chest pain (gastrointestinal, coronary artery diseases musculoskeletal, psychogenic)
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have rich textbook content and diagrams from multiple authoritative sources. Here is a comprehensive, well-organized response.
Chest Pain: Causes, Characteristics, and Clinical Approach
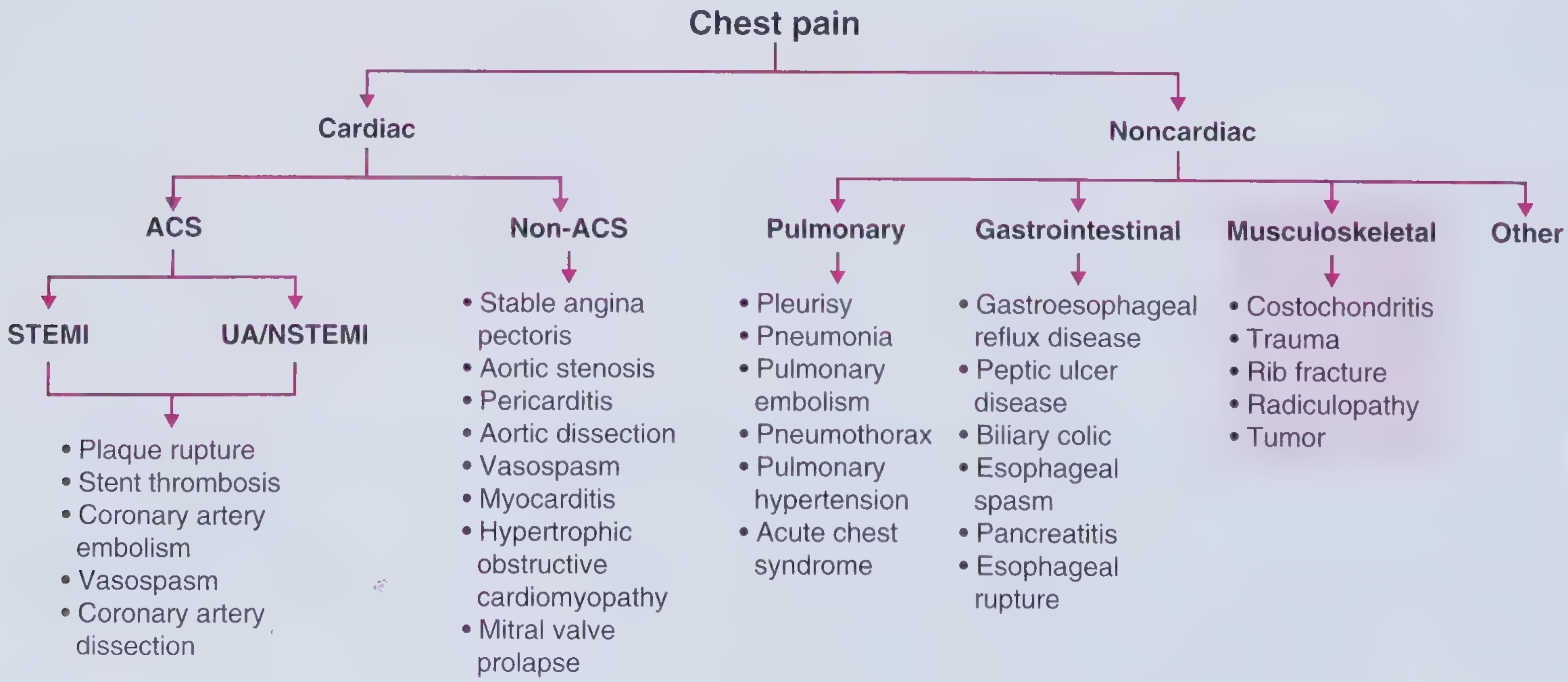
Chest pain differential - Frameworks for Internal Medicine
Chest pain is one of the most challenging symptoms in clinical medicine because its causes range from immediately life-threatening to entirely benign. The first task is always to rule out myocardial ischemia; only then should noncardiac causes be systematically evaluated.
