Explain internal capsule of brain in detailed and in simple way
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
I now have all the information and diagrams needed for a thorough, well-illustrated explanation. Let me write the full answer.
The Internal Capsule - A Complete, Simple Guide
What Is It?
The internal capsule is a thick, compact band of white matter (myelinated nerve fibers) located deep inside each cerebral hemisphere. Think of it as the brain's "highway interchange" - it carries virtually all the signals going down from the brain cortex to the spinal cord and brainstem, AND all the signals going up from the body to the cortex.
It is the largest projection fiber tract in the brain.
- Localization in Clinical Neurology, 8e, p. 31
Where Is It? (Location)
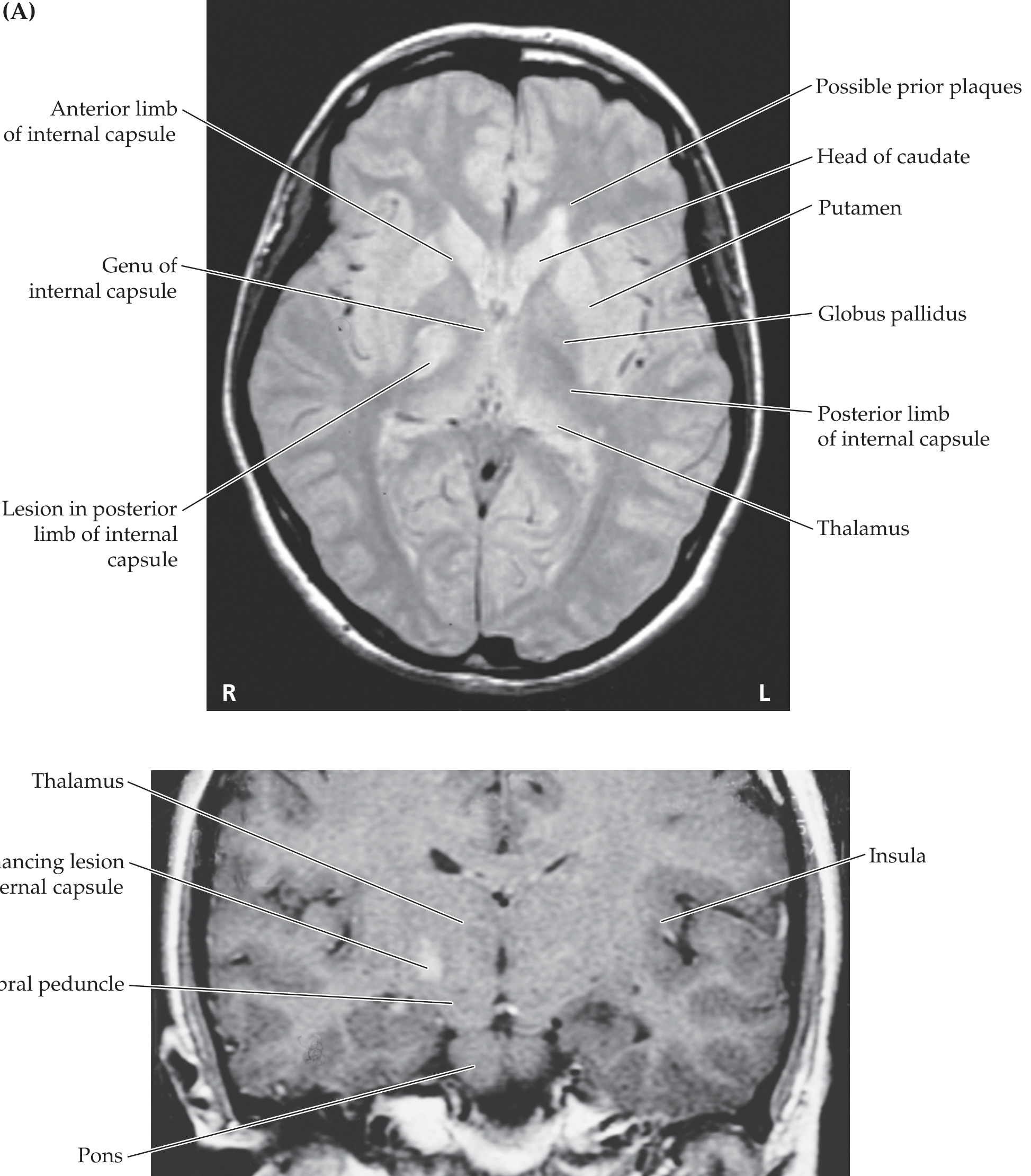
On a horizontal brain slice, the internal capsule sits like the letter "V" (or two arrowheads pointing inward). Its surrounding relationships are the most important thing to memorize:
| Direction | Structure |
|---|---|
| Medial | Caudate nucleus (front) and Thalamus (back) |
| Lateral | Lentiform nucleus = Putamen + Globus pallidus |
A simple trick: "TAIL" = Thalamus And Internal capsule are closer to midLine. The lentiform is always on the outside.
