I am first yesr radiology PG resident I have a seminar topic on osteomyelitis Please give insights about the topic and detailed explanations for seminar and viva
Reading File
Finding Sources
Searching PubMed
"osteomyelitis"[MeSH Terms] AND "diagnostic imaging"[MeSH Terms]
Searching the Web
osteomyelitis radiology imaging MRI CT X-ray classification Cierny-Mader seminar 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Here is your comprehensive, exam-ready seminar on Osteomyelitis from a radiology PG perspective, sourced from Grainger & Allison's Diagnostic Radiology, Robbins & Kumar Pathologic Basis of Disease, Robbins Basic Pathology, and Bailey & Love's Surgery.
OSTEOMYELITIS - Radiology PG Seminar
1. DEFINITION & OVERVIEW
Osteomyelitis is inflammation of bone and bone marrow, virtually always secondary to infection. It may complicate any systemic infection but frequently manifests as a solitary primary focus. - Robbins & Kumar Pathologic Basis of Disease
2. CLASSIFICATION
By Duration
| Type | Duration | Key Features |
|---|---|---|
| Acute | <2 weeks | Neutrophilic reaction, bone edema, no sequestrum yet |
| Subacute | 2 weeks - 3 months | Brodie abscess, periosteal reaction |
| Chronic | >3 months | Sequestrum, involucrum, sinus tracts, sclerosis |
By Route of Infection
- Hematogenous - most common in children; metaphysis of long bones
- Contiguous spread - from adjacent soft tissue infection (diabetic foot, pressure sores)
- Direct inoculation - post-trauma, post-surgery, open fractures
Cierny-Mader Classification (Chronic Osteomyelitis - Surgical Staging)
Anatomic Type:
- Type I: Medullary (endosteal)
- Type II: Superficial (cortical surface only)
- Type III: Localized (cortical + medullary, stable bone)
- Type IV: Diffuse (entire bone circumference, unstable)
Physiologic Class:
- Class A: Normal host (good immune response)
- Class B: Compromised host (local or systemic)
- Class C: Treatment worse than disease
3. PATHOLOGY & PATHOPHYSIOLOGY
Acute Phase (within 48 hours)
- Bacteria proliferate → neutrophilic reaction
- Necrosis of bone cells and marrow within 48 hours
- Spread through Haversian canals → reaches periosteum
- Periosteum loosely attached in children → subperiosteal abscess forms
