A 61-year-old patient came with high uric acid and 102 fever and BP 100/60. What should be the initial management?
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching PubMed
gout acute flare management guidelines 2024
I now have enough information to give a thorough, well-structured response. Let me synthesize everything.
Initial Management: 61-Year-Old with Hyperuricemia, Fever (102°F/38.9°C), and Hypotension (BP 100/60)
This clinical triad is a medical emergency that requires a systematic approach. The most critical issue is that fever + hypotension = presumptive sepsis/septic shock until proven otherwise, regardless of the uric acid level.
Step 1: Immediate Life-Threatening Assessment (First 10 Minutes)
The BP of 100/60 mmHg with fever meets criteria for sepsis with hemodynamic instability (possible septic shock). Do not anchor on gout alone.
Bedside priorities:
- IV access (2 large-bore peripheral lines)
- Cardiac monitor, pulse oximetry, 12-lead ECG
- Supplemental oxygen to maintain SpO2 >94%
- Rapid bedside assessment: mental status (confusion?), skin perfusion, urine output
Immediate investigations (draw BEFORE antibiotics):
- Blood cultures x2 (from 2 separate sites)
- CBC, CMP (renal function, electrolytes, LFT)
- Serum uric acid, serum lactate
- Urinalysis and urine culture
- Synovial fluid aspiration if a joint is swollen (to distinguish gout from septic arthritis - this is the single most important diagnostic test)
- Chest X-ray, joint X-ray if applicable
- CRP, ESR, procalcitonin
Step 2: Sepsis Resuscitation Bundle (Hours 1-3) - Surviving Sepsis Campaign
Since the patient is febrile + hypotensive, treat empirically for sepsis while the workup proceeds:
Fluids
- IV crystalloid (normal saline or Ringer's lactate) 30 mL/kg bolus for hypotension
- Reassess after each bolus for response vs. fluid overload
- If BP does not respond: start norepinephrine (vasopressor of choice in septic shock), targeting MAP ≥65 mmHg
Antibiotics
- Broad-spectrum IV antibiotics within 1 hour of diagnosis, before any imaging but after cultures
- Cover for the likely source: if joint-based, cover gram-positive organisms (especially S. aureus) with vancomycin + gram-negative coverage (e.g., piperacillin-tazobactam or cefepime)
- Choice should be guided by the presumed source (joint vs. urinary vs. pulmonary)
Step 3: Distinguish Gout Flare from Septic Arthritis (Critical Decision Point)
This is the key diagnostic challenge. Both can cause fever and an inflamed joint:
| Feature | Gout | Septic Arthritis |
|---|---|---|
| Fever | Mild-moderate | High, may be >38.9°C |
| Joint fluid WBC | 2,000-50,000/mm³ | Often >50,000/mm³ |
| Crystals on polarized microscopy | Needle-shaped, negatively birefringent | Absent |
| Gram stain/culture | Negative | Positive in ~60-80% |
| Serum uric acid | Elevated (but can be normal during attack) | May be normal or elevated |
Important: A raised uric acid alone does NOT confirm gout, and gout and septic arthritis can coexist. Joint aspiration with synovial fluid analysis (cell count, crystals, Gram stain, culture) is mandatory if a joint is involved.
Step 4: If Acute Gout Flare Is Confirmed
Once septic arthritis is excluded and hemodynamic stability is achieved, treat the gout flare. Given the clinical scenario (elderly, BP 100/60 suggesting possible renal hypoperfusion), drug selection is critical:
| Drug | Dose | Notes in This Patient |
|---|---|---|
| NSAIDs (indomethacin 50 mg TID, naproxen 500 mg BID) | First-line if no contraindications | Use with caution or AVOID given hypotension and possible renal compromise |
| Colchicine | 1.2 mg PO then 0.6 mg 1 hour later | AVOID if CrCl <30 or with renal insufficiency; also contraindicated with certain cardiac drugs |
| Oral corticosteroids | Prednisone 40-60 mg/day, taper over 7-10 days | Preferred in this patient - no renal dosing concern; can be used when NSAIDs and colchicine are contraindicated |
| Intra-articular steroids | Triamcinolone 40 mg (large joint) | Effective within 24 h in 90% of monoarticular attacks; septic arthritis must be ruled out first |
| IL-1 inhibitor (anakinra) | 100 mg SQ daily x3 days | Reserve for failure of above; contraindicated in active infection |
Do NOT start urate-lowering therapy (allopurinol/febuxostat) during an acute attack. Any acute change in uric acid level can worsen or prolong the flare. - Washington Manual of Medical Therapeutics
Step 5: Ongoing Monitoring
- Repeat BP and urine output every 30-60 minutes
- Serum lactate at 2 hours (target: clearance >10% or <2 mmol/L)
- Reassess antibiotic coverage at 48-72 hours when cultures return (de-escalate appropriately)
- If vasopressors required: ICU transfer
- Renal function monitoring if any nephrotoxic agents are used
Summary Algorithm for This Patient
Fever + Hypotension + High Uric Acid (61-year-old)
↓
Treat as SEPSIS FIRST (fluids + blood cultures + broad-spectrum IV antibiotics within 1 hour)
↓
Joint involvement? → Aspirate joint → Polarized microscopy + Culture
↓
Urate crystals + negative culture → Gout flare confirmed
↓
Hemodynamically unstable? → Prefer oral/IV corticosteroids (avoid NSAIDs, use colchicine only if renal function permits)
↓
Urate-lowering therapy (allopurinol) → Defer until 2+ weeks after attack resolves
Key clinical principle: Hypotension in a febrile, elderly patient is sepsis until proven otherwise. Anti-gout therapy is secondary to hemodynamic resuscitation and infection control. Oral corticosteroids are the safest anti-inflammatory option in this patient given the risk of NSAID-induced renal injury in the setting of hypotension.
