treatment of uncontrolled DM with ketosis with ketouria 2+
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"diabetic ketoacidosis" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
I now have comprehensive, authoritative information to provide a detailed clinical answer. Let me synthesize it:
Treatment of Uncontrolled Diabetes with Ketosis and Ketonuria 2+
Clinical Context
Ketonuria 2+ in the setting of uncontrolled diabetes represents diabetic ketosis — a state that may range from mild DKA to severe DKA depending on accompanying acid-base status. Before treating, classify severity.
Step 1 — Severity Classification (ADA Criteria)
| Severity | Glucose | pH | HCO₃⁻ | Ketones | Mental Status |
|---|---|---|---|---|---|
| Mild | >250 mg/dL | 7.25–7.30 | 15–18 mmol/L | Positive | Alert |
| Moderate | >250 mg/dL | 7.00–7.24 | 10–15 mmol/L | Positive | Alert/Drowsy |
| Severe | >250 mg/dL | <7.00 | <10 mmol/L | Positive | Stupor/Coma |
Ketonuria 2+ indicates significant ketonemia. β-hydroxybutyrate >3.0 mmol/L confirms DKA; note that nitroprusside-based urine strips detect only acetoacetate/acetone, not β-hydroxybutyrate — so ketonuria may underestimate true severity.
Step 2 — Treatment Algorithm
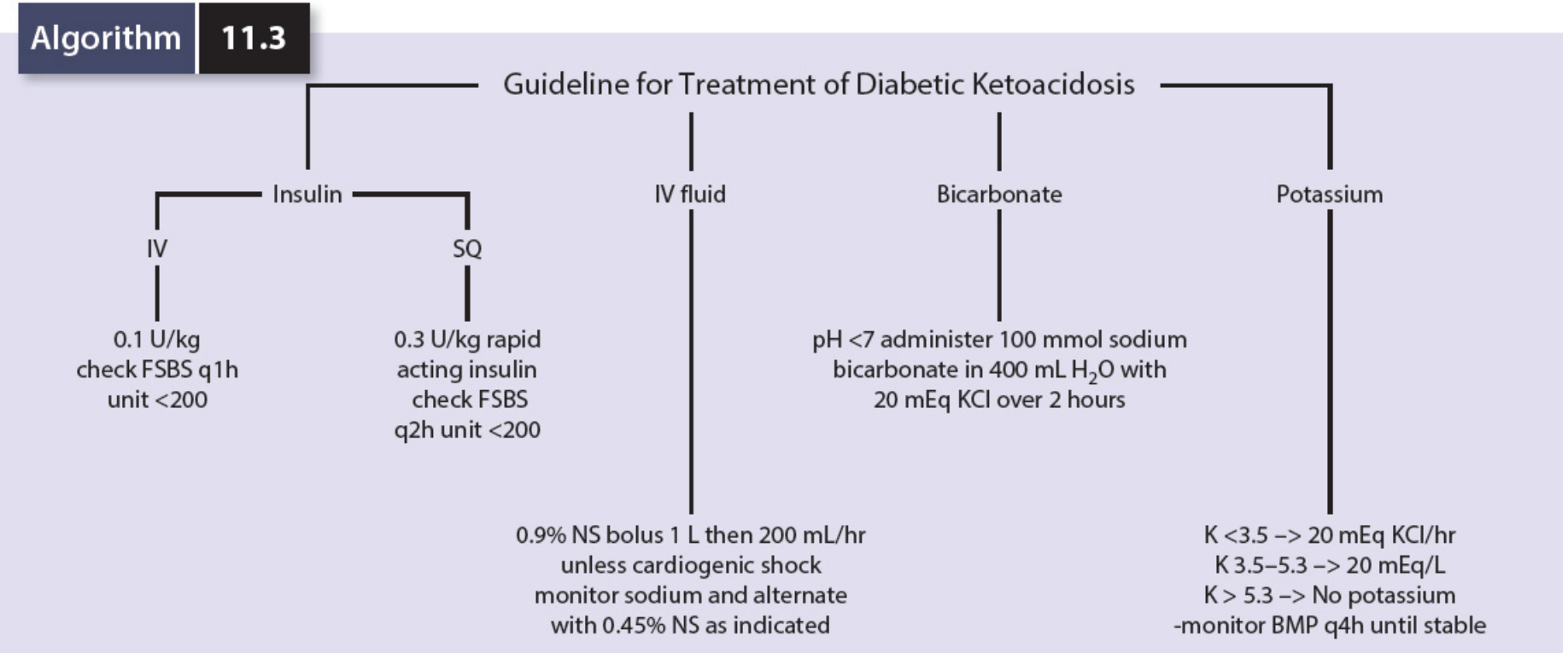
Four Pillars of Treatment
1. 🧪 Fluid Replacement (Most Urgent)
- Fluid losses of 5–10 liters are typical in DKA (Goldman-Cecil Medicine)
- Initial: 0.9% Normal Saline (NS) — 1 L bolus, then 2–4 liters over the first 2–4 hours
- 0.9% NS is used even if osmolality is high because it is relatively hypotonic to plasma
- Continue 0.9% NS at ~200 mL/hr, alternating with 0.45% NS as sodium normalizes
- Once glucose falls to <250 mg/dL: Add 10% dextrose alongside the NS to provide substrate for continued insulin infusion and prevent hypoglycemia while ketones clear
- Caution: Slow fluid replacement in patients with ischemic heart disease, heart failure, or renal impairment
2. 💉 Insulin
IV Route (preferred for moderate–severe DKA):
- Fixed-rate IV insulin infusion: 0.1 units/kg/hour
- Monitor blood glucose hourly (FSBS q1h)
- Once glucose <250 mg/dL AND ketones <1.0 mmol/L → reduce to 0.05 units/kg/hour to prevent hypoglycemia and hypokalemia
- Continue until patient can eat, then overlap with subcutaneous insulin by 1–2 hours before stopping IV infusion (to avoid rebound ketosis)
Subcutaneous Route (acceptable for mild DKA or if IV access unavailable):
- 0.3 units/kg rapid-acting insulin (e.g., lispro or aspart)
- Check FSBS every 2 hours; target <200 mg/dL
- Subcutaneous regimens are also effective per Goodman & Gilman
If the patient was already on background long-acting subcutaneous insulin, continue it alongside the IV infusion.