- Lifting of periosteum impairs blood supply → further necrosis
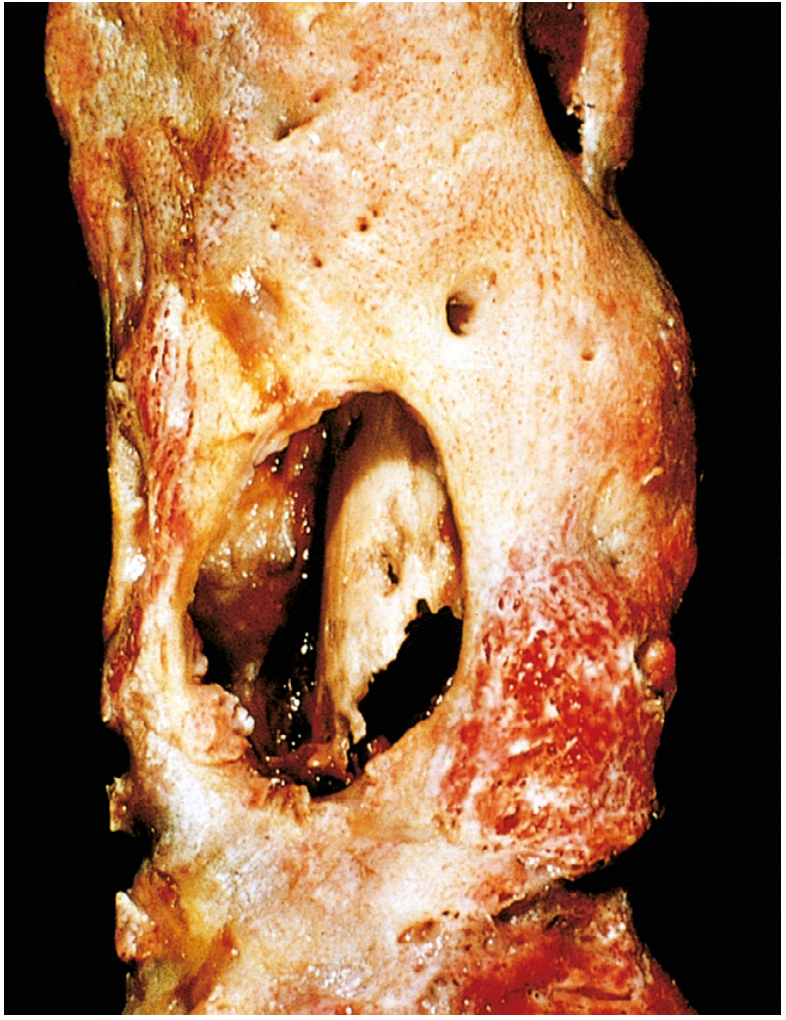
Chronic Phase (evolution)
- Devascularized dead bone = Sequestrum (the hallmark of chronic infection)
- New reactive bone shell around it = Involucrum
- Gaps in involucrum = Cloaca (through which pus discharges)
- Pus tracking to skin = Sinus tracts
- In chronic infection, walled-off abscess with sclerotic rim = Brodie Abscess
Key definitions for viva:
- Sequestrum: Dead devascularized bone surrounded by pus/granulation tissue. Dense, sclerotic on imaging.
- Involucrum: Shell of periosteal new bone formed around sequestrum.
- Cloaca: Opening in involucrum through which pus discharges into soft tissue.
- Sinus tract: Channel connecting the infected bone to the skin surface.
- Brodie Abscess: Subacute/chronic intraosseous abscess with sclerotic rim; typically in metaphysis of long bones.
4. MICROBIOLOGY
| Setting | Organism |
|---|---|
| Children (most common) | Staphylococcus aureus (80-90% of culture-positive cases) |
| Neonates | Group B Streptococcus, E. coli |
| Sickle cell disease | Salmonella spp. (also S. aureus) |
| Post-surgical / implants | Coagulase-negative staphylococci |
| Diabetic foot | Mixed gram-positive and gram-negative |
| IV drug users | Pseudomonas aeruginosa |
| Immunocompromised | Fungi (Candida, Aspergillus) |
| TB-endemic areas | Mycobacterium tuberculosis |
S. aureus staphylococcal cell wall proteins bind to bone matrix collagen, facilitating adherence - this is why it predominates. - Robbins & Kumar
5. LOCATION BY AGE (Critical for Viva)
Vascular anatomy of bone changes with age, which determines where infection localizes:
| Age Group | Location | Reason |
|---|---|---|
| Neonates (<1 yr) | Metaphysis + Epiphysis | Metaphyseal vessels penetrate growth plate |
| Children (1-16 yrs) | Metaphysis only | Growth plate is avascular barrier; rich metaphyseal sinusoids |
| Adults (>16 yrs) | Epiphysis + Subchondral | Growth plate closure creates anastomoses |
| Adults (spine) | Vertebral endplates | Dense end-arterial network at endplates |
Consequence in neonates: Epiphyseal involvement → spread to joint → septic arthritis with articular cartilage destruction and permanent disability.
