Use of epidemiology
Reading File
Searching the Web
uses of epidemiology in public health
Finding Sources
Reading File
Reading File
Reading File
Reading File
Here is a detailed breakdown of the Uses of Epidemiology, drawn directly from Park's Textbook of Preventive and Social Medicine:
Uses of Epidemiology
Epidemiology was originally defined narrowly as the study of epidemic diseases. Over time its scope has expanded far beyond searching for disease causes. Morris identified seven distinct uses, five of which extend epidemiology to broader concerns of modern medicine:
"A means of learning, or asking questions... and getting answers that lead to further questions."
1. To Study the Historical Rise and Fall of Disease
Epidemiology allows us to examine how disease patterns change over time in human populations. Health and disease are never constant - they fluctuate over short and long periods.
- The first contribution to the study of coronary heart disease (CHD) was recognizing it as an "epidemic."
- Old diseases like smallpox are conquered, while new ones like Legionnaires' disease, Lassa fever, and AIDS emerge.
- By studying time trends, useful projections into the future can be made and emerging health problems identified.
As Churchill noted: "The farther back you look, the farther forward you can see."
2. Community Diagnosis
This refers to identifying and quantifying health problems in a community using mortality and morbidity rates and ratios. It helps identify individuals or groups at risk or in need of health care.
Community diagnosis serves three purposes:
- Priority setting - quantifying problems helps decide which diseases to tackle first.
- Benchmark creation - morbidity/mortality data serves as a baseline for evaluating health services later.
- New knowledge - reveals patterns of disease distribution, causation, and prevention.
Community diagnosis also covers the social, cultural, and environmental characteristics of the community. This is why epidemiology is described as the "diagnostic tool of community medicine."
3. Planning and Evaluation of Health Services
Epidemiologic data forms the fundamental basis for rational allocation of limited resources.
Planning examples:
- Determining the number of hospital beds required for specific diseases
- Health manpower planning
- Planning immunization campaigns and screening programs
- Provision of sanitary services
Evaluation: Any control measure must be followed by evaluation. For example, evaluating a hepatitis vaccine requires measuring not just effectiveness in reducing disease frequency, but also the cost of large-scale application - vaccine cost, trained personnel, storage, and transport. This application of epidemiology to health care problems is called the "new epidemiology."
4. Evaluation of Individual Risks and Chances
Epidemiologists calculate the degree of risk in a population using:
- Absolute risk - incidence rate, specific rates
- Relative risk - comparison between exposed and non-exposed groups
- Attributable risk - the portion of risk attributable to a specific exposure
Classic examples:
- Risk of bearing a child with Down syndrome (trisomy 21)
- Risk assessment for smokers vs. non-smokers for cancer and CHD
5. Syndrome Identification
Epidemiological investigations help define and refine disease syndromes by correcting misconceptions arising from individual clinical observation.
Examples:
- Differentiation of gastric vs. duodenal ulcer - a "poverty gradient" in gastric ulcer certification but not in duodenal ulcer led to recognition of two distinct entities (before 1920 this distinction was poorly understood).
- Testing the Paterson-Kelly syndrome (dysphagia + iron-deficiency anaemia) epidemiologically showed the association was not supported.
- Distinct subtypes of essential hypertension identified via plasma renin levels.
6. Completing the Natural History of Disease
Epidemiology is concerned with the entire spectrum of disease across a population - not just hospital cases, which give a skewed picture.
- The epidemiologist studies disease in the community in relation to agent, host, and environmental factors.
- Example: Epidemiology revealed that one-third to two-thirds of deaths from ischaemic heart disease are sudden (within less than one hour). Most victims never reach the hospital. This finding gave tremendous impetus to the development of intensive coronary care units (ICCUs).
7. Searching for Causes and Risk Factors
This is the classic use of epidemiology - identifying causes by relating disease to interpopulation differences and population attributes.
Notable causal discoveries through epidemiology:
- Rubella as a cause of congenital defects in the newborn
- Thalidomide as a teratogenic agent
- Cigarette smoking as a cause of lung cancer
- Excess oxygen exposure in premature babies as the cause of retrolental fibroplasia
For chronic diseases, a single cause is rarely found, but the search for "risk factors" - a key conceptual shift - has given renewed impetus to epidemiological research.
