Expalin superior vena cava
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compose a detailed, well-illustrated explanation.
Superior Vena Cava (SVC)
Overview
The superior vena cava (SVC) is the large, thin-walled, valveless venous trunk that returns deoxygenated blood from the head, neck, upper limbs, and thorax to the right atrium of the heart. It is one of the two great veins entering the heart (the other being the inferior vena cava).
Anatomy and Location
The SVC is a vertically oriented vessel located in the superior and middle mediastinum. Its key anatomical features, from Gray's Anatomy for Students:
- Origin: Formed posterior to the lower edge of the right first costal cartilage, where the right and left brachiocephalic veins unite
- Termination: Ends at the lower edge of the right third costal cartilage, draining into the superior right atrium
- Length: Approximately 6-8 cm
- The lower half is invested within the pericardial sac (middle mediastinum)
- Receives the azygos vein just before entering the pericardial sac (posteriorly)
- May also receive pericardial and mediastinal veins
Relations (from Braunwald's Heart Disease):
- Runs anterior to the right main stem bronchus
- Lies posterior to and to the right of the ascending aorta
- Adjacent to right paratracheal, azygos, right hilar, and subcarinal lymph node groups
The SVC is easily visible on a chest radiograph, forming part of the right superolateral border of the mediastinum.
Tributaries
| Tributary | Drainage Area |
|---|---|
| Right brachiocephalic vein | Right head, neck, upper limb |
| Left brachiocephalic vein | Left head, neck, upper limb |
| Azygos vein | Thoracic wall, posterior intercostal veins |
| Pericardial/mediastinal veins | Pericardium, mediastinum |
Embryological Development
From Langman's Medical Embryology and The Developing Human:
The SVC develops from the right anterior cardinal vein and the right common cardinal vein (duct of Cuvier). The venous return is initially bilateral but shifts to the right during development.
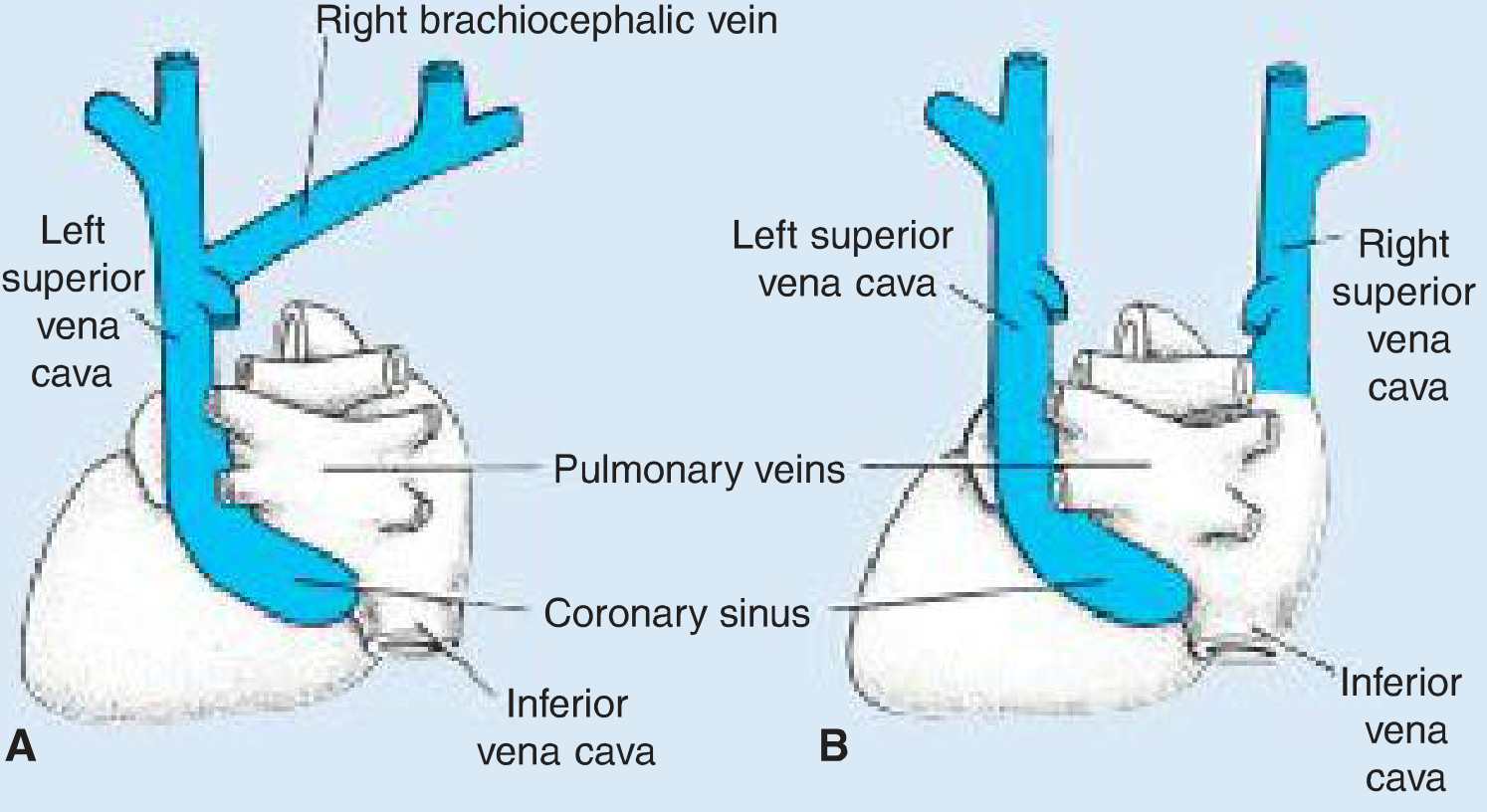
Congenital Anomalies:
- Left SVC - caused by persistence of the left anterior cardinal vein with obliteration of the right common cardinal/anterior cardinal veins. The left SVC drains into the right atrium via the coronary sinus.
- Double SVC - persistence of the left anterior cardinal vein along with failure of the left brachiocephalic vein to form. Both drain into the right atrium (left SVC through the coronary sinus).
Clinical Importance
1. Central Venous Access
The SVC is the standard landing zone for central venous catheters (CVCs), PICC lines, dialysis catheters, and pacemaker leads introduced via the subclavian, axillary, or internal jugular veins. The tips of these lines typically reside in the distal SVC or right atrium. The SVC's alignment with the inferior vena cava along the same vertical axis also allows guidewires to be advanced from SVC through the right atrium into the IVC for inferior vena cava filter placement and other procedures.
2. Superior Vena Cava Syndrome (SVCS)
SVCS results from obstruction of blood flow through the SVC, causing backup of venous pressure in the head, neck, and upper extremities.
History: First described by William Hunter in 1757 in a patient with a syphilitic aortic aneurysm.
Causes:
- Malignant (>85%): Lung carcinoma (most common), lymphoma, metastatic cancers
- Benign (3-15%): Thrombosis from intravascular devices (CVCs, pacemakers), fibrosing mediastinitis, thymoma, substernal goiter, aortic aneurysm, Behcet disease, radiation fibrosis
Why the SVC is vulnerable: It carries blood under low venous pressure, has a thin wall, and is surrounded by lymph nodes, the ascending aorta, and the trachea. Any mediastinal mass or lymphadenopathy can compress or invade it easily.