3. 🧂 Potassium Replacement
| Serum K⁺ | Action |
|---|---|
| >5.5 mEq/L | Hold potassium; monitor closely |
| 3.5–5.5 mEq/L | Add KCl 20–40 mEq/L to each liter of 0.9% NS as urine output confirmed |
| <3.5 mEq/L | Give KCl 20 mEq/hr IV; delay insulin until K⁺ ≥3.5 to avoid life-threatening hypokalemia |
Key point: Serum K⁺ is often elevated at presentation (due to acidosis shifting K⁺ extracellularly), but total body K⁺ is depleted. It drops rapidly once insulin is given — anticipate and replace.
4. 🫧 Bicarbonate
- Routinely NOT recommended — risk of paradoxically worsening CNS pH and cerebral edema
- Restoration of volume and insulin therapy usually corrects acidosis
- Only consider if: pH <7.0 AND not responding to fluids/insulin
- Give 100 mmol NaHCO₃ in 400 mL water with 20 mEq KCl over 2 hours
- Aim to raise pH above 7.1 only; do not attempt to normalize pH
Step 3 — Identify and Treat the Precipitant
Common triggers — address these in parallel:
- Infection (most common) — CBC, cultures, CXR, urinalysis
- Insulin omission or pump failure
- New-onset Type 1 DM
- Myocardial infarction, pancreatitis, medications (steroids, SGLT2 inhibitors)
The white blood cell count is typically elevated even without infection due to metabolic acidosis itself — do not diagnose infection on WBC alone.
Step 4 — Monitoring During Treatment
| Parameter | Frequency |
|---|---|
| Blood glucose | Every 1h (IV) or 2h (SQ) |
| Serum electrolytes (K⁺, Na⁺, HCO₃⁻) | Every 2–4 hours |
| Blood ketones (β-OHB) or urine ketones | Every 2–4 hours |
| Anion gap | Every 2–4 hours |
| Urine output | Continuous |
Note: Urine ketones may appear to worsen after insulin is started (as β-OHB converts to acetoacetate). Use blood ketones or anion gap as the primary marker of resolution, not urine ketones.
Resolution Criteria (DKA)
DKA is resolved when all three are met:
- Blood glucose <250 mg/dL
- Serum bicarbonate ≥15 mmol/L
- Venous pH >7.30
- Blood β-OHB <1.0 mmol/L (where available)
Phosphate & Magnesium
- Measure and monitor
- Routine IV replacement is not recommended unless phosphate <1.0 mg/dL with profound muscle weakness
Transition to Outpatient Therapy (after resolution)
- Resume usual diabetes regimen
- Sick-day rules education: frequent glucose monitoring, ketone testing when unwell, small frequent carbohydrate-containing fluids, adjust insulin rather than stop it
- Address compliance, device issues, or diabetes education gaps
Recent Evidence Update
Three recent meta-analyses (2024–2026) are relevant:
- Subcutaneous vs IV insulin (PMID 39090718): Subcutaneous insulin is comparable to continuous IV infusion in adult DKA management
- Balanced electrolyte solutions vs 0.9% NS (PMID 38925619): Balanced solutions (e.g., Lactated Ringer's, PlasmaLyte) result in faster DKA resolution than normal saline
- Early basal insulin with IV infusion (PMID 41208563): Giving subcutaneous basal insulin early alongside IV infusion reduces rebound ketosis after IV discontinuation
These findings suggest that subcutaneous protocols are a valid alternative for mild-moderate DKA, and balanced crystalloids may be preferred over 0.9% NS when available.
Sources: Goldman-Cecil Medicine International Edition (Table 210-12, Chapter 210); Comprehensive Clinical Nephrology 7th ed.; Goodman & Gilman's Pharmacological Basis of Therapeutics; Mulholland & Greenfield's Surgery 7e (Algorithm 11.3)
This is a shared conversation. Sign in to Orris to start your own chat.