Uses of Descriptive Epidemiology (additionally)
Descriptive studies specifically:
- Provide data on the magnitude of disease load (morbidity and mortality rates)
- Provide clues to disease aetiology and help formulate aetiological hypotheses
- Provide background data for planning, organising, and evaluating preventive and curative services
- Contribute to research by describing variations in disease occurrence by time, place, and person
Source: Park's Textbook of Preventive and Social Medicine (Morris's classification), pp. 104-106
Define a carrier role in disease transmission
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have all the content needed for a complete answer. Here it is:
The Carrier: Role in Disease Transmission
Definition
A carrier is defined as:
"An infected person or animal that harbours a specific infectious agent in the absence of discernible clinical disease and serves as a potential source of infection for others."
A carrier state arises when, due to inadequate treatment or immune response, the disease agent is not completely eliminated from the body.
Elements of a Carrier State
Three conditions must be present:
- Presence of the disease agent in the body
- Absence of recognizable symptoms and signs of disease
- Shedding of the disease agent in discharges or excretions, thus acting as a source of infection for others
Why Carriers Are Epidemiologically Dangerous
As a rule, carriers are less infectious than clinical cases, but they are more dangerous because:
- They escape recognition - neither they nor others know they are infected
- They continue living a normal life in the community
- They can infect susceptible individuals over a wider area and longer period of time under favourable conditions
The classic historical example is "Typhoid Mary" (Mary Mallon), a cook who was a chronic typhoid carrier and spread the disease to dozens of people without ever falling ill herself.
Classification of Carriers
A. By Type
(a) Incubatory Carriers
- Shed the infectious agent during the incubation period, before clinical illness begins
- Capable of infecting others before the onset of their own symptoms
- Usually occurs during the last few days of the incubation period
- Examples: measles, mumps, polio, pertussis, influenza, diphtheria, hepatitis B
(b) Convalescent Carriers
- Continue to shed the disease agent during the period of convalescence (after clinical recovery)
- Clinical recovery does NOT coincide with bacteriological recovery
- Example: A typhoid fever patient may excrete the bacilli for 6-8 weeks after recovery - posing a serious threat to household members
- Other examples: dysentery (bacillary and amoebic), cholera, diphtheria, whooping cough
- Highlights the importance of bacteriological surveillance after clinical recovery
(c) Healthy Carriers
- Emerge from subclinical (inapparent) infection - they never had overt disease but shed the agent
- Examples: poliomyelitis, cholera, meningococcal meningitis, salmonellosis, diphtheria
- Important note: not all subclinical infections lead to carrier state. In polio, a subclinical case may act as a temporary carrier; in tuberculosis, most persons with a positive tuberculin test do NOT actively disseminate bacilli and are not labelled carriers.
B. By Duration
(a) Temporary Carriers
- Shed the infectious agent for short periods of time
- Includes incubatory, convalescent, and healthy carriers
(b) Chronic Carriers
- Excrete the infectious agent for indefinite periods
- Diseases: typhoid fever, hepatitis B, dysentery, cerebrospinal meningitis, malaria, gonorrhoea
- Far more important sources of infection than cases - the longer the carrier state, the greater the risk to the community
- Some excrete intermittently, some continuously
- Duration varies by disease: in typhoid fever and hepatitis B, may last several years; in chronic dysentery, a year or longer
- In diphtheria, carrier state is associated with infected tonsils; in typhoid fever with gall bladder disease
- Chronic carriers can reintroduce disease into areas otherwise free of infection (e.g., malaria)
- Early detection and treatment are essential to limit the spread
C. By Portal of Exit
| Portal | Examples |
|---|---|
| Urinary | Typhoid, leptospirosis |
| Intestinal | Cholera, typhoid, dysentery, hepatitis A |
| Respiratory | Diphtheria, meningococcal meningitis, TB |
| Others | Skin, blood (malaria via mosquito) |
Special Note: Pseudo-Carriers
- Carriers of avirulent (non-disease-causing) organisms are called pseudo-carriers
- Pseudo-carriers are not important epidemiologically as they cannot cause disease in others
Source: Park's Textbook of Preventive and Social Medicine, pp. 107-108
Edverse event following immunization
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content. Here is the full answer:
Adverse Events Following Immunization (AEFI)
Definition
An AEFI is any untoward medical occurrence which follows immunization and which does not necessarily have a causal relationship with the usage of the vaccine. The adverse event may be any unfavourable or unintended sign, abnormal laboratory finding, symptom or disease.
