What is the cause and treatment of Vetriculomegaly due to cerebral atrophy with seizure
Reading File
Checking Date & Time
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
ventriculomegaly cerebral atrophy seizure
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive answer synthesized from authoritative neurology and pathology textbooks.
Ventriculomegaly Due to Cerebral Atrophy with Seizure
1. Definition & Mechanism
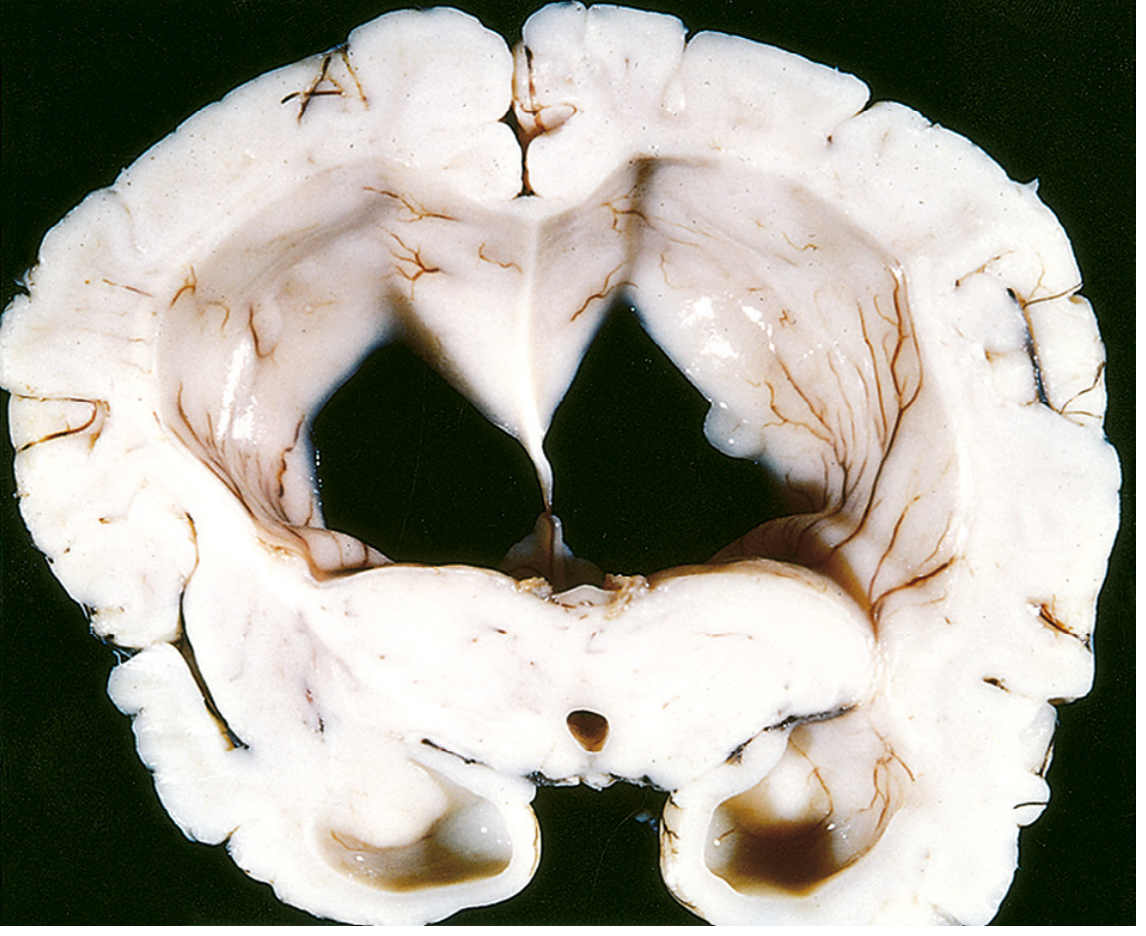
Ventriculomegaly secondary to cerebral atrophy is formally termed hydrocephalus ex vacuo. It is a compensatory, passive enlargement of the ventricular system (and subarachnoid spaces) that occurs when the brain loses parenchymal volume. As neurons and white matter are lost, CSF fills the resulting "empty" space — but this is NOT true hydrocephalus (intracranial pressure is normal or low, not elevated).
