Vitamin d
Reading File
Finding Sources
Searching PubMed
"vitamin D" supplementation
Reading File
Reading File
Loading Image
Reading File
Reading File
Here is a thorough overview of Vitamin D:
Vitamin D
What It Is
Vitamin D is a fat-soluble vitamin that functions more like a steroid hormone than a classic vitamin. It exists in two main dietary forms:
- Vitamin D3 (cholecalciferol) - from animal sources (fatty fish, fish oils, eggs, fortified milk) and made in the skin
- Vitamin D2 (ergocalciferol) - from plant sources (plants, yeasts) exclusively
Metabolism (How It Is Activated)
The activation process requires two sequential hydroxylation steps:
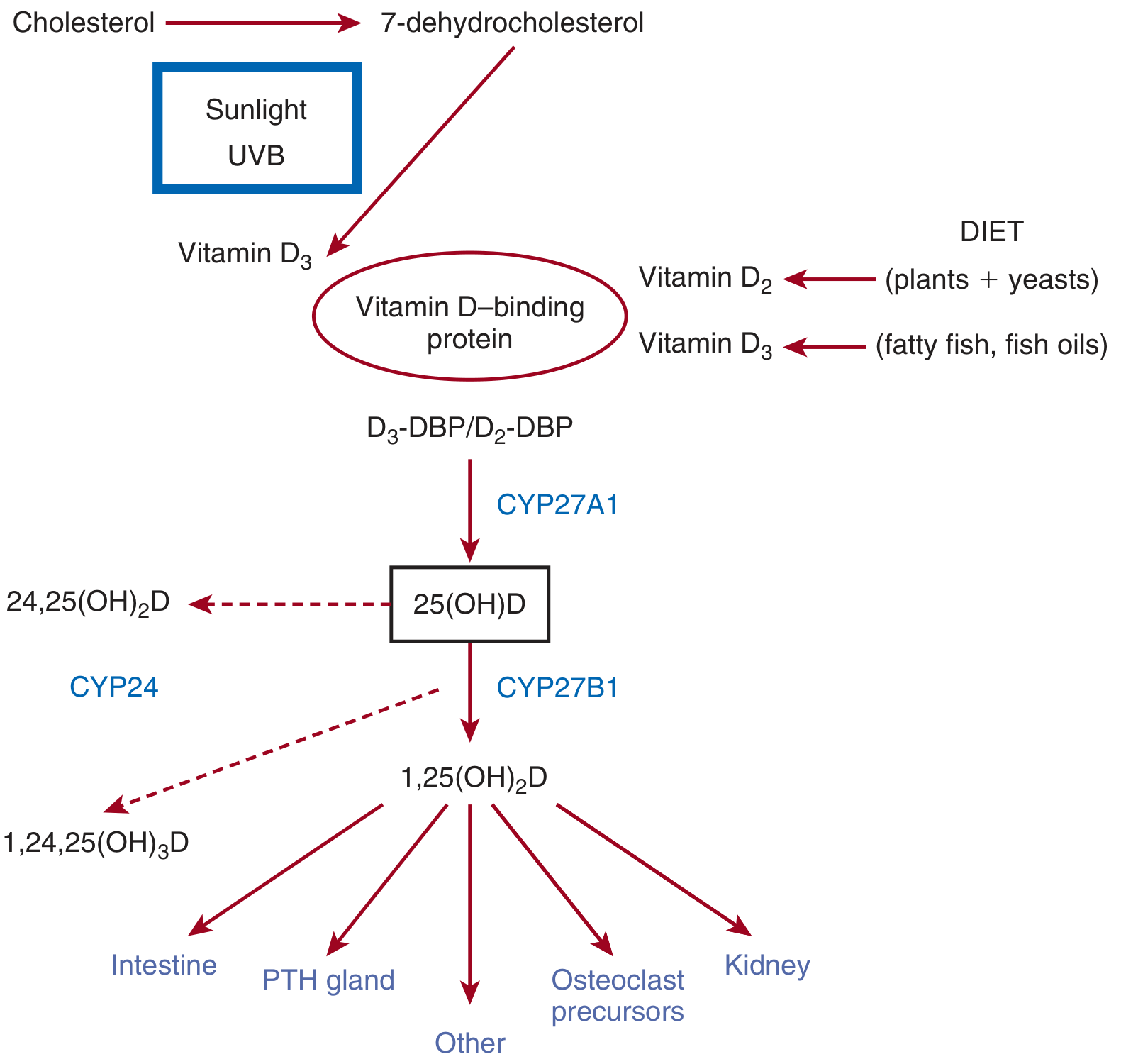
Step 1 - Skin synthesis:
Cholesterol → 7-dehydrocholesterol → Vitamin D3 (via UVB sunlight). This reaction requires UVB radiation and is reduced by:
- High skin melanin content
- Sunscreen with SPF 8 or higher
- Living at higher latitudes (less sunlight)
Step 2 - Liver hydroxylation:
D3 or D2 binds to vitamin D-binding protein (DBP) and is carried to the liver, where CYP27A1 (25-hydroxylase) converts it to 25(OH)D (calcidiol). This step is largely unregulated.