- Rosen's Emergency Medicine, p. 2338
- Washington Manual of Medical Therapeutics, p. 948
- Creasy & Resnik's Maternal-Fetal Medicine (Sepsis Management Table)
This patient also showed TLC count 14,000 and potassium is 2.75. So what is the potassium correction I should give?
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Excellent - I have comprehensive information. Here is the detailed answer:
Potassium Correction for K+ = 2.75 mEq/L
Classification of This Patient's Hypokalemia
- K+ of 2.75 mEq/L = mild-to-moderate hypokalemia (normal: 3.5-5.0 mEq/L)
- The TLC of 14,000 + fever + hypotension in this patient points to sepsis as a likely driver (catecholamine surge from infection causes intracellular K+ shift, and fever/poor intake adds to losses)
- This is not immediately life-threatening at 2.75, but requires prompt correction given the cardiac risk in a febrile, potentially septic patient
Estimated Total Body Deficit at K+ = 2.75
As shown in the graph below, serum K+ grossly underestimates the true total body deficit because the body shifts K+ from intracellular stores to maintain serum levels:
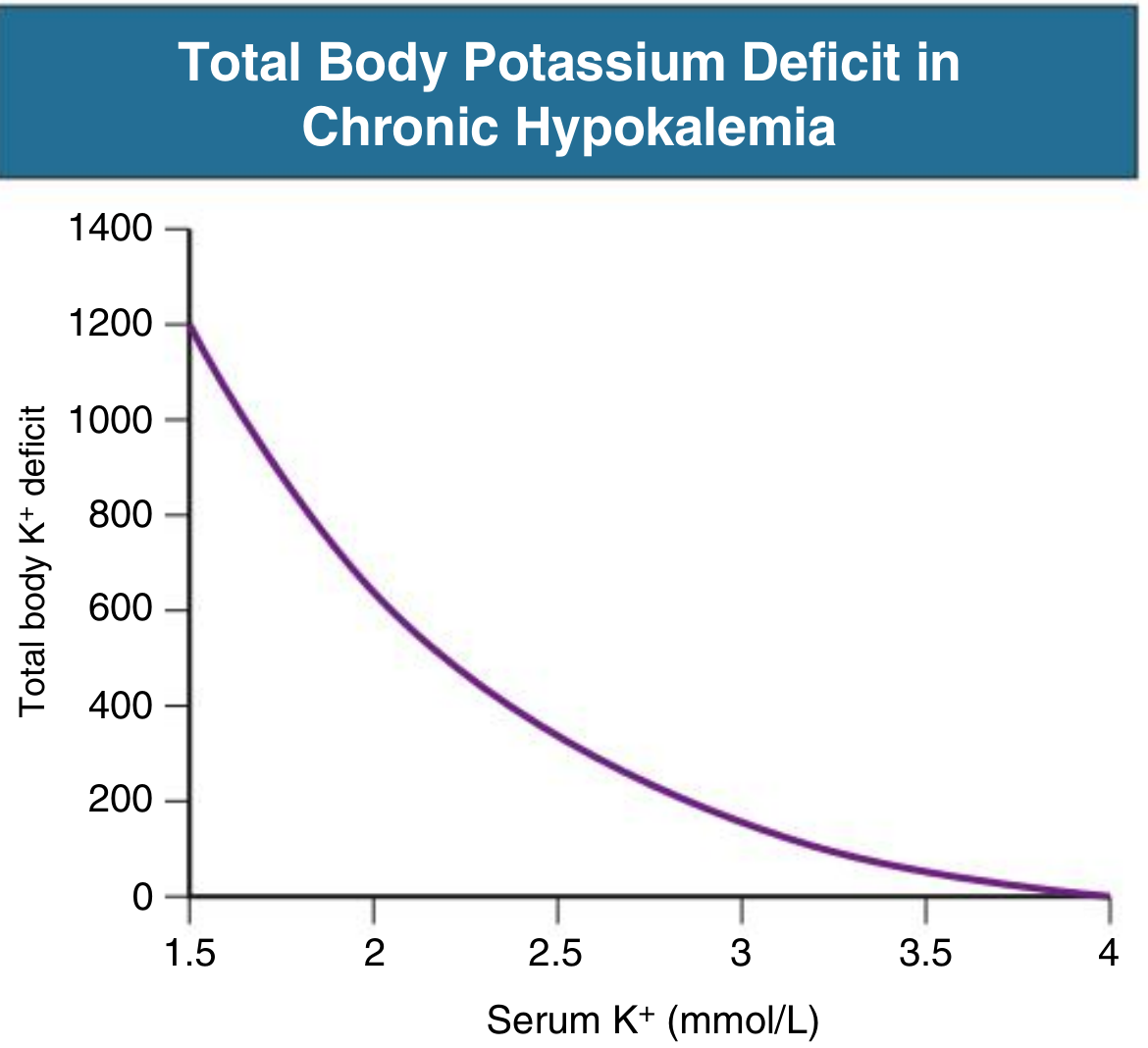
At a serum K+ of ~2.75 mEq/L, total body deficit is approximately 200-300 mEq - much more than you would calculate from extracellular fluid alone.