Above, the internal capsule fans out widely into the corona radiata (the white matter radiating to the cortex). Below, it narrows and continues as the cerebral peduncles of the midbrain.
Here is what it looks like on MRI - you can see the anterior limb, genu, and posterior limb clearly:
Parts of the Internal Capsule (5 Segments)
In a horizontal section, the internal capsule has 5 segments:
1. Anterior Limb
- ~2 cm long
- Sits between the head of the caudate (medial) and the lentiform nucleus (lateral)
- Also called the lenticulocaudate segment
2. Genu ("knee")
- The bend/corner of the V-shape, located at the level of the foramen of Monro
- "Genu" simply means knee in Latin
3. Posterior Limb
- ~3-4 cm long - the longest part
- Sits between the lentiform nucleus (lateral) and thalamus (medial)
- Also called the lenticulothalamic segment
- Contains the most clinically important fibers
4. Retrolenticular Segment
- Behind the lentiform nucleus (caudally)
5. Sublenticular Segment
- Below the lentiform nucleus (inferiorly)
What Fibers Run Through Each Part?
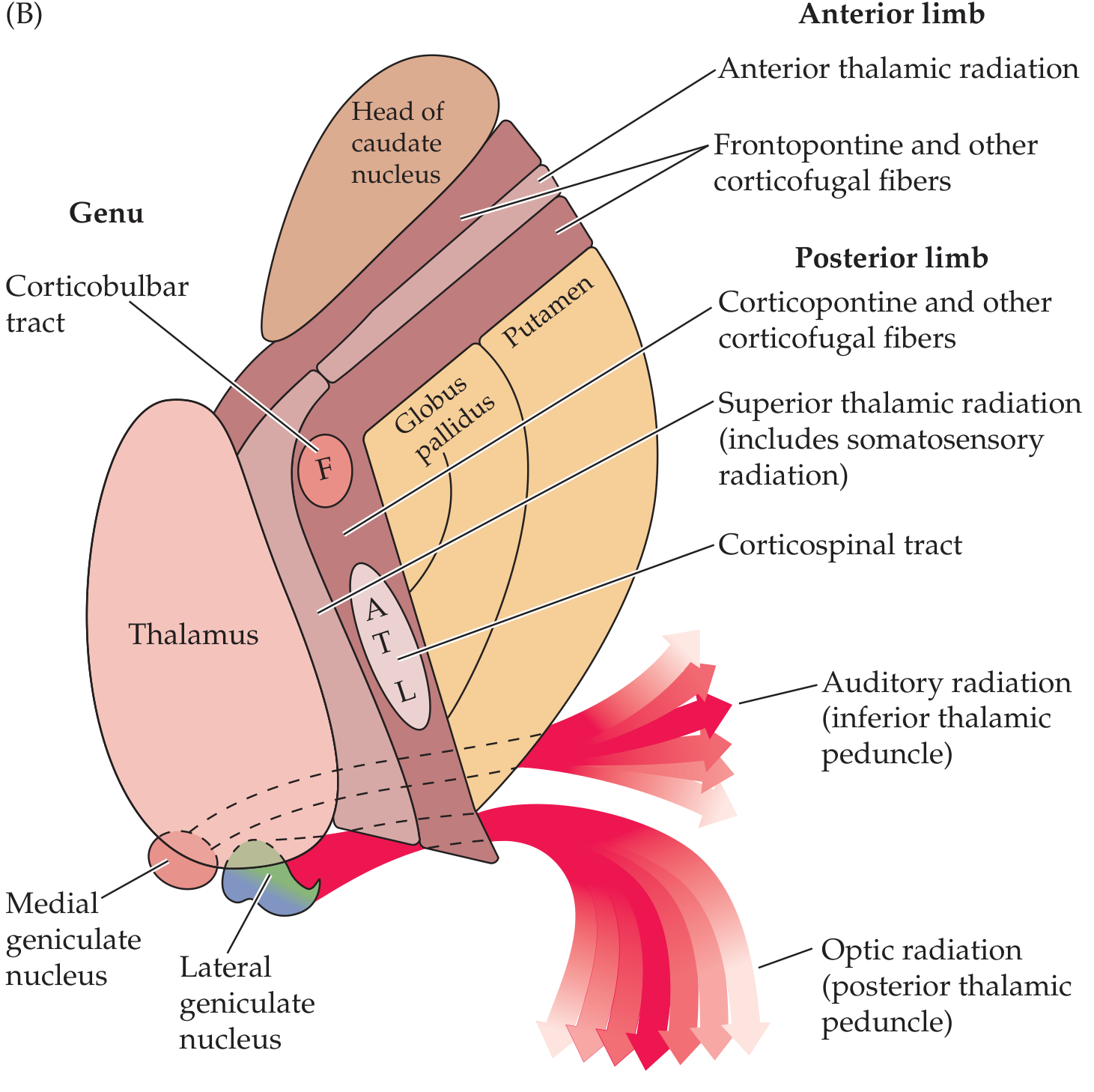
This is the most tested aspect. Here is the fiber map shown in the diagram:
| Segment | Fibers Passing Through |
|---|---|
| Anterior limb | Frontopontine fibers; anterior thalamic radiation (thalamocortical/corticothalamic connecting frontal lobe to thalamus); caudate-putaminal fibers |
| Genu | Corticobulbar tract (motor fibers to face, tongue - cranial nerves); corticoreticular fibers going to brainstem reticular formation |
| Posterior limb (anterior part) | Corticospinal tract - somatotopically arranged: face most anterior (F), then arm (A), then trunk (T), then leg (L) most posterior |
| Posterior limb (dorsal part) | Superior thalamic radiation (carries somatosensory information from thalamus to parietal cortex); corticorubral and corticothalamic fibers |
| Sublenticular segment | Auditory radiation (inferior thalamic peduncle) from medial geniculate to auditory cortex |