Step 3 - Kidney activation:
Calcidiol is converted by CYP27B1 (1-alpha-hydroxylase) in the proximal tubule of the kidney to 1,25(OH)2D (calcitriol) - the biologically active form. Calcitriol is ~1,000x more active than calcidiol.
Degradation: CYP24A1 (24,25-hydroxylase) and CYP3A4 in the kidney inactivate calcitriol.
- Medical Physiology, p. 1558-1560
- Brenner and Rector's The Kidney, p. 2394
Mechanism of Action
Calcitriol (1,25(OH)2D) is a steroid hormone. Inside target cells:
- It binds the Vitamin D Receptor (VDR) in the cytoplasm
- The VDR-ligand complex translocates to the nucleus
- It heterodimerizes with the Retinoid X Receptor (RXR)
- The complex binds vitamin D response elements (VDRE) on target genes
- Recruits coactivators/corepressors to modulate gene transcription
Physiological Actions
| Target | Effect |
|---|---|
| Intestine | Stimulates transcellular Ca2+ absorption (via TRPV6 channels and calbindin) and phosphate absorption (via NaPi cotransporter) |
| Kidney | Promotes Ca2+ and phosphate reabsorption from renal tubules |
| Bone | At normal levels: promotes mineralization (raises Ca x PO4 ion product). At excess: promotes bone mobilization/resorption |
| Parathyroid gland | Suppresses PTH secretion (negative feedback) |
| Immune system | Modulates innate and adaptive immunity |
The net result of normal vitamin D activity is a rise in both plasma calcium and phosphate, which drives bone mineralization.
Regulation
- PTH increases renal 1-alpha-hydroxylase → more calcitriol production
- Low phosphate also stimulates calcitriol synthesis
- Calcitriol itself provides negative feedback by suppressing PTH and 1-alpha-hydroxylase
- High calcium intake → suppresses PTH → less 1-hydroxylation → less calcitriol (reduces gut absorption over time)
Laboratory Testing
- 25(OH)D (calcidiol) is the standard serum test for vitamin D status (reflects body stores)
- Reference ranges commonly used:
- Deficient: < 20 ng/mL
- Insufficient: 20-29 ng/mL
- Sufficient: ≥ 30 ng/mL
Deficiency
Causes:
- Inadequate sun exposure (elderly, institutionalized, dark skin, high latitudes)
- Poor dietary intake
- Fat malabsorption (Crohn's, celiac, pancreatic insufficiency) - vitamin D is fat-soluble and needs bile salts
- Chronic kidney disease (impaired 1-hydroxylation)
- Liver disease (impaired 25-hydroxylation)
Effects in children: Rickets - unmineralized osteoid, bowed legs, abnormal bone rigidity
Effects in adults: Osteomalacia - increased unmineralized osteoid, bone pain, stress fractures, hypocalcemia
Consequences of chronic mild deficiency:
-
Secondary hyperparathyroidism (elevated PTH compensating for low Ca2+)
-
Worsening osteoporosis from persistent PTH-driven bone resorption
-
Hypocalcemia → nerve hypersensitivity → numbness, tingling, tetany
-
Medical Physiology, p. 1560
Toxicity (Excess)
Vitamin D toxicity causes hypercalcemia (excess bone mobilization + intestinal absorption). Symptoms include nausea, weakness, polyuria, nephrocalcinosis, and soft tissue calcification. This cannot occur from sun exposure alone (skin synthesis is self-limiting), only from excessive supplementation.
Recent Evidence (2024-2026)
A 2024 meta-analysis (PMID 39421966) found that vitamin D supplementation significantly reduces asthma exacerbations in children. Research on vitamin D's role in hair loss (androgenetic alopecia) and dermatological conditions continues to be investigated, though evidence remains mixed.
Sources: Medical Physiology (Boron & Boulpaep), Brenner and Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.