Empyhema
Reading File
Finding Sources
Searching PubMed
empyema thoracis management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it.
Empyema (Empyema Thoracis)
Definition
Empyema is a collection of frank pus (purulent fluid) within the pleural space, resulting from invasion by pyogenic bacteria, fungi, parasites, or mycobacteria. It represents the end of a spectrum that begins with a simple parapneumonic effusion and progresses through increasingly infected and loculated stages. - Sabiston Textbook of Surgery, p. 2471
Pathogenesis and Stages
The American Thoracic Society classifies empyema into three overlapping stages:
| Stage | Fluid Character | WBC (cells/mm³) | LDH (IU) | pH | Bacteria |
|---|---|---|---|---|---|
| Exudative | Thin, free-flowing, elastic | <1,000 | <500 | >7.3 | Absent |
| Fibrinopurulent | Purulent, inelastic, loculated | >5,000 | >1,000 | <7.1 | Present |
| Organizing | Thick, rigid fibrous peel | Varies | Varies | <7.1 | Varies |
- Mulholland and Greenfield's Surgery, p. 4359
Stage 1 - Exudative: Increased permeability of pleural membranes leads to influx of inflammatory cells and protein-rich exudate. Fluid is thin and sterile. Most patients respond to antibiotics without drainage.
Stage 2 - Fibrinopurulent: Increased procoagulant activity promotes fibrin deposition with early then extensive septations. Pleural fluid becomes viscous; LDH rises, glucose and pH fall. Macroscopically purulent fluid. Drainage is required; chest tube alone may be insufficient.
Stage 3 - Organizing: Fibroblast proliferation generates a fibrous pleural peel encasing the lung ("trapped lung"), preventing re-expansion. Decortication is required.
- Fishman's Pulmonary Diseases, Table 76-6
Causes
- Parapneumonic: Most common. Up to 50% of pneumonias have an associated effusion, but <5% progress to empyema.
- Trauma: Penetrating thoracic injury, hemothorax superinfection
- Post-surgical: Thoracotomy, pneumonectomy (bronchopleural fistula)
- Esophageal rupture/perforation
- Hematogenous spread from distant infection
- Tuberculosis: Especially in endemic areas or HIV-infected patients
Microbiology
Organisms have shifted significantly from the preantibiotic era:
- Pre-antibiotic era: Streptococcus pneumoniae predominated (64% of all empyemas)
- Current era: Anaerobic bacteria in up to 75% of cases; mixed aerobic-anaerobic flora very common
- Key anaerobes: Fusobacterium nucleatum, Prevotella spp., Peptostreptococcus spp., Bacteroides fragilis
- Key aerobes: Streptococcus pneumoniae, S. aureus, Klebsiella pneumoniae (especially hospital-acquired)
- Hospital-acquired empyemas: Higher prevalence of S. aureus and gram-negative rods
Pleural infections are associated with death or surgical intervention in >30% of patients. - Fishman's Pulmonary Diseases, p. 127
Clinical Features
- Systemic: Fever, malaise, weight loss, anorexia
- Respiratory: Dyspnea, pleuritic chest pain, reduced breath sounds, dullness to percussion
- In children: Worsening pneumonia with tachypnea, sometimes cyanosis; abdominal pain may be present
- Chronicity: Progressive debilitation if untreated; can form pleurocutaneous fistula, chest wall mass, or rib/vertebral destruction (especially TB empyema)
Diagnosis
Imaging
- Chest X-ray: First-line; shows pleural effusion, may reveal loculations
- Chest CT: Best modality for identifying loculations and distinguishing empyema from lung parenchymal pathology (e.g., lung abscess). Enhancing pleural rind ("split pleura sign") is characteristic.
