Supra ventricular tachycardia short notes in paediatrics With reference nelson
Supraventricular Tachycardia (SVT) in Paediatrics
Short Notes - with reference to Nelson's Textbook of Paediatrics
Note on sources: Nelson's Textbook of Paediatrics is not directly available in this library. The notes below are compiled from equivalent authoritative paediatric references - Rosen's Emergency Medicine (Paediatric Cardiac chapter), The Harriet Lane Handbook (Johns Hopkins, 23rd ed.), and Tintinalli's Emergency Medicine - which align with Nelson's content on this topic.
Definition
Epidemiology
- No cardiac abnormalities are found in approximately 50% of cases
- Wolff-Parkinson-White (WPW) syndrome is found in only 10-20% of paediatric SVT
- Associated congenital heart disease includes Ebstein's anomaly and corrected transposition of the great arteries
- WPW prevalence: 0.1 to 3.1 per 1000; more common in boys
Mechanisms / Classification
1. Orthodromic AVRT (most common - narrow complex)
- Antegrade conduction: Atria → AV node → Ventricles (normal path)
- Retrograde conduction: Ventricles → Atria via accessory pathway
- Produces a narrow-QRS complex SVT
2. Antidromic AVRT (less common - wide complex)
- Antegrade conduction: Atria → Accessory pathway → Ventricles
- Retrograde: via AV node
- Produces a wide-QRS complex SVT
3. Other causes
- Atrioventricular nodal reentrant tachycardia (AVNRT)
- Atrial flutter / atrial fibrillation
- Automatic (ectopic) atrial tachycardia
- Junctional ectopic tachycardia (especially post-cardiac surgery)
Clinical Features
Infants
- Irritability, poor feeding, pallor
- Respiratory distress, tachypnea
- Signs of congestive heart failure (CHF) if prolonged: hepatomegaly, oedema
- Heart rate typically >220 beats/min
- Healthy infants can tolerate rates approaching 300 bpm for a time, but if untreated SVT produces signs of CHF and shock
Older Children
- Palpitations
- Difficulty breathing / chest discomfort
- Syncope (if rate high enough to impair cardiac filling)
- Heart rate typically >180 beats/min
ECG Features
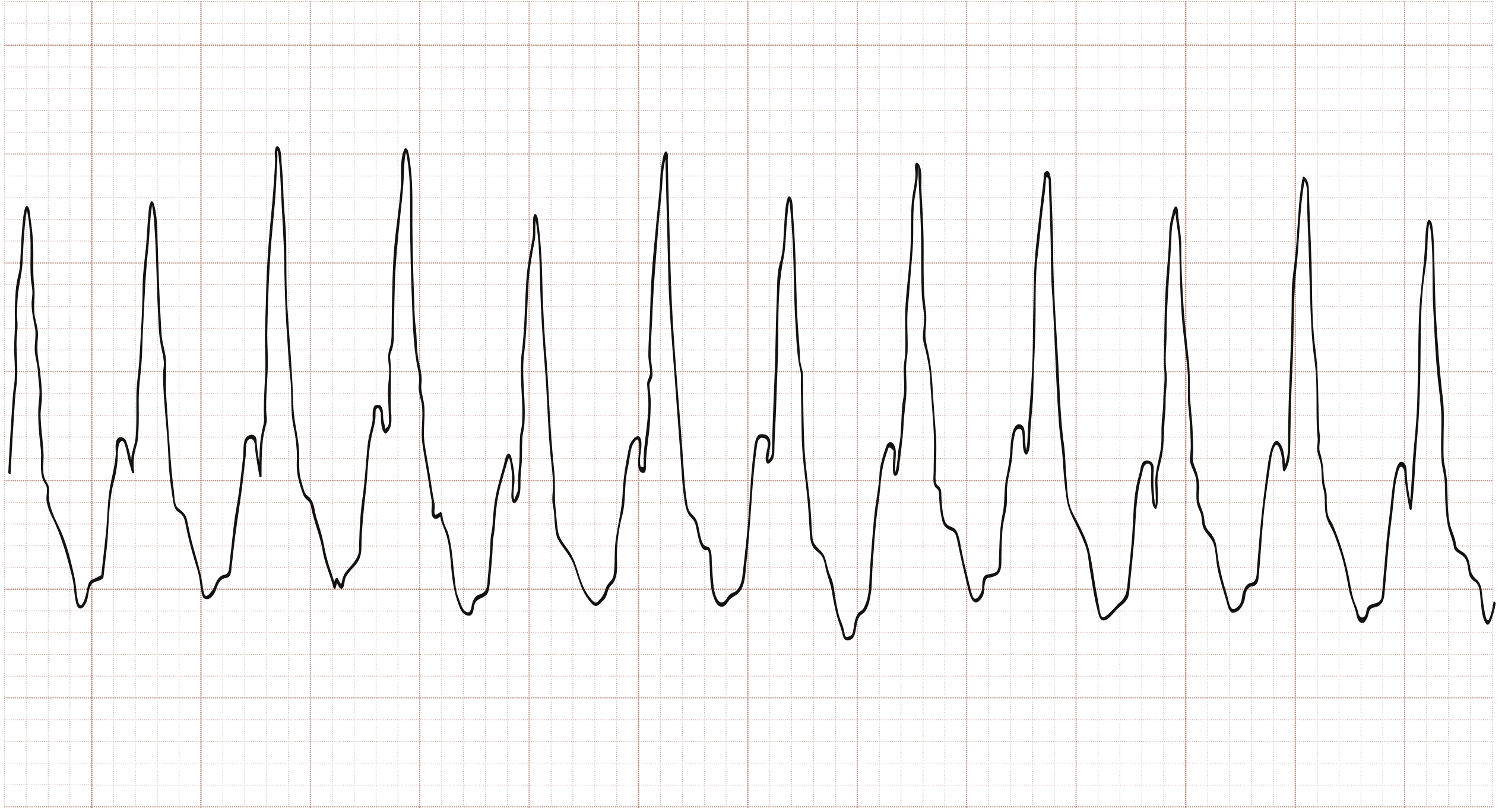
Key ECG findings in SVT:
- Rate: >220 bpm in infants; >180 bpm in children
- Rhythm: Regular, no beat-to-beat variability (constant R-R intervals)
- P waves: Absent or retrograde (buried in QRS or ST segment)
- Narrow QRS complex (orthodromic) or wide QRS complex (antidromic, WPW, or bundle branch block)
Differentiating SVT from Sinus Tachycardia
| Feature | Sinus Tachycardia | SVT |
|---|---|---|
| Precipitating events | Dehydration, fever, pain | No precipitating event |
| P waves on ECG | Present | Absent |
| Heart rate varies with activity | Yes | No |
| Beat-to-beat variability | Yes | Constant R-R intervals |
| Rate in infants | Usually <220 bpm | Usually >220 bpm |
| Rate in children | Usually <180 bpm | Usually >180 bpm |
WPW Syndrome - Key Points (Nelson's)
- Most common form of ventricular preexcitation in children
- Accessory pathway = thin strands of subendocardial tissue that "bypass" the AV node
- Some pathways are bidirectional; others are unidirectional
- "Concealed" pathways: conduct only retrograde - not visible on resting ECG but can trigger SVT
- ECG features during sinus rhythm: short PR interval + delta wave
- Familial autosomal dominant inheritance described; most cases sporadic
Management
Step 1 - Haemodynamically UNSTABLE (altered consciousness, hypotension, pallor, cyanosis, delayed cap refill)
- Immediate synchronized cardioversion
- Initial dose: 0.5-1 J/kg
- If no conversion: double to 2 J/kg
- No time for vagal maneuvers or adenosine in an unstable child
Step 2 - Haemodynamically STABLE
A. Vagal Maneuvers (first line)
- Ice to face (diving reflex) - most useful in infants; apply ice bag/cold water-soaked cloth to forehead, eyes, bridge of nose for 10-15 seconds (do NOT occlude airway; do NOT apply ocular pressure)
- Valsalva maneuver - exhale forcefully against closed glottis for 10-15 sec (suitable for older children)
- Modified Valsalva - semi-recumbent at 45°, perform Valsalva, then immediately supine with 15-sec passive leg raise at 45° (higher success rate)
- Carotid sinus massage - less effective in children; not recommended in infants; avoid if prior stroke/carotid disease
