Full treatment regimen for the mamagement of DM type 1
Reading File
Finding Sources
Searching PubMed
"type 1 diabetes"[MeSH Terms] AND "management"[MeSH Terms]
Searching the Web
type 1 diabetes mellitus management treatment regimen 2025 guidelines
Finding Sources
Finding Sources
Searching PubMed
"type 1 diabetes"[MeSH Terms] AND "insulin therapy"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to write a comprehensive, well-structured answer. Here is the full treatment regimen for Type 1 Diabetes Mellitus:
Treatment Regimen for Type 1 Diabetes Mellitus (T1DM)
T1DM is characterized by autoimmune destruction of pancreatic β-cells resulting in absolute insulin deficiency. Management requires lifelong exogenous insulin, glucose monitoring, dietary planning, and prevention of complications. All patients with T1DM should be primarily managed by an endocrinologist or in close concert with one.
1. Insulin Therapy - The Cornerstone
Every person with T1DM requires exogenous insulin to sustain life. The goal is to mimic the physiologic pattern of basal insulin secretion plus mealtime (prandial) boluses.
Insulin Preparations
| Type | Examples | Onset | Peak | Duration |
|---|---|---|---|---|
| Rapid-acting analogues | Lispro, Aspart, Glulisine | 15-30 min | 30-90 min | 3-4 hrs |
| Short-acting (Regular) | Human insulin (U100, U500) | ~30 min | 2-4 hrs | 5-8 hrs |
| Intermediate (NPH) | Isophane insulin | 1-2 hrs | 4-8 hrs | 12-16 hrs |
| Long-acting analogues | Glargine, Detemir, Degludec | 2-4 hrs | Flat/peakless | 20-24+ hrs |
| Premixed | NPH/Regular 70:30 | Variable | Variable | Variable |
Rapid-acting and long-acting analogues cause less hypoglycemia and weight gain compared to human insulins, though they are more expensive. - Goldman-Cecil Medicine, p. 2474
A. Multiple Daily Injections (MDI) - Basal-Bolus Regimen
The preferred strategy for most patients with T1DM:
- Total daily dose (TDD): 0.3 to 1.0 unit/kg/day
- Basal insulin: ~50% of TDD given as long-acting analogue (glargine, detemir, or degludec) once or twice daily
- Prandial bolus: Remaining ~50% divided as rapid-acting analogue before each meal
- Dosing rule: 1 unit per 10-15 g of carbohydrate consumed + a correction factor of 1 unit to lower plasma glucose by 20-50 mg/dL above target
- Regular insulin: inject 30 minutes before meals; rapid-acting analogues: inject 15 minutes before or 15-20 minutes after starting a meal
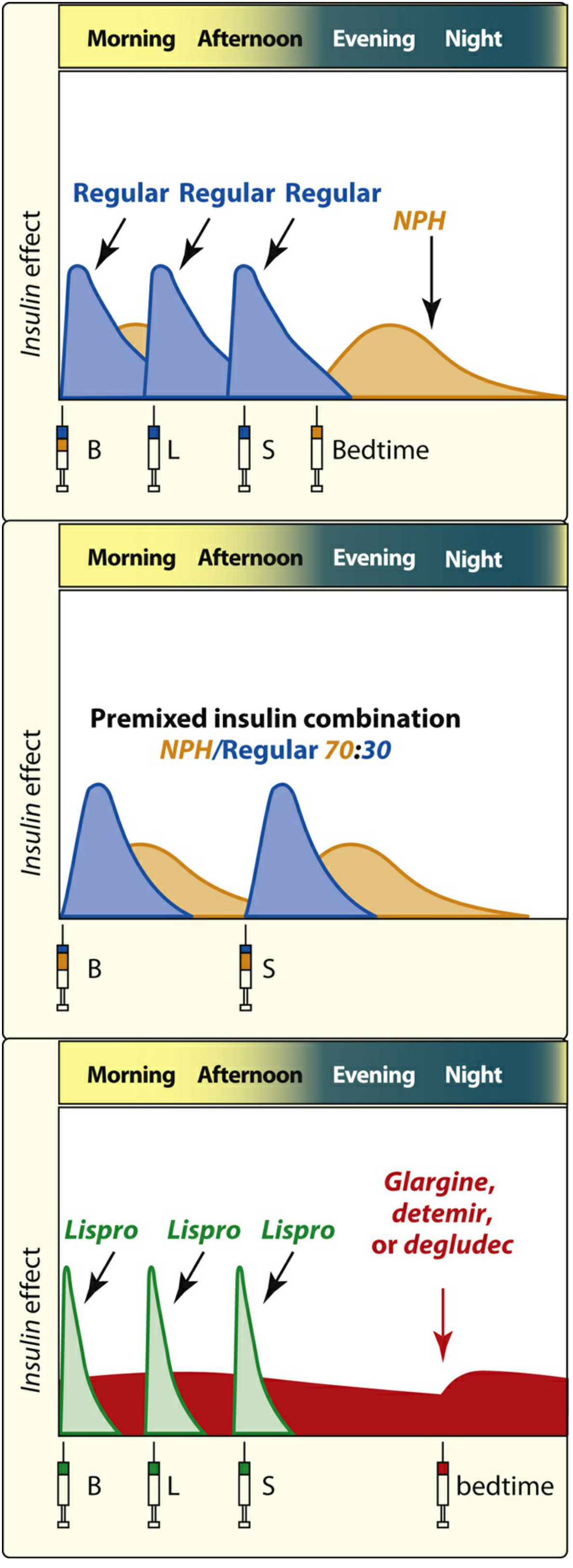
Figure: Examples of three insulin regimens providing both prandial and basal insulin replacement. B = breakfast, L = lunch, S = supper. - Lippincott Illustrated Reviews: Pharmacology
B. Standard (Twice-Daily) Regimen
Used in select patients (e.g., very young children, limited resources):
- Twice-daily injections combining NPH with regular or rapid-acting insulin
- Less flexible but reduces injection frequency
- Less likely to achieve target HbA1c compared to MDI
C. Inhaled Insulin
- Available for rapid-acting prandial use (Afrezza)
- Onset even faster than subcutaneous rapid-acting analogues (peak within 10-20 minutes)
- Rarely recommended; reserved for specialized centers
2. Continuous Subcutaneous Insulin Infusion (CSII) - Insulin Pump
CSII delivers rapid-acting insulin analogue continuously via a small subcutaneous catheter changed every 2-3 days.
- HbA1c reduction: 0.3-0.5% vs MDI
- Advantages: Reduces severe hypoglycemia, allows programmable variable basal rates (including adjustment for the "dawn phenomenon"), allows bolus dosing based on carbohydrate content + glucose corrections, more flexible lifestyle
- Infusion sites: Abdomen, flanks, upper legs, arms
- Tubeless systems available for greater convenience