A useful rule of thumb: every 0.1 mEq/L fall in serum K+ below 3.5 represents approximately 10 mEq of total body deficit in mild-to-moderate hypokalemia.
- Patient's deficit: 3.5 - 2.75 = 0.75 mEq/L below normal
- Estimated deficit: ~100-150 mEq (mild-moderate range), but true total body deficit may be larger due to intracellular shift
Route of Administration
This patient is hemodynamically unstable (BP 100/60) and febrile - IV route is required.
- IV is preferred when oral intake is unreliable, patient is hypotensive, or when rapid correction is needed
- Do NOT use dextrose-containing fluids (D5W) as the diluent - it raises insulin, which drives K+ intracellularly and can paradoxically worsen hypokalemia
- Use normal saline (0.9% NaCl) as the carrier solution
IV Potassium Replacement Protocol
| Situation | Rate | Notes |
|---|---|---|
| Standard replacement | 10 mEq/hr | Safe via peripheral IV; cardiac monitoring advisable |
| Moderate hypokalemia (2.5-3.5) | 10-20 mEq/hr | Cardiac monitoring required if >10 mEq/hr |
| Emergency (arrhythmia, severe <2.5, respiratory compromise) | Up to 40 mEq/hr | Must use central vein; continuous ECG monitoring |
For this patient (K+ = 2.75, not in cardiac emergency):
- Give KCl 20 mEq in 100-200 mL NS over 1-2 hours
- Can repeat every 2-4 hours with K+ recheck
- Total correction over 24 hours: typically 40-100 mEq IV in divided doses, then reassess
- Recheck serum K+ after every 40-60 mEq given
Peripheral vs. Central Vein
- Peripheral vein: Max concentration 40 mEq/L (10 mEq/100 mL), max rate 10 mEq/hr - causes burning/phlebitis at higher concentrations
- Central vein: Can give higher concentrations and faster rates when urgently needed
- Given this patient's BP 100/60 and likely need for IV fluids/vasopressors, a central line is appropriate and should be used for K+ infusion
Critical Concurrent Checks
-
Check serum magnesium - Hypomagnesemia causes refractory hypokalemia (Mg2+ is a cofactor for K+ uptake into cells). If Mg2+ is low, correct it first or simultaneously, otherwise K+ correction will fail.
- Mg replacement: MgSO4 1-2 g IV over 15-30 minutes
-
ECG monitoring - Look for: flattened T waves, prominent U waves, prolonged QT, ventricular ectopy
-
Repeat K+ level after every 40-60 mEq replaced - never assume the deficit is corrected
-
Renal function - Given the hypotension in this patient, renal perfusion may be compromised. If oliguria/AKI develops, reduce replacement rate to avoid overshoot into hyperkalemia
-
Avoid NSAIDs (already relevant from gout management) - they impair renal K+ excretion regulation
Summary Order for This Patient
1. IV KCl 40 mEq in 500 mL NS over 4 hours (10 mEq/hr) via peripheral IV
OR KCl 20 mEq/hr via central line with continuous ECG monitoring
2. Check serum Mg2+ → if low, give MgSO4 1-2 g IV simultaneously
3. Recheck serum K+ in 4-6 hours
4. Repeat dosing until K+ >3.5 mEq/L (target >4.0 mEq/L in setting of cardiac risk/sepsis)
5. Once oral intake resumes, transition to oral KCl 40-100 mEq/day in 2-4 divided doses
6. Continue cardiac monitoring throughout
Replenishing total body K+ stores may take several days even after serum levels normalize, because intracellular refilling is slow.
- Sabiston Textbook of Surgery, p. 601
- Comprehensive Clinical Nephrology 7th Ed., p. 165
This is a shared conversation. Sign in to Orris to start your own chat.