B. Adenosine (drug of choice if vagal maneuvers fail)
| Age | Initial dose | Second dose | Max single dose |
|---|---|---|---|
| Neonate | 0.05-0.1 mg/kg | Increase by 0.05-0.1 mg/kg q2 min | 0.3 mg/kg |
| Child | 0.1 mg/kg (max 6 mg) | 0.2 mg/kg (max 12 mg) | 12 mg |
| Adolescent (≥50 kg) | 6 mg | 12 mg | 12 mg |
- Half-life: <10 seconds - must be pushed rapidly and flushed
- Side effects: transient asystole, facial flushing, dyspnea, chest pain, headache, bronchospasm (avoid/use caution in asthmatics)
- Contraindicated: 2nd/3rd degree AV block, sick sinus syndrome (unless pacemaker in place)
- Drug interactions: methylxanthines (caffeine, theophylline) decrease effect; carbamazepine/dipyridamole increase toxicity; use with caution with digoxin
C. If adenosine fails - Elective cardioversion with procedural sedation
D. Amiodarone
- Loading dose: 5 mg/kg IV over 20-60 minutes
- Used for adenosine-refractory SVT or WPW with pre-excitation
Step 3 - Long-term Suppression / Prophylaxis
- Beta-blockers (propranolol, atenolol) - first-line for recurrent SVT
- Flecainide or sotalol for refractory cases
- Radiofrequency catheter ablation - definitive cure; indicated for recurrent, refractory SVT or high-risk WPW
Complications (if untreated)
- Congestive heart failure
- Cardiogenic shock
- Sudden cardiac death (rare - mainly in WPW with antegrade pre-excitation and rapid conduction to ventricles)
Summary Mnemonics
- Fast (>220 infants, >180 children)
- Fixed rate (no variability)
- No visible P waves
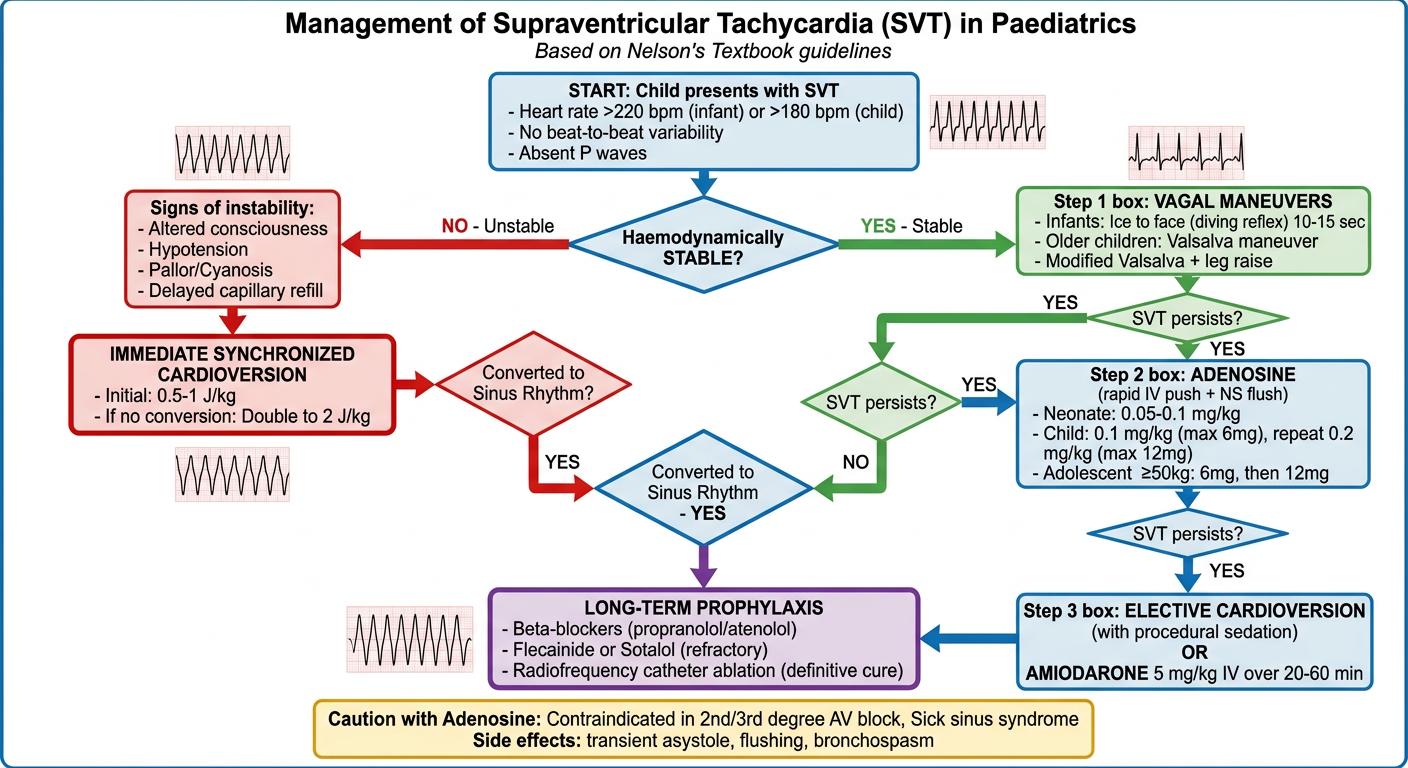
Management in flowchart diagram with image
A detailed medical flowchart diagram titled "Management of Supraventricular Tachycardia (SVT) in Paediatrics" based on Nelson's Textbook guidelines. The flowchart should be clean, professional, and easy to read with the following structure: START: "Child presents with SVT - Heart rate >220 bpm (infant) or >180 bpm (child), No beat-to-beat variability, Absent P waves" First decision diamond: "Haemodynamically STABLE?" LEFT branch (NO - Unstable): Red/orange color coding - "Signs of instability: Altered consciousness, Hypotension, Pallor/Cyanosis, Delayed