pathology)
(Robbins & Kumar Basic Pathology, Table 9.2)
| Time Frame | Gross Appearance | Microscopy |
|---|---|---|
| 0–½ hr | None | None (reversible) |
| ½–4 hr | None | Sarcolemmal disruption; mitochondrial densities |
| 4–12 hr | Dark mottling | Coagulation necrosis onset, edema |
| 12–24 hr | Dark mottling | Pyknotic nuclei, hypereosinophilic myocytes, early neutrophils |
| 1–3 days | Yellow-tan center | Loss of nuclei + striations, peak neutrophils |
| 3–7 days | Soft center, hyperemic border | Neutrophil death; macrophage phagocytosis begins |
| 7–10 days | Maximally soft + yellow | Granulation tissue forming at margins |
| 2–8 weeks | Gray-white scar from border inward | Increased collagen, decreased cellularity |
| >2 months | Dense white scar | Complete fibrous scar |
11. Complications
(Robbins & Kumar, Rosen's Emergency Medicine)
| Complication | Timing | Notes |
|---|---|---|
| Arrhythmias | Immediate–days | VF is most common cause of death; VT, heart block (inferior MI), sinus bradycardia |
| Cardiogenic shock | Hours–days | >40% LV mass necrosed; mortality >50% |
| Free wall rupture | Day 3–7 (peak) | Softened necrotic tissue; causes acute hemopericardium + tamponade |
| Interventricular septal rupture | Day 3–7 | Sudden VSD with left-to-right shunt; new harsh systolic murmur |
| Papillary muscle rupture | Day 2–7 | Acute severe MR; pulmonary edema |
| RV infarction | Acute | Complicates inferior MI; hypotension + raised JVP + clear lungs |
| Pericarditis | Day 2–4 | Fibrinous; Dressler's syndrome (autoimmune) at 2–10 weeks |
| Mural thrombus | Days–weeks | Forms on dyskinetic LV wall; risk of systemic embolism |
| LV aneurysm | Weeks–months | Persistent ST elevation; risk of VT, thrombus, CHF |
| Heart failure / Cardiomyopathy | Late | Ventricular remodeling; progressive LV dilation |
12. Key Biomarkers
| Marker | Rises | Peaks | Returns to Normal | Notes |
|---|---|---|---|---|
| Troponin I/T (high-sensitivity) | 2–4 hr | 12–24 hr | 7–14 days | Gold standard; most sensitive & specific |
| CK-MB | 3–6 hr | 24 hr | 48–72 hr | Useful for re-infarction |
| Myoglobin | 1–2 hr | 6–10 hr | 24 hr | Very early but non-specific |
Summary: Quick Reference Table
| Territory | Blocked Artery | ST Elevation Leads | Reciprocal Depression | Special Features |
|---|---|---|---|---|
| Anterior/Anteroseptal | LAD | V₁–V₄ | II, III, aVF | Wellens, de Winter patterns |
| Anterolateral | Proximal LAD | V₁–V₆, I, aVL | II, III, aVF | Large territory = worst prognosis |
| High Lateral | LCx or D1 | I, aVL | III, aVF, V₁ | Can be subtle |
| Inferior | RCA (90%) or LCx (10%) | II, III, aVF | I, aVL | Check V₄R for RV; III > II = RCA |
| Posterior | RCA PDA or LCx | Tall R + ST depression V₁–V₃ | — | Use V₇–V₉ to confirm |
| Right Ventricular | Proximal RCA | II, III, aVF + V₃R–V₄R | Lateral | Preload-dependent; avoid nitrates |
| Left Main | LMCA | aVR > V₁; diffuse depression | — | Cardiogenic shock; emergency CABG |
Sources: Ganong's Review of Medical Physiology 26th Ed.; Robbins & Kumar Basic Pathology; Harrison's Principles of Internal Medicine 22E; Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.