Reported AEFIs can be:
- True adverse events - genuinely a result of the vaccine or immunization process
- Coincidental events - not due to the vaccine but temporally associated with immunization
Vaccines used in national immunization programmes are extremely safe and effective; however, no immune response is entirely free from the risk of adverse reactions or remote sequelae.
CIOMS/WHO 2012 Cause-Specific Classification of AEFIs
In 2012, the Council for International Organizations of Medical Sciences (CIOMS) and WHO introduced a new cause-specific categorization:
| Cause-Specific Type | Definition |
|---|---|
| Vaccine product-related reaction | An AEFI caused or precipitated by a vaccine due to one or more of its inherent properties, even when prepared, handled and administered correctly |
| Vaccine quality defect-related reaction | An AEFI caused by a manufacturing quality defect in the vaccine. Very rare today due to improved Good Manufacturing Practices (GMP) - historically the Cutter Incident is a classic example |
| Immunization error-related reaction | An AEFI caused by an error in vaccine preparation, handling, or administration (programme error) - preventable |
| Immunization anxiety-related reaction | An AEFI arising from anxiety about the immunization itself (e.g., vasovagal syncope/fainting) |
| Coincidental event | An AEFI that occurs after immunization but is not caused by it - would have occurred regardless |
"Immunization" includes all processes after a vaccine leaves the manufacturing site: handling, prescribing and administration.
1. Common Minor Vaccine Reactions
The immune system reacts to a vaccine to build immunity - local and systemic reactions are part of this response.
Local reactions (pain, swelling, redness at injection site):
- Occur in about 10% of vaccinees
- DTP (whole cell) or tetanus boosters: up to 50% affected
- BCG produces a specific reaction: papule 2+ weeks post-immunization → ulcerates → heals in months → leaves a scar. Keloid formation is more common among Asian and African populations
Systemic reactions (fever, irritability, malaise, loss of appetite):
- Fever in ~10% or less, except DTP (~50%)
- Measles vaccine: fever, rash, conjunctivitis in 5-15% (mild compared to wild measles; can be severe in immunocompromised)
- Mumps (swollen parotid) and rubella (joint pains, lymph nodes): <1% in children; rubella causes joint pains in up to 15% of adults
- OPV: systemic reactions <1%
2. Rare but Serious Vaccine Reactions
| Vaccine | Reaction | Onset Interval | Rate per Doses |
|---|---|---|---|
| BCG | Suppurative lymphadenitis | 2-6 months | 1-10/10,000 |
| BCG | BCG osteitis | 1-12 months | 1-700/1,000,000 |
| BCG | Disseminated BCG infection | 1-12 months | 0.19-1.56/1,000,000 |
| Hepatitis B | Anaphylaxis | 0-1 hour | 1.1/1,000,000 |
| Influenza (inactivated) | Guillain-Barre syndrome | - | 1-2/1,000,000 |
| Influenza (live) | Wheezing (children 6-11 months) | - | 14/100 |
| OPV | Vaccine-associated paralytic polio (VAPP) | 4-30 days | - |
| MMR/Measles | Thrombocytopenia | 15-35 days | - |
| Rotavirus | Intussusception | Shortly after | - |
Most rare and serious reactions (seizures, thrombocytopenia, HHE, persistent screaming) do not lead to long-term problems. Anaphylaxis, while potentially fatal, is treatable without long-term effects.
3. Serious vs. Severe: An Important Distinction
These terms are NOT interchangeable:
- Serious: An AEFI that results in death, is life-threatening, requires hospitalization, causes persistent disability/incapacity, is a congenital anomaly, or requires intervention to prevent permanent impairment
- Severe: Describes the intensity of an event (mild/moderate/severe) - the event itself may be of minor medical significance (e.g., mild fever vs. moderate fever). Anaphylaxis is always both serious AND severe.