1. Coronary Artery Disease (CAD)
Mechanism
Chest discomfort from CAD results from myocardial ischemia - an imbalance between myocardial oxygen supply and demand. This is the cardinal manifestation of CAD. - Goldman-Cecil Medicine
Classic Features (Diamond-Forrester Criteria)
For a pain to be classified as typical angina, it must meet all three criteria:
- Substernal, pressure-like quality
- Precipitated by exertion or emotional stress
- Relieved by rest or nitroglycerin within <30 minutes
- Atypical angina: meets 2 of 3 criteria
- Noncardiac chest pain: meets only 1 criterion
- Fuster and Hurst's The Heart, 15th Edition
Temporal Patterns
- Stable angina: triggered by exertion, lasts <5 minutes, resolves with rest or nitroglycerin
- Unstable angina/NSTEMI: pain at rest or with minimal exertion; clinically indistinguishable from MI except it may respond more rapidly to antianginal therapy
- STEMI: severe, ongoing pain building over several minutes; troponin elevation + ECG changes
- Chest pain lasting hours-to-days without troponin elevation or ECG changes strongly argues against angina
Important Nuances
- Women and older individuals may present with less classic ("atypical") symptoms despite equivalent or more advanced disease
- Patients often don't say "pain" - they may describe "pressure, ache, discomfort, uneasy feeling"
- Radiation to neck, jaw, shoulder, or arms must always raise suspicion
- Plaque rupture can cause sudden-onset rest pain even without prior anginal history
ACS Subtypes by Mechanism
| ACS Type | Mechanisms |
|---|---|
| STEMI / UA-NSTEMI | Plaque rupture, stent thrombosis, coronary artery embolism, vasospasm, coronary artery dissection |
| Non-ACS cardiac | Stable angina, aortic stenosis, pericarditis, aortic dissection, vasospasm, myocarditis, HOCM, MVP |
2. Gastrointestinal Causes
Epidemiology
Esophageal disorders - particularly GERD - account for 30-40% of noncardiac chest pain. Contrary to popular belief, GERD is far more common than esophageal spastic motor disorders as a cause. - Murray & Nadel's Respiratory Medicine; Yamada's Gastroenterology
Key Mechanism
Receptors in the esophageal wall respond to mechanical (spasm), chemical (acid), or thermal (hot liquids) stimuli. Afferent nerves travel through both vagal and spinal pathways (T3-T12). Pain from the distal esophagus can be referred directly over the heart and may radiate to neck and arms - mimicking angina almost perfectly. Esophageal pain can even be relieved by nitroglycerin. - Murray & Nadel's
GI Conditions Causing Chest Pain
| Condition | Key Features |
|---|---|
| GERD | Burning, postprandial, worse lying down; acidic taste; relieved by antacids |
| Esophageal spasm | Painful contractions; may mimic angina including radiation; can last >1 hour; residual dull ache |
| Nutcracker esophagus / Jackhammer esophagus | Dysmotility with high peristaltic pressures; episodic substernal pain |
| Peptic ulcer disease | Epigastric and retrosternal discomfort after meals; associated with NSAID use |
| Biliary colic | Right upper quadrant pain radiating to chest and right scapula |
| Acute pancreatitis | Epigastric and retrosternal pain radiating to the back; elevated lipase/amylase (≥3x ULN) |
| Boerhaave syndrome | Esophageal rupture after violent retching; subcutaneous emphysema + left pleural effusion - a surgical emergency |
| Functional chest pain | Rome IV criteria; increased visceral sensitivity; no identifiable organic cause |
Clinical Clues Favoring GI Origin
- Pain lasting >1 hour with residual dull ache
- Association with heartburn, odynophagia, or dysphagia
- Postprandial timing, positional changes
- Absence of ECG changes or troponin elevation
Management
Treatment strategies include proton pump inhibitors, calcium channel blockers, nitrates, and phosphodiesterase inhibitors. Workup includes upper endoscopy, barium swallow, and esophageal manometry. - Frameworks for Internal Medicine
3. Musculoskeletal Causes
Epidemiology
Musculoskeletal disorders of the chest wall account for 10-20% of noncardiac chest pain. - Murray & Nadel's
Conditions
| Condition | Characteristics |
|---|---|
| Costochondritis | Tenderness at costochondral junctions; responds to NSAIDs |
| Chest wall trauma / rib fracture | History of trauma; pain reproduced by palpation; responds to NSAIDs |