Clinical Features:
- Facial and neck edema (worse in the morning, improves with ambulation)
- Arm swelling
- Distended neck and chest veins
- Dyspnea, cough
- Facial plethora
- Less commonly: stridor, headache, syncope, hoarseness, confusion
The location of obstruction relative to the azygos vein matters clinically:
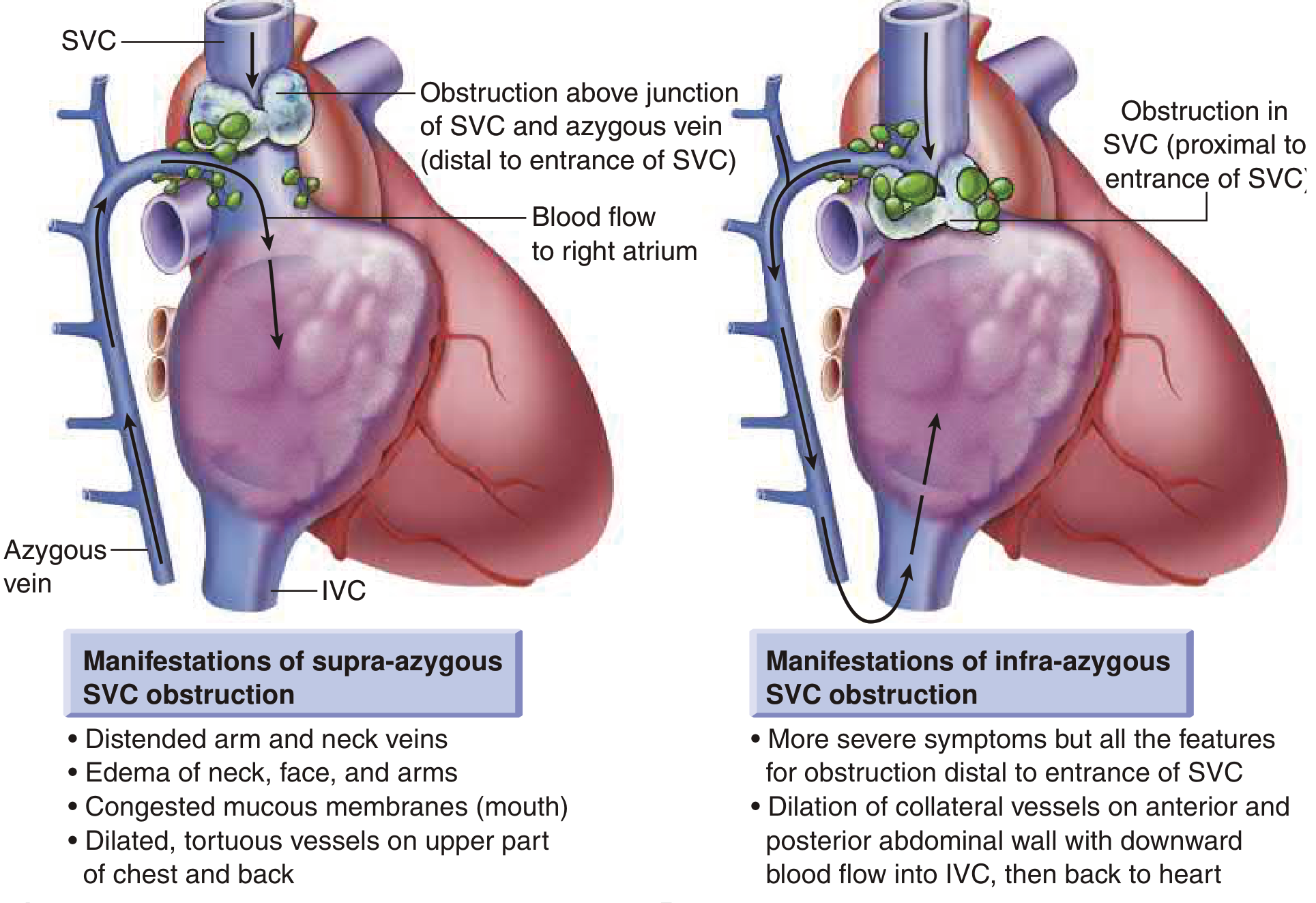
Investigations: Chest X-ray (widened mediastinum), CT chest (preferred - shows the level and cause of obstruction), MR venography (if contrast allergy), IV venography.
Treatment:
- Address the underlying cause (chemo/radiotherapy for malignancy)
- Endovascular stenting for thrombotic obstruction (palliative, rapid symptom relief)
- Surgical bypass in selected cases
- Median survival with malignant SVCS is approximately 6 months
Summary
| Feature | Detail |
|---|---|
| Formed by | Union of right and left brachiocephalic veins |
| Level of formation | Posterior to right 1st costal cartilage |
| Termination | Right atrium, at level of right 3rd costal cartilage |
| Length | ~6-8 cm |
| Pericardial portion | Lower half |
| Key tributary | Azygos vein (joins posteriorly just before pericardium) |
| Embryologic origin | Right anterior + common cardinal veins |
| Function | Drains head, neck, arms, thorax to right atrium |
Sources: Gray's Anatomy for Students, p. 256 | Braunwald's Heart Disease (p. 1196) | Langman's Medical Embryology | The Developing Human, 10th ed.
This is a shared conversation. Sign in to Orris to start your own chat.