- Patients must be able to revert quickly to MDI injections in case of pump failure (DKA can develop within hours given the short half-life of insulin ~5-10 minutes and no long-acting depot)
Goldman-Cecil Medicine, p. 2474
3. Sensor-Augmented Pump and Continuous Glucose Monitoring (CGM)
- CGM devices measure interstitial glucose continuously, providing real-time trends
- Sensor-augmented pumps (CGM + CSII) improve HbA1c by -0.4 to -0.6% vs standard MDI, and reduce hypoglycemia risk
- Features include automatic insulin suspension when low glucose predicted, alarms for out-of-range values
4. Closed-Loop / Automated Insulin Delivery (AID) - "Artificial Pancreas"
The most advanced technology:
- Integrates real-time CGM + insulin pump + control algorithm
- Automatically adjusts insulin delivery every 5-10 minutes
- Can deliver automatic corrective boluses when glucose reaches a predetermined high threshold
- Reduces nighttime hypoglycemia, lowers HbA1c, reduces time-in-hypoglycemia
- Open-source systems (e.g., "Do-It-Yourself" loops) are also available
- Requires expert supervision and patient education
Goldman-Cecil Medicine, p. 2475
5. Glycemic Targets
| Parameter | Target (ADA) |
|---|---|
| Fasting plasma glucose | 80-130 mg/dL |
| Postprandial glucose (2h) | < 180 mg/dL |
| HbA1c | ≤ 7% (≤53 mmol/mol) for most patients |
| Time-in-range (CGM) | > 70% of readings between 70-180 mg/dL |
- Intensive therapy (3+ injections/day + frequent monitoring) achieves better HbA1c but carries higher risk of hypoglycemia, coma, and seizures compared to standard therapy
- Intensive therapy is not recommended for patients with long-standing disease, severe microvascular complications, advanced age, or hypoglycemia unawareness
- HbA1c ≥7.5% OR <5.6% both associate with increased all-cause mortality
Lippincott Illustrated Reviews: Pharmacology, p. 807; Goldman-Cecil Medicine, p. 2475
6. Blood Glucose Monitoring
- SMBG (self-monitoring): Several times daily before meals and at bedtime using portable meters
- CGM: Preferred over SMBG where accessible; provides continuous interstitial glucose readings
- Ketone monitoring: Test urine or capillary blood ketones when glucose is unexpectedly and persistently elevated; moderate/large ketones (≥2+ or >1.5 mmol/L) = seek urgent care for possible DKA
- Mobile apps and software assist with insulin dose calculations
7. Adjunctive (Non-Insulin) Therapies
These are used in addition to insulin, not as replacements:
Pramlintide (Amylin Analogue)
- Synthetic amylin given subcutaneously immediately before meals
- Delays gastric emptying, reduces postprandial glucagon, improves satiety
- Modestly lowers HbA1c by 0.3-0.5%; facilitates weight loss
- Starting dose: 15 mcg before meals, titrated to maintenance 120 mcg
- When initiating, reduce mealtime insulin dose by 50% to avoid severe hypoglycemia
- Adverse effects: nausea, anorexia, vomiting
- Contraindicated in gastroparesis, hypoglycemia unawareness
- Must not be mixed in the same syringe as insulin
Goldman-Cecil Medicine, p. 2474; Lippincott Illustrated Reviews: Pharmacology, p. 807
SGLT2 Inhibitors (off-label / approved in some countries)
- Dapagliflozin (low dose) and sotagliflozin (SGLT1/2 dual inhibitor)
- Lower HbA1c by 0.28-0.48%; facilitate weight loss through glycosuria
- Risk: Precipitate euglycemic DKA in 3-6% of T1DM patients
- Also increase risk of urinary tract and genital yeast infections
- Approved for T1DM in parts of Europe but not approved in the US or UK for T1DM
Goldman-Cecil Medicine, p. 2475
8. Diet and Lifestyle
- Carbohydrate counting is the preferred dietary approach - insulin dose matched to carbohydrate content of each meal (ratio may vary by time of day)