| Retrolenticular segment | Optic radiation (Gratiolet) from lateral geniculate to visual cortex (calcarine); corticotectal fibers |
The somatotopic arrangement in the posterior limb is easy to remember: Face - Arm - Trunk - Leg going from front to back (anterior to posterior).
- Neuroanatomy through Clinical Cases 3rd Edition, p. 257
Blood Supply
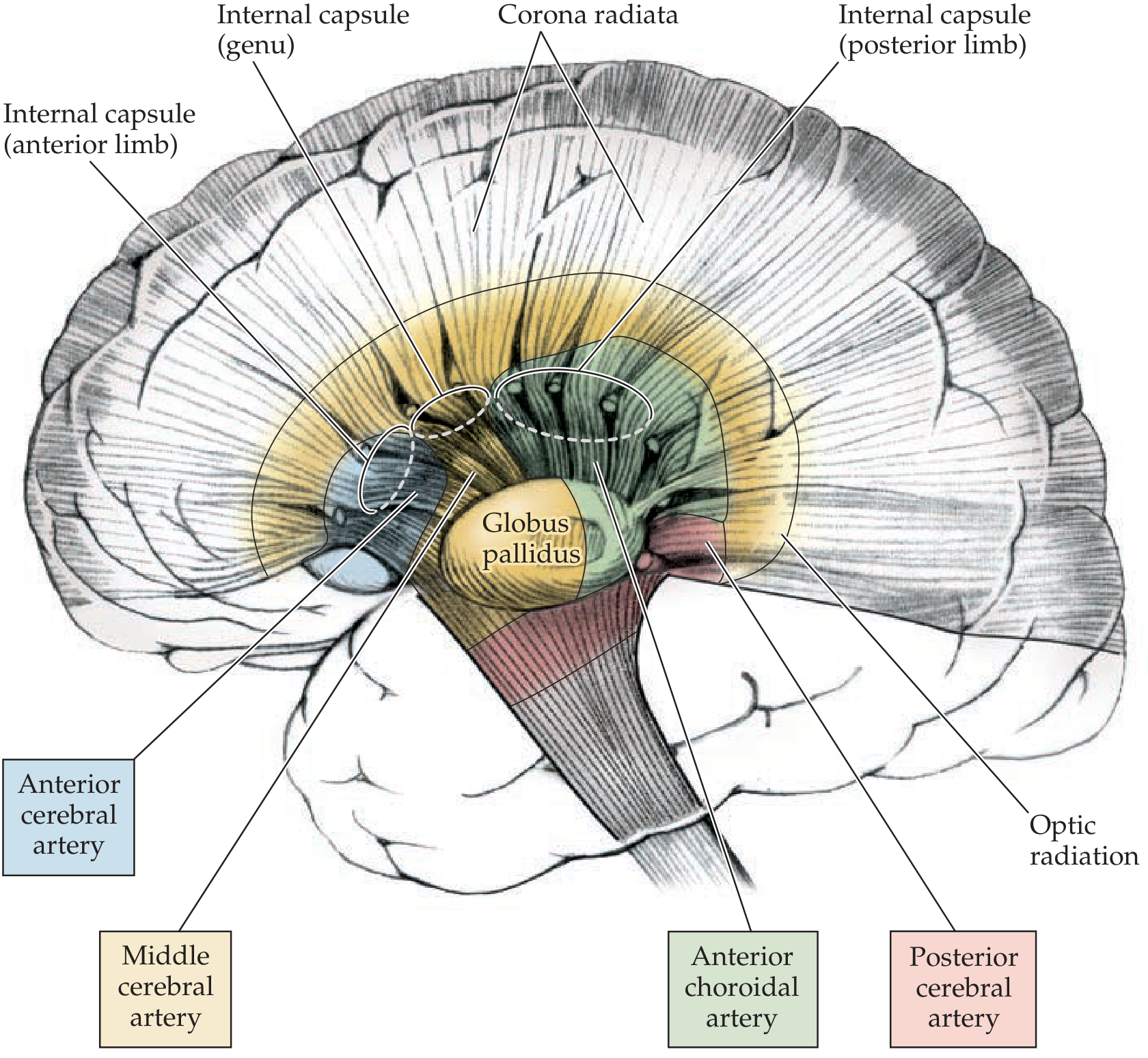
This is extremely important clinically. The internal capsule gets blood from three sources:
| Part of Internal Capsule | Blood Supply |
|---|---|
| Anterior limb (superior) | Lenticulostriate branches of the middle cerebral artery (MCA) |
| Anterior limb (inferior/medial) | Recurrent artery of Heubner (branch of anterior cerebral artery - ACA) |
| Genu + middle/inferior posterior limb | Anterior choroidal artery (branch of internal carotid) |
| Superior anterior + posterior limb | Lenticulostriate branches of the MCA |
The anterior choroidal artery is particularly important - it supplies the genu and most of the posterior limb.
- Localization in Clinical Neurology, 8e, p. 31
Why Is the Internal Capsule So Clinically Important?
Because all the motor and sensory fibers are tightly packed together here. A small stroke or hemorrhage causes devastating, widespread deficits.
Classic Syndromes
1. Pure Motor Hemiplegia (PMH) - most common capsular stroke syndrome
- Small lacunar infarct in the posterior limb
- Complete contralateral weakness of face + arm + leg (all three, because fibers are packed together)
- No sensory loss, no visual field defect
2. Genu Syndrome (Capsular Genu Syndrome)
- Lesion at the genu
- Facial and tongue weakness with only mild limb weakness
- This makes sense because the genu carries corticobulbar (cranial nerve motor) fibers
- May also cause dysarthria
3. Lateral and Posterior Capsular Lesion
Contralateral signs include:
- Hemiparesis
- Decreased pain and temperature
- Dysarthria
- Homonymous hemianopia (visual field loss)
- Memory impairment
- Visuoperceptual problems (with right-sided lesions)
- Bradley and Daroff's Neurology in Clinical Practice, p. 3297