| Cervical radiculopathy ("cervical angina") | Compression of C4-C8 nerve roots (often from degenerative disc disease); associated neck pain |
| Subacromial bursitis | Shoulder-area pain |
| Herpes zoster | Unilateral dermatomal rash; burning pain along a dermatome |
| Intercostal muscle cramps | Often after vigorous activity or coughing |
| Chest wall tumor | Soft tissue sarcoma most common primary malignancy; may present in context of known malignancy |
| Pectus excavatum / carinatum | Congenital deformities occasionally causing pain |
The Key Diagnostic Clue
Pain reproducible on palpation of the chest wall is the single most useful feature distinguishing musculoskeletal pain from angina. A history of recent trauma, chest infection, or prolonged coughing also supports this diagnosis. - Murray & Nadel's; Frameworks for Internal Medicine
4. Psychogenic (Psychiatric) Causes
Epidemiology
Psychological factors may explain up to 50% of noncardiac chest pain - making it the single largest category of noncardiac chest pain. - Murray & Nadel's
Key Condition: Panic Disorder
- Panic attacks are the most common psychogenic cause
- Chest pain is one of the most frequently encountered somatic symptoms during a panic attack
- Patients may also have agoraphobia, major depression, and substance use
- A strong association exists between noncardiac chest pain and anxiety/panic disorder, particularly in patients with mitral valve prolapse
- Patients with documented heart disease may also have panic attacks - organic and psychiatric causes are not mutually exclusive
Pathophysiology
Psychological factors affect each person's interpretation of bodily sensations. Panic disorder produces real autonomic activation (tachycardia, diaphoresis, palpitations) that the patient experiences as life-threatening, reinforcing the cycle of anxiety. - Murray & Nadel's; Yamada's Gastroenterology
Distinguishing Features
- No exertional trigger (or anxiety itself is the "trigger")
- Associated features: palpitations, dyspnea, diaphoresis, tingling/paresthesias, fear of dying
- During episodes, eyes often closed (vs. true syncope/cardiac)
- Normal biomarkers, ECG, and stress testing
- Often young patients, or those with known anxiety/depression history
Treatment
Panic disorder responds well to:
- Nonpharmacologic: cognitive behavioral therapy (CBT)
- Pharmacologic: SSRIs are first-line
"Functional chest pain" (Rome IV) overlaps with both psychogenic and GI categories when no organic cause is identified and visceral hypersensitivity is present.
Comparative Summary Table
| Feature | CAD / Angina | GI | Musculoskeletal | Psychogenic |
|---|---|---|---|---|
| Quality | Pressure, squeezing, ache | Burning, crampy, spasm-like | Sharp, aching | Variable; "tightness" |
| Location | Substernal, radiates to arm/jaw | Substernal, epigastric | Localized chest wall | Substernal, diffuse |
| Trigger | Exertion, emotion, cold | Meals, lying down, alcohol | Palpation, movement, trauma | Anxiety, stress, spontaneous |
| Duration | <5 min (angina); >30 min (MI) | Minutes to hours | Variable | Minutes to hours |
| Relief | Rest, nitroglycerin | Antacids, PPIs, posture | NSAIDs, rest | Reassurance, anxiolytics |
| Palpation | Not reproducible | Not reproducible | Reproducible | Not reproducible |
| Associated Sx | Dyspnea, diaphoresis, nausea | Heartburn, regurgitation, dysphagia | Neck pain, skin changes (zoster) | Palpitations, tingling, fear of death |
| Biomarkers | Troponin elevated (MI) | Normal | Normal | Normal |
| ECG | Ischemic changes (ST, T wave) | Normal | Normal | Sinus tachycardia only |
Approach to the Patient
- First, rule out life-threatening causes: ACS, aortic dissection, pulmonary embolism, tension pneumothorax, Boerhaave syndrome
- Obtain 12-lead ECG and troponin in all cases of acute chest pain
- Use Diamond-Forrester criteria to estimate pretest probability of CAD
- If cardiac workup is negative, systematically evaluate GI, musculoskeletal, and psychogenic causes
- In most patients with noncardiac chest pain, no clear organic cause will be identified and symptoms are deemed functional - Yamada's Gastroenterology
Sources: Frameworks for Internal Medicine; Fuster and Hurst's The Heart, 15th Ed.; Goldman-Cecil Medicine; Murray & Nadel's Textbook of Respiratory Medicine; Yamada's Textbook of Gastroenterology, 7th Ed.; Cummings Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.