6. IMAGING MODALITIES - SEQUENTIAL APPROACH
6A. Plain Radiograph (X-Ray)
- First-line investigation, but has significant limitations
- Lag period: Radiographic changes lag behind disease by 10-21 days (up to 2 weeks)
- At least 30-50% bone mineral must be destroyed before lytic change is visible on X-ray
Acute findings:
- Soft tissue swelling (earliest sign, within days)
- Periosteal reaction (linear/laminated)
- Focal cortical irregularity / destruction
- Ill-defined lucency in metaphysis
Chronic findings:
- Sequestrum: Dense opaque fragment within area of destruction ("dead bone in a sea of pus")
- Involucrum: Periosteal new bone shell (bone-within-a-bone appearance)
- Mixed lytic and sclerotic pattern
- Sclerosis and cortical thickening
Brodie Abscess on X-ray:
- Well-defined oval lytic lesion with sclerotic rim
- Classically in distal tibia metaphysis in children
- May show a "channel sign" - track extending to growth plate
Tuberculous Dactylitis (Spina Ventosa):
- Rare; cyst-like cavities with diaphyseal expansion
- More commonly in hand bones than feet
- Predominantly in children
6B. Ultrasound (USG)
- Particularly useful in infants and children
- Detects subperiosteal collections (fluid between periosteum and cortex) very early
- Can detect periosteal elevation and soft tissue edema before X-ray changes
- Guides aspiration and drainage procedures
- A difference of 1-2 mm in capsular distance between sides is suggestive of hip effusion
- Cannot evaluate intramedullary involvement
6C. CT Scan
Role:
- Best for defining cortical destruction
- Detects sequestrum clearly (dense fragment within lytic cavity)
- Identifies intraosseous gas (pathognomonic of infection)
- Demonstrates cloacae (channels/gaps in involucrum)
- Guides CT-directed biopsy/aspiration
- Evaluates sinus tracts (CT sinogram/fistulogram)
- Demonstrates vacuum phenomenon in disc (favors degeneration over infection in spine)
- Limitation: Radiation, poor soft tissue contrast, metal artefact
6D. MRI - The Gold Standard
MRI has the highest sensitivity and specificity for detecting osteomyelitis. Bone marrow edema is the earliest feature and can be detected as early as 1-2 days after onset. - Radiopaedia / Grainger & Allison
MRI Protocol:
- T1 coronal + axial
- T2/STIR (fat-suppressed)
- Post-gadolinium T1 fat-suppressed
- DWI (increasingly used)
Signal Characteristics:
| Sequence | Normal Marrow | Acute OM | Sequestrum | Abscess |
|---|---|---|---|---|
| T1 | High (fat) | Low | Very low | Low rim |
| T2/STIR | Low | High | Low | High center |
| Post-Gad | None | Enhancement | No enhancement | Rim enhancement |
Key MRI Signs:
- Bone marrow edema (T1 low, STIR high): Earliest finding - present within 1-2 days
- Subperiosteal abscess: T2 high signal collection lifting periosteum with rim enhancement
- Sequestrum: T1 and T2 low signal fragment with no enhancement (dead, avascular)
- Involucrum: T1 low, T2 low (cortical bone)
- Sinus tracts: Linear T2 high signal tracts extending from bone to skin
- Soft tissue edema/abscess: STIR high signal in surrounding muscles
Penumbra Sign (Subacute/Brodie Abscess):
- Peripheral relatively high-signal ring on T1 (granulation tissue) surrounding a low-signal central zone (abscess)
- Granulation tissue shows avid gadolinium enhancement
- Helps differentiate Brodie abscess from aggressive tumors like Ewing's sarcoma
Caution: On T2 sequences, reactive edema may exaggerate the extent of infection.