"Hydrocephalus ex vacuo is simply a descriptive term and is not itself responsible for any pathology. It refers to excess CSF in a region where brain tissue was lost as a result of stroke, surgery, atrophy, trauma, or other insult." — Neuroanatomy through Clinical Cases, 3rd Edition
2. Causes of Cerebral Atrophy Leading to Ventriculomegaly
Cerebral atrophy arises from many conditions. Major categories include:
Neurodegenerative Diseases
| Disease | Mechanism |
|---|---|
| Alzheimer's disease | Amyloid plaques + tau tangles → neuronal loss; widening sulci, ventricular enlargement (ex vacuo) |
| Frontotemporal lobar degeneration (FTLD) | Selective frontal/temporal neuronal loss |
| Huntington's disease | Striatal (caudate + putamen) atrophy → prominent hydrocephalus ex vacuo |
| Multiple system atrophy | Cerebellar + brainstem atrophy |
| Lewy body dementia | Widespread cortical neuronal loss |
Vascular Causes
- Multi-infarct (vascular) dementia — repeated ischemic strokes destroy parenchyma
- Binswanger's disease — subcortical white matter ischemia
- Cerebral amyloid angiopathy
Traumatic / Acquired
- Traumatic brain injury (TBI) — post-traumatic atrophy is common; most post-TBI patients with ventricular enlargement have hydrocephalus ex vacuo rather than true hydrocephalus
- Prolonged status epilepticus — repeated or sustained seizures themselves cause hippocampal and cortical neuronal death → atrophy
- Diffuse anoxic/hypoxic injury (cardiac arrest, near-drowning)
- Post-surgical resection
Infectious / Inflammatory
- HIV-associated neurocognitive disorder (HAND)
- Encephalitis (viral, autoimmune)
- Neurosyphilis, chronic meningitis
- Congenital Zika syndrome — cerebral calcifications, cortical malformations, ventriculomegaly due to brain atrophy are hallmarks
Toxic / Metabolic
- Chronic alcohol abuse — direct neurotoxicity + thiamine deficiency (Wernicke-Korsakoff)
- Heavy metal toxicity (lead, mercury, manganese)
- Chronic electrolyte abnormalities, hepatic/renal failure
- Vitamin B12 deficiency, hypothyroidism
Inherited / Developmental
- Hereditary spastic paraplegias (certain subtypes: e.g., SPG52 with ventriculomegaly + cerebellar atrophy + leukodystrophy)
- Inborn errors of metabolism (metachromatic leukodystrophy, etc.)
- Post-prematurity (intraventricular hemorrhage → periventricular white matter loss)
"With significant atrophy, there is compensatory ventricular enlargement (hydrocephalus ex vacuo) secondary to reduced brain volume." — Robbins, Cotran & Kumar: Pathologic Basis of Disease
3. Relationship Between Ventriculomegaly/Cerebral Atrophy and Seizures
This is bidirectional:
Atrophy → Seizures
- Loss of inhibitory interneurons, gliosis, and cortical reorganization after any of the above injuries creates epileptogenic foci
- Hippocampal atrophy (mesial temporal sclerosis) is one of the most common causes of temporal lobe epilepsy
- Cortical dysgenesis, post-stroke, and post-encephalitic scars all generate seizure foci
Seizures → Atrophy
- Prolonged status epilepticus causes glutamate-mediated excitotoxicity → neuronal death → hippocampal and cortical atrophy
- Repeated tonic-clonic seizures over years contribute to progressive hippocampal volume loss
4. Treatment
A. Treatment of the Underlying Cause of Cerebral Atrophy
This is the primary goal, as hydrocephalus ex vacuo itself does not require shunting or neurosurgical intervention (unlike true obstructive hydrocephalus or normal-pressure hydrocephalus).