- Ultrasound: Used to guide drainage and assess echogenicity/septations; helps identify optimal access site before thoracoscopy
Pleural Fluid Analysis (Thoracentesis)
| Parameter | Significance |
|---|---|
| pH <7.2 | Complicated effusion requiring drainage |
| Glucose <30 mg/dL | Strongly suggests empyema |
| LDH P:S ratio >0.6 | Exudate (Light's criteria) |
| Protein P:S ratio >0.5 | Exudate (Light's criteria) |
| Gross pus | Diagnostic of empyema regardless of other values |
| Positive Gram stain/culture | Confirms infection |
- Fischer's Mastery of Surgery, Table 91.2
Treatment
Treatment depends on the stage, severity, and patient comorbidities. The two cornerstones are drainage and antibiotics.
1. Antibiotics
- Directed by culture; empiric coverage must include anaerobes
- Used in all stages; alone sufficient only in early exudative stage with small effusion
2. Drainage
Stage 1 (Exudative): Antibiotics +/- simple thoracentesis or small pigtail catheter; chest tube if larger
Stage 2 (Fibrinopurulent):
- Chest tube (28-32 Fr) - may not be effective for loculated disease
- Intrapleural fibrinolytics: tPA + DNase (combination) - proven in RCTs to improve drainage and reduce surgical referral. A 2024 systematic review (PMID 39182102) found surgery vs. fibrinolysis outcomes comparable in many cases
- Saline irrigation via thoracostomy - useful in patients not candidates for surgery or tPA/DNase
Surgical Options:
- VATS (Video-Assisted Thoracoscopic Surgery): Definitive in 85-91% of patients; creates a single cavity, removes fibropurulent membranes, allows decortication. Early VATS reduces hospital length of stay. Preferred in complex/loculated disease.
- Open thoracotomy + decortication: For organized empyema with thick pleural peel; strips the fibrous rind off the lung to allow re-expansion. Remains standard for late-stage disease.
- Tube removal when drainage <100-200 mL/day with resolving clinical signs
3. Special Situations