4. Case Definitions and Treatment of Specific AEFIs
| Adverse Event | Case Definition | Treatment | Vaccine |
|---|---|---|---|
| Acute flaccid paralysis (VAPP) | Flaccid paralysis 4-30 days after OPV (or 4-75 days after contact); vaccine virus isolated; neurological deficits persist 60 days | Supportive care only | OPV |
| Anaphylactoid reaction | Wheezing, bronchospasm, laryngospasm, or skin manifestations within 2 hours of immunization | Self-limiting; antihistamines | All |
| Anaphylaxis | Severe immediate allergic reaction (<1 hour); circulatory failure ± bronchospasm/laryngospasm | Adrenaline injection | All |
| Encephalopathy | Any two of: seizures, severe altered consciousness ≥1 day, distinct behaviour change ≥1 day; within 48 hrs of DTP or 7-12 days after measles/MMR | Supportive care | Measles, Pertussis |
| Brachial neuritis | Deep severe aching pain in shoulder/upper arm followed by weakness and wasting; sensory loss possible | Analgesics | Tetanus |
| Disseminated BCG infection | Widespread infection 1-12 months post-BCG; M. bovis BCG strain isolated; usually immunocompromised | Anti-TB regimen (isoniazid + rifampicin) | BCG |
5. Fainting vs. Anaphylaxis - Key Differences
| Feature | Fainting | Anaphylaxis |
|---|---|---|
| Skin | Pallor, cold clammy | Itching, urticaria, swelling of lips/face |
| Respiratory | Normal/shallow | Wheezing, stridor, cyanosis |
| Cardiovascular | Bradycardia; hypotension reversed by supine position | Tachycardia; hypotension NOT reversed by supine |
| CNS | Relieved by lying down | Anxiety, distress, loss of consciousness; not relieved by supine |
6. Events That Should Be Reported
| Time After Immunization | Reportable Events |
|---|---|
| Within 24-48 hours | Anaphylaxis, anaphylactoid reaction, persistent screaming (>3 hrs), hypotonic-hyporesponsive episode (HHE), toxic shock syndrome (TSS) |
| Within 7 days | Severe local reaction, sepsis, injection site abscess (bacterial/sterile) |
| Within 14 days | Seizures/febrile seizures (6-12 days for measles/MMR; 0-2 days for DTP), encephalopathy |
| Within 3 months | Acute flaccid paralysis (4-30 days for OPV recipient; 4-75 days for contact) |
| 1-12 months after BCG | Lymphadenitis, disseminated BCG infection, osteitis/osteomyelitis |
| No time limit | Any death, hospitalization, disability, or other severe/unusual event thought to be related to immunization |
Minor common reactions such as local reactions, fever, and self-limiting symptoms need not be reported.
7. Investigating AEFI Clusters
A cluster of AEFI = two or more cases of the same adverse event related in time, place or vaccine administration.
Decision-making flowchart for AEFI clusters:
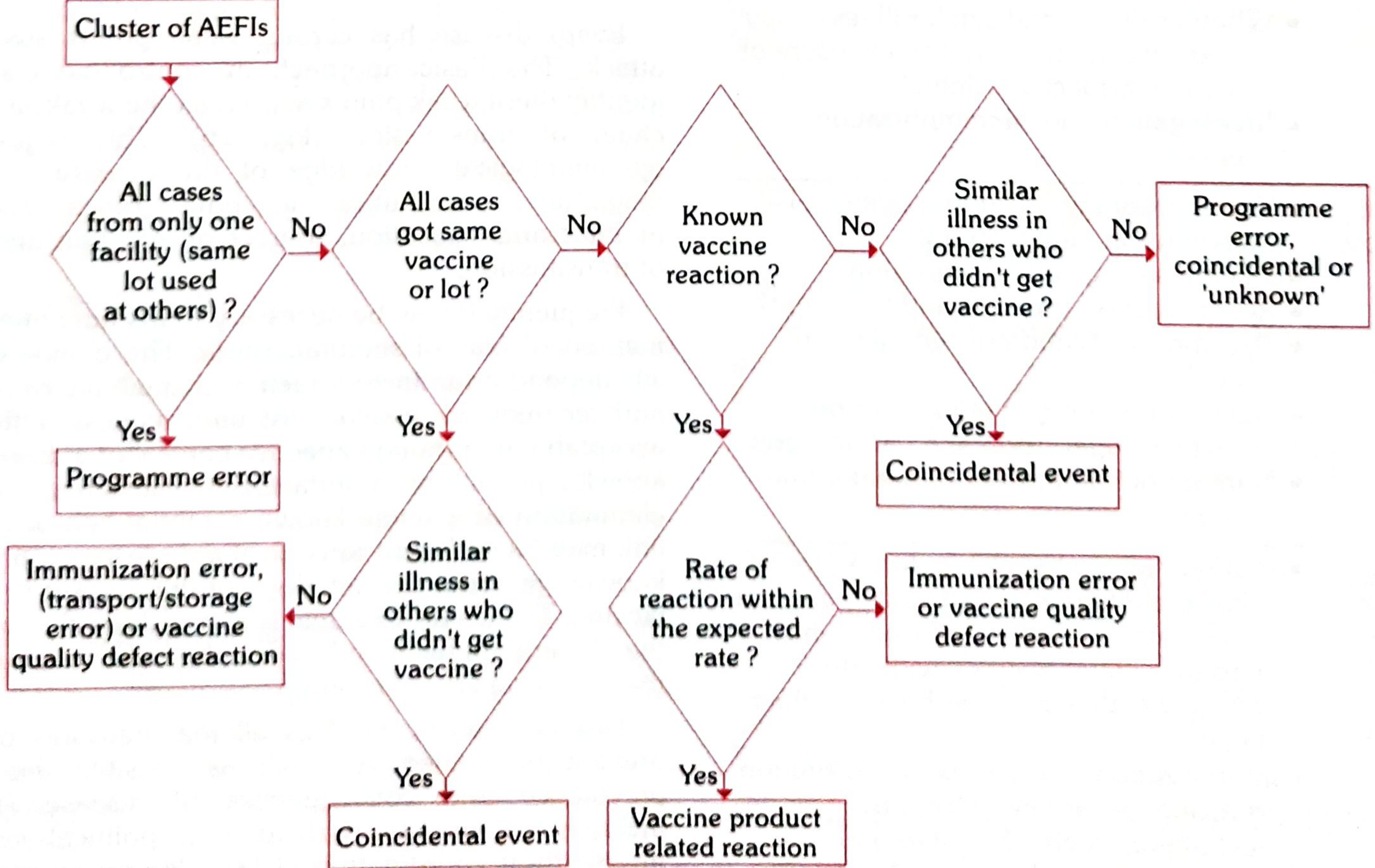
Key principles:
- If all cases from one facility (same lot) → Programme error
- If all got the same vaccine/lot and it's a known reaction occurring at expected rate → Vaccine product-related reaction
- If the event also occurred in unimmunized people → Coincidental event
- If it's a known reaction occurring at an increased rate → Programme error or vaccine quality defect
8. Steps in an AEFI Investigation
- Confirm information - Obtain medical records, identify other cases
- Investigate and collect data - Patient history, immunization history, prior allergies, clinical description, vaccine storage conditions
- Assess the service - Vaccine storage, reconstitution process, syringe/needle sterilization, training of vaccinators
- Formulate a working hypothesis on the likely cause
- Test the hypothesis - Does case distribution match? Are laboratory tests needed?
- Conclude investigation - Reach a conclusion, complete AEFI Investigation Form, take corrective action
Source: Park's Textbook of Preventive and Social Medicine, pp. 127-134 (CIOMS/WHO 2012 classification)
Health advise to international traveler
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content from Harrison's and Fordtran's. Here is the full detailed answer:
Health Advice to International Travelers
Why Travel Medicine Matters
As many as 43-79% of travelers to low- and middle-income countries report developing a travel-related illness. International air travel now allows the globe to be circumnavigated in <24 hours - shorter than the incubation period of almost all infections - meaning infected travelers can arrive at destinations before symptoms begin. Epidemics such as SARS (2003), Ebola (2014), and COVID-19 (2020) illustrate this risk vividly.
Most illnesses are minor, but fewer than 1-3% of travelers require hospitalization. Notably, the most common causes of death in travelers are not infections but cardiovascular events, motor vehicle accidents, drowning, homicide, and suicide.
Pre-Travel Consultation: Key Elements
A pre-travel consultation should cover five core areas:
| Element | Key Questions |
|---|---|
| Risk Assessment | Destination, duration, accommodations, activities, altitude, reason for travel |
| Traveler Profile | Age, medical history, medications, allergies, pregnancy status, immune status |
| Immunizations | Routine, recommended, and required vaccines for the itinerary |
| Malaria & Arthropod-borne Infection Prevention | Destination risk, local drug resistance, chemoprophylaxis choice |
| GI illness, Injuries, and Other Conditions | Food/water safety, STIs, altitude illness, jet lag, VTE |
The CDC Travelers' Health website provides comprehensive, up-to-date country-specific recommendations on vaccinations, malaria chemoprophylaxis, and travel health notices.