capillary refill" - Action box: "IMMEDIATE SYNCHRONIZED CARDIOVERSION - Initial: 0.5-1 J/kg - If no conversion: Double to 2 J/kg" - Arrow to "Converted to Sinus Rhythm?" RIGHT branch (YES - Stable): Green color coding - Step 1 box: "VAGAL MANEUVERS - Infants: Ice to face (diving reflex) 10-15 sec - Older children: Valsalva maneuver - Modified Valsalva + leg raise" - Arrow: "SVT persists?" - Step 2 box: "ADENOSINE (rapid IV push + NS flush) - Neonate: 0.05-0.1 mg/kg - Child: 0.1 mg/kg (max 6mg), repeat 0.2 mg/kg (max 12mg) - Adolescent ≥50kg: 6mg, then 12mg" - Arrow: "SVT persists?" - Step 3 box: "ELECTIVE CARDIOVERSION (with procedural sedation) OR AMIODARONE 5 mg/kg IV over 20-60 min" Both paths converge at: "Converted to Sinus Rhythm - YES" - Final box: "LONG-TERM PROPHYLAXIS - Beta-blockers (propranolol/atenolol) - Flecainide or Sotalol (refractory) - Radiofrequency catheter ablation (definitive cure)" Bottom note box: "Caution with Adenosine: Contraindicated in 2nd/3rd degree AV block, Sick sinus syndrome. Side effects: transient asystole, flushing, bronchospasm" Use color coding: Red for unstable pathway, Green for stable pathway, Blue for drug boxes, Purple for long-term management. Include small ECG waveform icons to illustrate narrow vs wide complex SVT. Professional medical illustration style with clear arrows and decision points.
Haemodynamically UNSTABLE (Red pathway)
- Immediate synchronized cardioversion - 0.5-1 J/kg → if fails → 2 J/kg
- Do NOT waste time on vagal maneuvers or adenosine
Haemodynamically STABLE (Green pathway)
- Infants: Ice to face (diving reflex), 10-15 sec
- Older children: Valsalva / Modified Valsalva + leg raise
- Neonate: 0.05-0.1 mg/kg rapid IV push
- Child: 0.1 mg/kg (max 6 mg) → 0.2 mg/kg (max 12 mg)
- Adolescent ≥50 kg: 6 mg → 12 mg
- Elective cardioversion under procedural sedation, OR
- Amiodarone 5 mg/kg IV over 20-60 min
Long-term prophylaxis (Purple pathway)
- Beta-blockers (propranolol / atenolol) - first line
- Flecainide or sotalol for refractory cases
- Radiofrequency catheter ablation - definitive cure for recurrent/high-risk SVT