- Alternatively: meal-to-meal carbohydrate consistency with fixed premeal dosing
- Avoid rapidly absorbed carbohydrates ideally; caloric restriction only if overweight/obese
- Mediterranean diet recommended (heart-healthy, as for general population)
- Individualize based on food preferences, culture, finances, physical activity, glycemic targets
- Exercise: Adjust insulin and carbohydrate intake around physical activity; temporary basal rate reductions can be used in pump users during exercise
9. Management of Acute Complications
Hypoglycemia
- Treat with 15-20g of fast-acting carbohydrates (rule of 15)
- Glucagon (IM/SC/intranasal) for severe/unconscious patients
- Prevent by careful glucose monitoring, dose adjustments, patient education
Diabetic Ketoacidosis (DKA)
- Requires urgent IV fluid resuscitation, continuous IV insulin infusion, potassium replacement
- ADA 2025 guidelines include new treatment pathways for DKA (and HHS) with outlined transition to subcutaneous insulin
- Insulin pump use can continue in hospital when clinically appropriate (per 2025 ADA update)
10. Cardiovascular and Complication Monitoring/Prevention
| System | Screening/Intervention |
|---|---|
| Retinopathy | Annual dilated eye exam; tight glucose + BP control |
| Nephropathy | Annual urinary albumin + eGFR; RAAS inhibitors (ACE-I or ARB) for proteinuria |
| Neuropathy | Annual foot exam, monofilament testing |
| Cardiovascular | Statins for lipid lowering; aggressive BP control (RAAS inhibitors preferred); smoking cessation |
| Blood pressure target | <130/80 mmHg |
| LDL target | <100 mg/dL (or lower with established CVD) |
Intensive glucose control and adjunctive cardioprotective therapy have collectively reduced blindness, renal failure, and amputation rates to <1% in T1DM patients.
11. Disease-Modifying and Preventive Therapy
- Teplizumab (anti-CD3 monoclonal antibody): Approved for use in individuals at high risk for T1DM (≥2 positive autoantibodies + impaired glucose tolerance = Stage 2); a single 14-day course may delay progression to clinical T1DM by ~2 years in high-risk relatives
- Immunosuppressive agents (rituximab, cyclosporine, anti-CD3) slow early disease but effects are not sustained after withdrawal
12. Surgical / Experimental Options
- Whole pancreas transplantation: 5-year graft survival ~70%; reserved for patients already undergoing kidney transplant or those with severe metabolic instability/hypoglycemia unawareness unresponsive to conventional therapy; requires lifelong immunosuppression
- Islet cell transplantation: Experimental; limited availability; also requires immunosuppression
- Stem cell therapy: Active research area; not yet in routine use
Summary of Key Principles
- Insulin is mandatory - no alternative replaces it in T1DM
- Basal-bolus MDI or CSII are the preferred delivery strategies; closed-loop/AID systems represent the current gold standard when accessible
- CGM is preferred over SMBG for glucose monitoring
- HbA1c target ≤7% for most patients; individualize for special populations
- Carbohydrate counting with dose adjustment is the dietary cornerstone
- Multidisciplinary team (endocrinologist, diabetes educator, dietitian, ophthalmologist, nephrologist, podiatrist) is essential for long-term care
- Teplizumab is a recent disease-modifying option for high-risk pre-clinical T1DM
Sources: Goldman-Cecil Medicine, 2 Vol. Set (Chapter 210); Lippincott Illustrated Reviews: Pharmacology; Katzung's Basic & Clinical Pharmacology, 16e; ADA Standards of Medical Care in Diabetes 2025
This is a shared conversation. Sign in to Orris to start your own chat.