1. Immunizations
Vaccines are classified as routine, recommended, or required:
- Routine vaccines - all travelers should be up to date: influenza, COVID-19, tetanus-diphtheria-pertussis, MMR, varicella, pneumococcal (if indicated)
- Recommended vaccines based on destination and activities:
- Hepatitis A - most common vaccine-preventable illness in travelers
- Typhoid - recommended for travel to South Asia, sub-Saharan Africa, South America
- Hepatitis B - if not already immunized
- Yellow fever - required for entry to certain countries in Africa and South America; certificate needed
- Meningococcal - required for Hajj pilgrims; recommended for sub-Saharan Africa meningitis belt
- Japanese encephalitis - for rural travel to Asia
- Rabies - for remote destinations, outdoor activities, prolonged stays
- Cholera - for aid workers or high-risk areas
- Chikungunya - a live vaccine approved in the US (2023) for adults ≥18 years at increased risk; single dose; contraindicated in immunocompromised
- Required vaccines: Yellow fever certificate (International Certificate of Vaccination or Prophylaxis - ICVP) is legally required for entry into some countries
2. Malaria Prevention
Malaria is the leading cause of life-threatening infections in travelers. The disease burden is highest in sub-Saharan Africa (P. falciparum). In the US, nearly all of the ~1823 cases reported annually were acquired during travel - most patients had not taken chemoprophylaxis, had been inconsistent, or took the wrong regimen.
Mosquito Avoidance (Anopheles mosquitoes bite dusk to dawn)
- Wear long-sleeved shirts and long pants
- Apply DEET 20-50% insect repellent to exposed skin (preferred by CDC and WHO)
- Consider permethrin-treated clothing
- Sleep under insecticide-treated bed nets if not in well-screened accommodation
- Limit outdoor activity between dusk and dawn
Malaria Chemoprophylaxis
| Drug | Use | Timing |
|---|---|---|
| Atovaquone-proguanil (Malarone) | All areas including chloroquine-resistant | Start 1-2 days before; take daily; stop 7 days after return |
| Doxycycline | All areas including chloroquine-resistant | Start 1-2 days before; take daily; stop 4 weeks after return |
| Mefloquine | Areas without mefloquine resistance | Start 2-3 weeks before; weekly dosing; stop 4 weeks after return |
| Chloroquine | Limited to chloroquine-sensitive areas only | Weekly dosing |
- Significant hepatic or renal impairment affects the choice of prophylaxis
- Drug-drug interactions with regular medications must be checked
- Prophylaxis reduces risk but does not eliminate it - any fever during or after travel should prompt urgent evaluation for malaria
3. Other Arthropod-borne Infections
- Dengue fever - leading cause of fever in travelers returning from most tropical destinations outside sub-Saharan Africa. No FDA-approved dengue vaccine for US travelers (Dengvaxia limited to residents with prior infection; Qdenga approved in EU for age ≥4). Personal mosquito protection (Aedes mosquitoes bite day and night) is the main strategy.
- Chikungunya - causes severe arthralgias that can become chronic; vaccine available for high-risk adults ≥18 years
- Zika - major concern for pregnant women; DEET and barrier contraception essential
- Yellow fever - use personal protection + vaccination for endemic areas
4. Travelers' Diarrhea
Definition: ≥3 unformed stools plus at least 1 accompanying symptom (nausea, vomiting, cramps, fever, bloody stool) in 24 hours.
- Affects an estimated 25-50% of travelers to developing countries
- 90% are brief and self-limited (1-5 days)
- 5-10% develop dysentery; 1-2% have persistent diarrhea >2 weeks
- 3-17% develop post-infection IBS
High-Risk Destinations
South Asia, sub-Saharan Africa, South America (highest risk) vs. North America, Japan, Australia, Europe (lowest risk)
Common Causes
- Bacterial (60-80% of cases): ETEC and EAEC account for 50-75% overall; regional variation - Campylobacter and Salmonella common in Southeast Asia; Shigella in Africa and South Asia
- Viral: Norovirus ~15% of cases
- Parasitic (Giardia, Entamoeba histolytica, Cryptosporidium): more common in prolonged diarrhea (>14 days)
Prevention
- Eat only thoroughly cooked hot foods
- Avoid raw vegetables, unpeeled fruits, shellfish, street food
- Drink bottled or boiled water; avoid ice in low-resource settings
- "Boil it, cook it, peel it, or forget it"
Treatment
| Severity | Treatment |
|---|---|
| Mild | Oral rehydration (soups, electrolyte solutions); avoid dairy; bismuth subsalicylate (Pepto-Bismol) or loperamide |
| Moderate-severe | Antibiotics: Azithromycin 500-1000 mg single dose (preferred, esp. Southeast Asia for resistant Campylobacter); Ciprofloxacin 750 mg single dose; Rifaximin 200 mg TID x 3 days (for non-invasive E. coli only) |
| Seek care when: | Volume depletion, high fever, bloody stool, severe abdominal pain, immunocompromised, persistent >14 days |
Antibiotic prophylaxis is not recommended routinely - reserved for highly selected high-risk individuals only (immunocompromised, high-stakes travel with no access to care).