For Diabetic Foot Osteomyelitis:
- "High likelihood of osteomyelitis" phrase is recommended where there is bone marrow high signal on fluid-weighted sequences adjacent to an ulcer, abscess, or sinus tract, regardless of T1 signal. (ACR Appropriateness Criteria 2025)
- DWI + dynamic contrast-enhanced MRI improves diagnostic accuracy (Wudhikulprapan et al., Clin Radiol 2024 - systematic review, PMID 39168784)
6E. Nuclear Medicine / Radionuclide Imaging
Bone Scan (Tc-99m MDP):
- 3-phase bone scan: Flow, blood pool, delayed
- Very sensitive (>90%) but low specificity
- Positive in 24-48 hours of infection
- Remains positive for weeks even after treatment
- Limitation: Cannot distinguish tumor, fracture, inflammation
Gallium-67 Scan:
- Accumulates in areas of inflammation/infection
- Combined with bone scan increases specificity
- If Ga scan shows increased uptake where bone scan is normal → active infection
Labeled White Cell Scan (In-111 or Tc-99m HMPAO WBC):
- Most specific nuclear medicine study for infection
- Requires blood withdrawal, labeling, and reinjection
- Best for peripheral osteomyelitis
- Less useful in spine (normally active red marrow mimics WBC uptake)
FDG-PET/CT:
- Increasingly used, especially for:
- Chronic osteomyelitis monitoring
- Diabetic foot osteomyelitis
- Skull base osteomyelitis (malignant external otitis)
- Vertebral osteomyelitis
- High sensitivity and specificity
- Can monitor treatment response using SUV values
- A 2024 meta-analysis (Jin et al., Clin Radiol 2024, PMID 38880677) and 2026 systematic review (Laidlaw et al., Tomography 2026, PMID 41893827) confirm FDG-PET accuracy for skull base OM treatment response
7. VERTEBRAL OSTEOMYELITIS (SPONDYLODISCITIS)
Epidemiology
- Incidence: 2.4/100,000/year, increasing with age
- Lumbar spine most common (58%), then thoracic (30%), cervical (11%)
- Primary sources: UTI, skin/soft tissue, IV access, endocarditis, dental
Pathogenesis
- Starts at vertebral endplates (dense end-arterial network)
- Spreads to adjacent disc space
- Through disc → contiguous vertebral endplate destruction
- Extension into paravertebral soft tissues and epidural space
Imaging in Vertebral Osteomyelitis
Plain X-ray:
- Earliest (but late) sign: loss of disc height and endplate irregularity
- Later: vertebral body destruction, loss of disc space
- Even later: kyphosis (Gibbus deformity in TB)
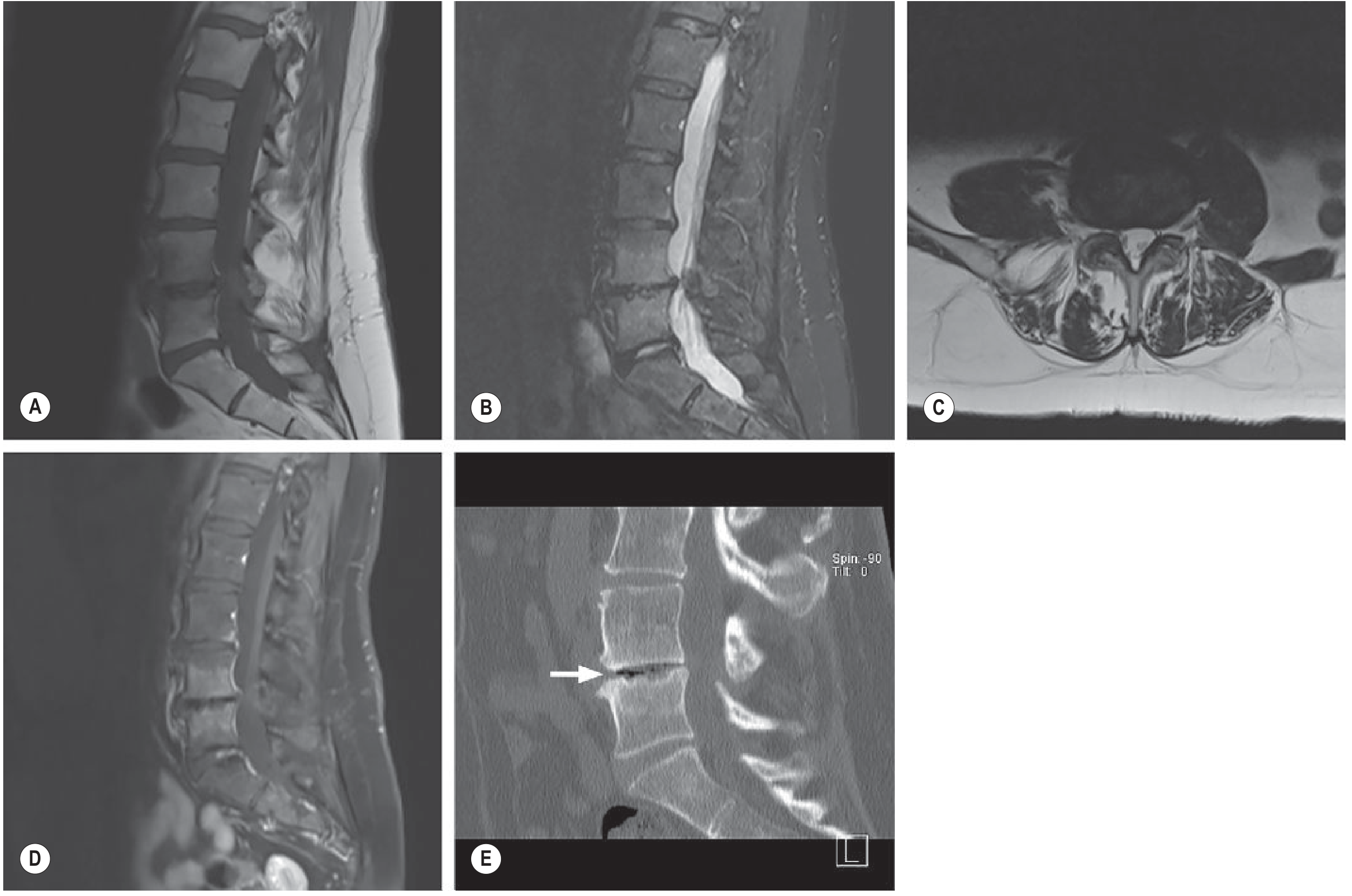
MRI - Investigation of Choice:
- T1: Low signal in vertebral bodies (loss of normal fat marrow signal)
- T2/STIR: High signal in vertebral bodies and disc
- Post-gadolinium: Enhancement of vertebral bodies and disc