Postpneumonectomy empyema: Very challenging; no lung tissue to fill the empty thorax. Options:
- Eloesser flap - creates an open chest window
- Clagett procedure - open drainage with antiseptic irrigation and later closure
TB empyema: Rare; occurs late in debilitated patients; cavity rupture into pleura causes bronchopleural fistula. Untreated: pleurocutaneous fistula, rib destruction.
Risk Stratification - RAPID Score
The RAPID score predicts 3-month mortality:
| Variable | Components |
|---|---|
| R - Renal function | BUN/urea |
| A - Age | |
| P - Purulence | |
| I - Infection source | Community vs. hospital |
| D - Dietary factors | Albumin |
| RAPID Category | 3-Month Mortality |
|---|---|
| Low risk | 3% |
| Medium risk | 9% |
| High risk | 31% |
High-risk patients may benefit from earlier surgical intervention. - Fishman's Pulmonary Diseases
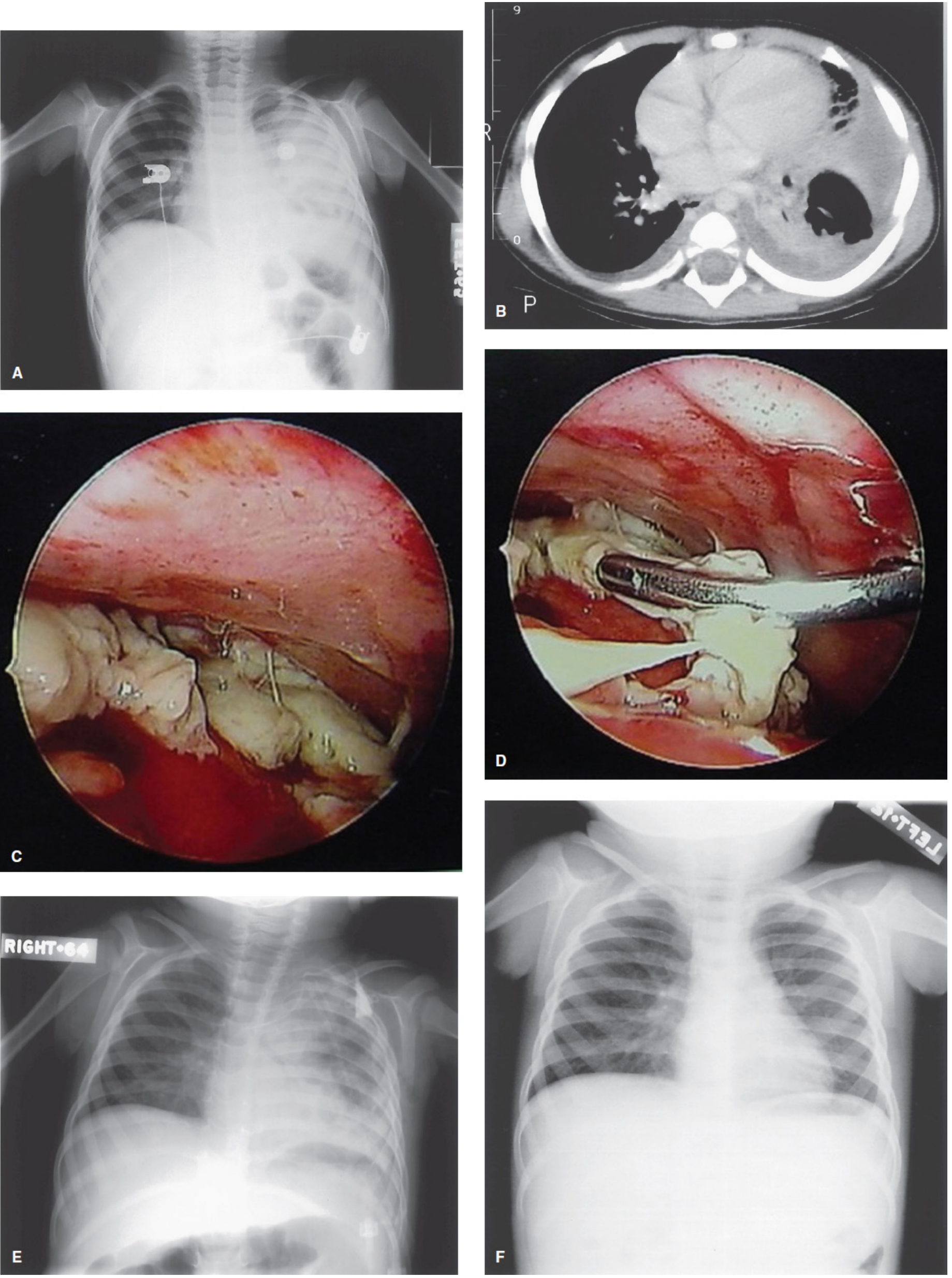
VATS in Empyema - Illustrated
Key Points Summary
- Empyema = pus in the pleural space; most often complicates pneumonia
- Three stages: exudative → fibrinopurulent → organizing; stage determines treatment
- Anaerobes now dominate (up to 75%); hospital-acquired cases have more S. aureus / gram-negatives
- Diagnose with CT + pleural fluid analysis (pH <7.2, glucose <30 mg/dL, gross pus)
- Treatment: antibiotics + drainage (escalate from thoracentesis → chest tube + tPA/DNase → VATS → open decortication based on stage)
- Organized empyema with trapped lung requires decortication; postpneumonectomy empyema may need Eloesser flap or Clagett procedure
- RAPID score identifies high-risk patients (3-month mortality up to 31%)
Recent evidence note: A 2024 systematic review (PMID 39182102) comparing surgery vs. intrapleural fibrinolysis for complicated pleural infections found no clear superiority of surgery; early VATS and combined tPA/DNase are both reasonable first-line interventions in fibrinopurulent empyema.
This is a shared conversation. Sign in to Orris to start your own chat.