| Cause | Targeted Treatment |
|---|---|
| Alzheimer's disease | Cholinesterase inhibitors (donepezil, rivastigmine), memantine; anti-amyloid therapies (lecanemab) |
| Vascular dementia | Antiplatelet therapy, BP/lipid control, stroke prevention |
| HIV encephalopathy | Antiretroviral therapy (ART) |
| Autoimmune encephalitis | Steroids, IVIG, plasmapheresis, rituximab |
| Thiamine deficiency | IV thiamine replacement |
| Metabolic causes | Correct underlying metabolic disorder |
| TBI | Supportive; neuroprotection; rehabilitation |
Note: Ventriculoperitoneal (VP) shunting is indicated for normal-pressure hydrocephalus (ventricles disproportionately enlarged relative to cortical atrophy with the triad of gait, incontinence, cognition) — NOT for hydrocephalus ex vacuo.
B. Treatment of Seizures (Antiepileptic Drug Therapy)
The goal of antiepileptic drug (AED) therapy is to maximize seizure control while minimizing drug toxicity.
Broad-Spectrum AEDs (Generalized Seizures)
| Drug | Mechanism |
|---|---|
| Valproate (valproic acid) | Enhances GABA; Na⁺ channel blockade |
| Lamotrigine | Na⁺ channel blockade |
| Levetiracetam | SV2A modulation |
| Topiramate | Na⁺ channels + GABA enhancement |
| Zonisamide | Na⁺ and Ca²⁺ channel blockade |
Narrow-Spectrum AEDs (Focal/Partial Seizures — common in atrophic brains)
| Drug | Mechanism |
|---|---|
| Carbamazepine | Na⁺ channel blockade — first-line for focal seizures |
| Oxcarbazepine | Na⁺ channel blockade |
| Phenytoin | Na⁺ channel blockade |
| Gabapentin / Pregabalin | Reduce excitatory neurotransmitter release (Ca²⁺ channel α2δ subunit) |
"Carbamazepine or lamotrigine is generally first-line treatment for children, young people and adults with focal seizures." — Swanson's Family Medicine Review
Drug-Resistant Epilepsy
- ~30% of patients with focal seizures are resistant to medical treatment
- Options include:
- Surgical resection of the epileptogenic zone (most effective for drug-resistant epilepsy)
- Vagal nerve stimulator (VNS) implantation
- Responsive neurostimulation (RNS)
- Ketogenic diet (especially in children)
Status Epilepticus (Emergency Management)
- Benzodiazepines first (lorazepam IV, diazepam, midazolam)
- Second-line: IV levetiracetam, valproate, or fosphenytoin
- Refractory: general anesthesia (propofol, midazolam, pentobarbital)
5. Imaging Approach
- MRI brain is the gold standard — high-resolution T1, FLAIR, coronal hippocampal views
- MRI has ~85% sensitivity for lesion detection in intractable epilepsy
- EEG / video-EEG for seizure classification and localization
- FDG-PET / amyloid PET for neurodegenerative work-up
- CT in acute/emergency settings
Summary
| Aspect | Key Points |
|---|---|
| Mechanism | Hydrocephalus ex vacuo — passive CSF fill of space vacated by lost brain tissue |
| Common causes | Neurodegeneration (AD, HD), vascular disease, TBI, encephalitis, alcohol, hypoxia, congenital infections |
| Seizures | Result from gliosis, cortical scarring, hippocampal atrophy; also worsen atrophy over time |
| Ventriculomegaly treatment | Treat underlying cause; shunting NOT indicated for ex vacuo |
| Seizure treatment | AEDs (carbamazepine/lamotrigine for focal; valproate/levetiracetam for generalized); surgery for drug-resistant cases |
Sources: Neuroanatomy through Clinical Cases 3rd Ed. · Robbins, Cotran & Kumar: Pathologic Basis of Disease · Adams and Victor's Principles of Neurology 12th Ed. · Barash et al. Clinical Anesthesia 9th Ed. · Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.