- Key finding: Involvement of disc + BOTH adjacent vertebral bodies (disc "protected" in TB but destroyed in pyogenic)
Pyogenic vs TB Spondylodiscitis (High-Yield Comparison):
| Feature | Pyogenic | Tuberculous |
|---|---|---|
| Disc involvement | Early, prominent disc destruction | Relatively preserved disc (initially) |
| Vertebral bodies | 2 adjacent levels (skip rare) | Multiple levels, skip lesions possible |
| Paraspinal abscess | Smaller, phlegmon | Large cold abscess (psoas, paraspinal) |
| Endplate | Irregular, destroyed | Anterior wedging, gibbus deformity |
| Vacuum in disc | Favors degeneration | Against infection |
| Enhancement | Homogeneous | Peripheral rim-enhancing abscess |
| Calcification | Absent | May be present (chronically) |
| Cord compression | Less common | More common (Pott's paraplegia) |
Complications to identify on imaging:
- Epidural abscess (MRI - T2 high, rim enhancing collection posterior/anterior to cord)
- Paravertebral abscess
- Psoas abscess (CT/MRI)
- Cord compression / myelopathy
Modic Type I changes vs Infection - Key Differentiator:
- Modic I: T1 low, T2 high endplate changes without disc enhancement, normal disc height OR osteophytes
- Vacuum phenomenon on CT = Degeneration (infection virtually excluded)
8. PEDIATRIC OSTEOMYELITIS - SPECIAL POINTS
- Commonest organisms: S. aureus (older children), Group B Strep + E. coli (neonates), Kingella kingae (infants < 4 yrs - increasingly recognized)
- Kingella kingae: K. kingae is difficult to culture, often requiring PCR for identification, and has probably been historically underdiagnosed. Presents with mild musculoskeletal symptoms and only mild elevation of inflammatory markers. - Grainger & Allison
- Metaphyseal infections in neonates can cross the growth plate → epiphyseal involvement → septic arthritis
- Whole-body MRI or skeletal scintigraphy should be considered in neonates/infants to exclude multifocal infection
- Complications: Premature growth plate fusion ("chevron" epiphysis in meningococcal), limb length discrepancy, angular deformity
9. DIABETIC FOOT OSTEOMYELITIS
- Most common cause: Contiguous spread from overlying ulcer/cellulitis
- Predominantly involves forefoot (metatarsal heads, phalanges)
- Probe-to-bone test: Positive if a blunt probe through ulcer reaches bone (high specificity for OM ~90%)
- MRI is the recommended investigation
- Challenge: Differentiating OM from Charcot neuroarthropathy (both show marrow edema)
- ACR Appropriateness Criteria 2025 (PMID 41193054): MRI with and without contrast is the most appropriate initial advanced imaging; FDG-PET is appropriate when MRI is non-diagnostic or contraindicated