4. Internal Capsular Hemorrhage
- Hemorrhage from small perforating arteries (lenticulostriates are prone to rupture in hypertension)
- Classically causes decorticate rigidity on the hemiplegic side
- May cause pure motor hemiplegia or mixed sensorimotor syndrome
- The small arteries of the internal capsule are especially prone to rupture or thrombosis in hypertension
Simple Way to Think About It - The Highway Analogy
Imagine the brain cortex as a busy city and the spinal cord/brainstem as a distant town. The internal capsule is the narrow highway tunnel that connects them.
- The anterior limb carries "planning and coordination" traffic (frontopontine connections)
- The genu carries "face control" traffic (corticobulbar)
- The posterior limb carries "main body movement and sensation" traffic (corticospinal + somatosensory)
- The retrolenticular/sublenticular parts carry "vision and hearing" traffic (optic and auditory radiations)
Because everything is squeezed into this narrow tunnel, even a tiny blockage (small lacunar infarct or hypertensive bleed) causes the entire opposite side of the body to stop working - that's why capsular strokes produce such dramatic deficits out of proportion to their small size.
Quick Summary Table
| Feature | Detail |
|---|---|
| Nature | White matter (myelinated axons) |
| Shape | V-shaped on horizontal section |
| Medial to it | Caudate + Thalamus |
| Lateral to it | Putamen + Globus pallidus |
| Above it | Corona radiata |
| Below it | Cerebral peduncles |
| Parts | Anterior limb, Genu, Posterior limb, Retrolenticular, Sublenticular |
| Key fibers | Corticospinal, corticobulbar, thalamocortical, optic radiation, auditory radiation |
| Blood supply | MCA lenticulostriates, anterior choroidal artery, ACA (Heubner) |
| Common lesion | Lacunar infarct or hypertensive hemorrhage |
| Classic deficit | Contralateral pure motor hemiplegia |
Sources: Neuroanatomy through Clinical Cases 3rd Edition; Localization in Clinical Neurology 8e; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.