5. Food and Water Safety Summary
- Boil water for 1 minute (3 minutes at altitude >2000 m) OR use iodine/chlorine tablets OR use a filtration device
- Safe foods: hot cooked foods, fruits you peel yourself, pasteurized dairy
- Avoid: raw/undercooked meat and seafood, unpasteurized dairy, tap water, ice, raw salads in high-risk areas
6. Other Important Health Topics
Altitude Illness
- Risk at >2500 m; symptoms include headache, nausea, fatigue, dizziness
- Prevention: ascend gradually (≤300-500 m/day above 3000 m), rest, stay hydrated
- Acetazolamide (Diamox) 125-250 mg BD starting 1-2 days before ascent is recommended prophylaxis for those ascending rapidly
- Dexamethasone for treatment of high-altitude cerebral oedema (HACE)
Venous Thromboembolism (VTE)
- Long-haul flights (>4 hours) increase DVT risk, especially in high-risk individuals
- Advice: stay hydrated, move around the cabin, perform leg exercises, wear graduated compression stockings
- Anticoagulant prophylaxis for very high-risk travelers (prior DVT/PE, known thrombophilia, recent surgery)
Jet Lag
- Due to disruption of circadian rhythm crossing multiple time zones
- Short-acting hypnotics (e.g., zolpidem) and melatonin (0.5-5 mg at destination bedtime) can help adaptation
Sexually Transmitted Infections
- Incidence of STIs increases significantly during travel
- Carry and use condoms; pre-exposure prophylaxis (PrEP) for HIV-negative travelers at risk
- Hepatitis B vaccination if not already immune
Animal Bites and Rabies
- Avoid petting or approaching stray animals, dogs, bats, monkeys
- Pre-exposure rabies vaccination for travelers to remote destinations, children, and those with occupational exposure
- Any animal bite: wash wound immediately with soap and water for at least 15 minutes; seek post-exposure prophylaxis (PEP) urgently
Injury and Crime Prevention
- Avoid motorcycles/motorbikes - major cause of injury deaths
- Use seatbelts; avoid night driving in low-resource settings
- Be aware of personal security; avoid ostentatious displays of wealth
Mental Health
- Travel-related stress can exacerbate or unmask psychiatric disorders
- Depression and anxiety are common reasons for medical evacuation
7. Returning Traveler - Post-Travel Screening
- Any fever within 3 months of return from a malaria-endemic area = malaria until proven otherwise - urgent blood films required
- Persistent diarrhea >14 days: stool microscopy and culture for parasites
- Jaundice: consider hepatitis A/B/E, leptospirosis, malaria
- Skin lesions: consider cutaneous leishmaniasis, myiasis, larva migrans
- Unexplained eosinophilia: helminth infections (schistosomiasis, strongyloides, filariasis)
Special Traveler Groups
| Group | Key Concerns |
|---|---|
| Pregnant women | Avoid malaria-endemic areas if possible; chloroquine safe in pregnancy; mefloquine generally avoided in first trimester; Zika risk; live vaccines contraindicated |
| Immunocompromised | Live vaccines contraindicated; higher malaria risk; strict food/water precautions |
| Elderly | Cardiovascular risk; VTE prevention; heat stress |
| VFR travelers (visiting friends/relatives) | Higher risk - often do not seek pre-travel advice, more likely to travel to rural areas, less likely to take prophylaxis |
| Infants and children | Age-appropriate doses; some antimalarials not suitable for young children |
Sources: Harrison's Principles of Internal Medicine 22E (2025), Chapter 130, pp. 1054-1056; Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chapter 110, pp. 2205-2206
This is a shared conversation. Sign in to Orris to start your own chat.