| Feature | Osteomyelitis | Charcot Neuroarthropathy |
|---|---|---|
| Location | Beneath ulcer/pressure point | Midfoot (Lisfranc, Chopart) |
| Skin | Ulcer present | No ulcer |
| Bone edema | Focal | Diffuse, multiple bones |
| Joint | May be involved | Fragmentation, dislocation |
| Enhancement | Present | Present |
| Sinus tract | Often present | Absent |
10. CHRONIC OSTEOMYELITIS - IMAGING OVERVIEW
- Hallmarks: Sequestrum + Involucrum + Sinus tracts + Sclerosis
- Plain X-ray usually sufficient to establish diagnosis; MRI for activity assessment
- CT: Best for surgical planning (extent of sequestrum, cloacae)
- MRI: Active infection shows enhancing marrow; healed/quiescent infection shows fatty conversion of marrow (T1 high)
- Squamous cell carcinoma can develop in chronic draining sinus tracts (Marjolin's ulcer) - complication of longstanding chronic OM
11. DIFFERENTIAL DIAGNOSES
For Periosteal Reaction + Bone Destruction
- Ewing's Sarcoma - can look identical on plain film; onion-skin periosteal reaction; usually diaphysis; aggressive; MRI shows large soft tissue mass; biopsy required
- Osteosarcoma - aggressive periosteal reaction (Codman triangle, sunburst), metaphyseal
- Langerhans Cell Histiocytosis - lytic lesion, periosteal reaction, younger patients
- Stress fracture - history, location, linear lucency
For Brodie Abscess
- Osteoid Osteoma - nidus < 2 cm, nocturnal pain relieved by aspirin
- Giant Cell Tumor - epiphyseal, adults, no sclerotic rim
- Chondroblastoma - epiphyseal in children
- Bone cyst - no sclerotic rim, no clinical infection
For Vertebral Lesion
- Metastasis - disc usually preserved (unlike pyogenic infection), pedicle destruction (vertebra plana), no endplate irregularity
- Multiple Myeloma - diffuse or focal, no disc involvement
- Modic Changes - vacuum disc, no paraspinal soft tissue
12. INVESTIGATIONS SUMMARY
| Investigation | Sensitivity | Specificity | Key Role |
|---|---|---|---|
| Plain X-ray | Low (early) | Moderate | First line; sequestrum, involucrum |
| USG | Good (soft tissue) | Moderate | Subperiosteal abscess, guided aspiration |
| CT | Moderate | Good | Sequestrum, cortical destruction, biopsy guide |
| MRI | 90-100% | 80-90% | Gold standard; earliest detection |
| Tc-99m bone scan | High (>90%) | Low | Multifocal disease, early detection |
| Labeled WBC scan | High | High | Most specific nuclear medicine modality |
| FDG-PET/CT | High | High | Monitoring treatment, chronic OM, diabetic foot |
13. VIVA QUESTIONS AND MODEL ANSWERS
Q1: What is the earliest radiological sign of acute osteomyelitis?
A: Soft tissue swelling is the earliest plain film sign. On MRI, bone marrow edema (T1 low, STIR high signal) is the earliest sign, detectable within 1-2 days of infection.
Q2: Why do plain X-rays have a lag in osteomyelitis?
A: Radiographic changes lag behind disease by 10-21 days because at least 30-50% of bone mineral must be lost before a lytic lesion becomes visible on plain films.
Q3: Define sequestrum, involucrum, and cloaca.
A: Sequestrum = devascularized dead bone fragment (dense, sclerotic on X-ray, very low signal on all MRI sequences, no enhancement). Involucrum = shell of periosteal new bone surrounding the sequestrum. Cloaca = gap/opening in the involucrum through which pus discharges.
Q4: What is the Penumbra sign on MRI?
A: Seen in Brodie abscess (subacute osteomyelitis). A peripheral T1 high-signal ring of granulation tissue surrounding the central T1-low abscess cavity. The granulation tissue shows avid gadolinium enhancement. Helps differentiate Brodie abscess from Ewing's sarcoma.
Q5: Why is the metaphysis affected in childhood osteomyelitis?
A: The metaphyseal sinusoidal vessels are sluggish, fenestrated, and lack phagocytic lining cells. This slowed flow, combined with microtrauma in the metaphysis, allows bacterial seeding during transient bacteremia.
Q6: Where does osteomyelitis localize in neonates vs. older children vs. adults?
A: Neonates: Metaphysis + epiphysis (metaphyseal vessels penetrate growth plate). Older children: Metaphysis only (growth plate is an avascular barrier). Adults: Epiphysis and subchondral region (growth plate closure creates anastomoses).
Q7: Which organism is most common in sickle cell osteomyelitis?
A: Salmonella species. Osteonecrosis in sickle cell disease creates nidus for bacterial seeding, and impaired splenic function reduces immune response to gram-negative organisms.
Q8: How do you differentiate pyogenic from tuberculous spondylodiscitis on MRI?
A: Pyogenic: Early disc destruction, adjacent two vertebral bodies, smaller paraspinal abscess, homogeneous enhancement. TB: Disc relatively preserved initially, large cold paraspinal/psoas abscess, anterior wedging, gibbus deformity, rim-enhancing abscess, may have skip lesions.
Q9: What is the role of vacuum phenomenon on CT in vertebral lesions?
A: Vacuum phenomenon (gas within disc) strongly favors degeneration over infection. It virtually excludes infective discitis because bacterial metabolism in the disc does not produce nitrogen gas.
Q10: What complication can develop in a chronic draining sinus tract?
A: Squamous cell carcinoma (Marjolin's ulcer) can develop in chronic draining sinus tracts of osteomyelitis. This is a rare but well-recognized complication of longstanding infection.
Q11: What is the Cierny-Mader classification?
A: An anatomico-physiological staging system for chronic osteomyelitis. It classifies the infection anatomically (Type I-IV: medullary, superficial, localized, diffuse) and the host physiologically (Class A: normal; Class B: locally or systemically compromised; Class C: treatment worse than disease).
Q12: Which is the best imaging modality for osteomyelitis in the diabetic foot?
A: MRI with and without contrast is recommended as first-line by ACR Appropriateness Criteria 2025. FDG-PET/CT is appropriate when MRI is non-diagnostic or contraindicated. A 2024 meta-analysis confirmed DWI + DCE-MRI improves accuracy.
Q13: What is Kingella kingae and why is it important?
A: It is a gram-negative β-hemolytic bacillus increasingly recognized as a cause of osteomyelitis and septic arthritis in infants and children under 4 years. It causes infection with almost normal blood markers and only mild fever, making diagnosis difficult. It requires PCR for identification as it is difficult to culture, and has been historically underdiagnosed.
Q14: What is the role of labeled WBC scan in osteomyelitis?
A: Labeled white cell scan (In-111 or Tc-99m HMPAO) is the most specific nuclear medicine study for bone infection. It is best for peripheral osteomyelitis. It is less useful in spinal osteomyelitis because normal active red marrow mimics WBC uptake.
Q15: What is spina ventosa?
A: Tuberculous dactylitis. Cystic cavities associated with diaphyseal expansion of bones of the hand (more than feet). Seen in children. The name refers to the "windswept" appearance of the expanded, air-filled bony digit on X-ray.
14. KEY IMAGING FINDINGS - QUICK RECALL TABLE
| Finding | Modality | Significance |
|---|---|---|
| Soft tissue swelling | X-ray | Earliest plain film sign |
| Subperiosteal abscess | USG / MRI | Early sign, especially in children |
| Sequestrum | X-ray / CT / MRI | Hallmark of chronic OM |
| Involucrum | X-ray / CT | Shell of new bone around sequestrum |
| Sinus tract | MRI / CT sinogram | Chronic OM, communication to skin |
| Penumbra sign | MRI T1 | Brodie abscess |
| Endplate erosion + disc destruction | MRI | Pyogenic spondylodiscitis |
| Large cold abscess | MRI | Tuberculous spondylodiscitis |
| Vacuum phenomenon | CT | Degeneration (NOT infection) |
| FDG uptake | PET/CT | Active infection / treatment monitoring |
15. RECENT EVIDENCE (PubMed 2024-2026)
- DWI + DCE-MRI in Diabetic Foot OM - A 2024 systematic review and meta-analysis (Clin Radiol) confirms that diffusion-weighted imaging and dynamic contrast-enhanced MRI improve diagnostic accuracy for diabetic foot osteomyelitis.
- ACR Appropriateness Criteria 2025 for Diabetic Foot OM - The 2025 ACR update recommends MRI with/without contrast as first-line; FDG-PET/CT when MRI is non-diagnostic.
- FDG-PET in Skull Base OM - A 2026 meta-analysis (Tomography) demonstrates FDG-PET is accurate for treatment response assessment in skull base osteomyelitis (malignant external otitis).
Suggested Seminar Structure (30-45 minutes)
- Definition + Epidemiology (2 min)
- Classification - by duration, route, Cierny-Mader (5 min)
- Pathophysiology - acute to chronic, key terms (5 min)
- Microbiology by clinical setting (3 min)
- Imaging approach - modality by modality with images (15 min)
- X-ray findings (acute/chronic/Brodie/TB dactylitis)
- USG role
- CT role
- MRI (gold standard - protocol, sequences, key signs)
- Nuclear medicine
- Special scenarios: Vertebral OM, Diabetic foot, Pediatric OM (8 min)
- Differentials (5 min)
- Recent evidence / ACR guidelines (2 min)
- Summary table + Viva Q&A
Sources:
- Grainger & Allison's Diagnostic Radiology (Elsevier)
- Robbins & Kumar Pathologic Basis of Disease (2024)
- Bailey & Love's Short Practice of Surgery (28th ed.)
- Campbell's Operative Orthopaedics (15th ed., 2026)
- ACR Appropriateness Criteria - Diabetic Foot Osteomyelitis (2025, PMID 41193054)
- Wudhikulprapan et al., Clin Radiol 2024 (PMID 39168784)
- Laidlaw et al., Tomography 2026 (PMID 41893827)
Good luck with your seminar! Focus especially on the MRI sequences and signal characteristics, the pyogenic vs TB spine comparison, and the age-based localization - these are the most common viva topics for radiology PG residents.
This is a shared conversation. Sign in to Orris to start your own chat.