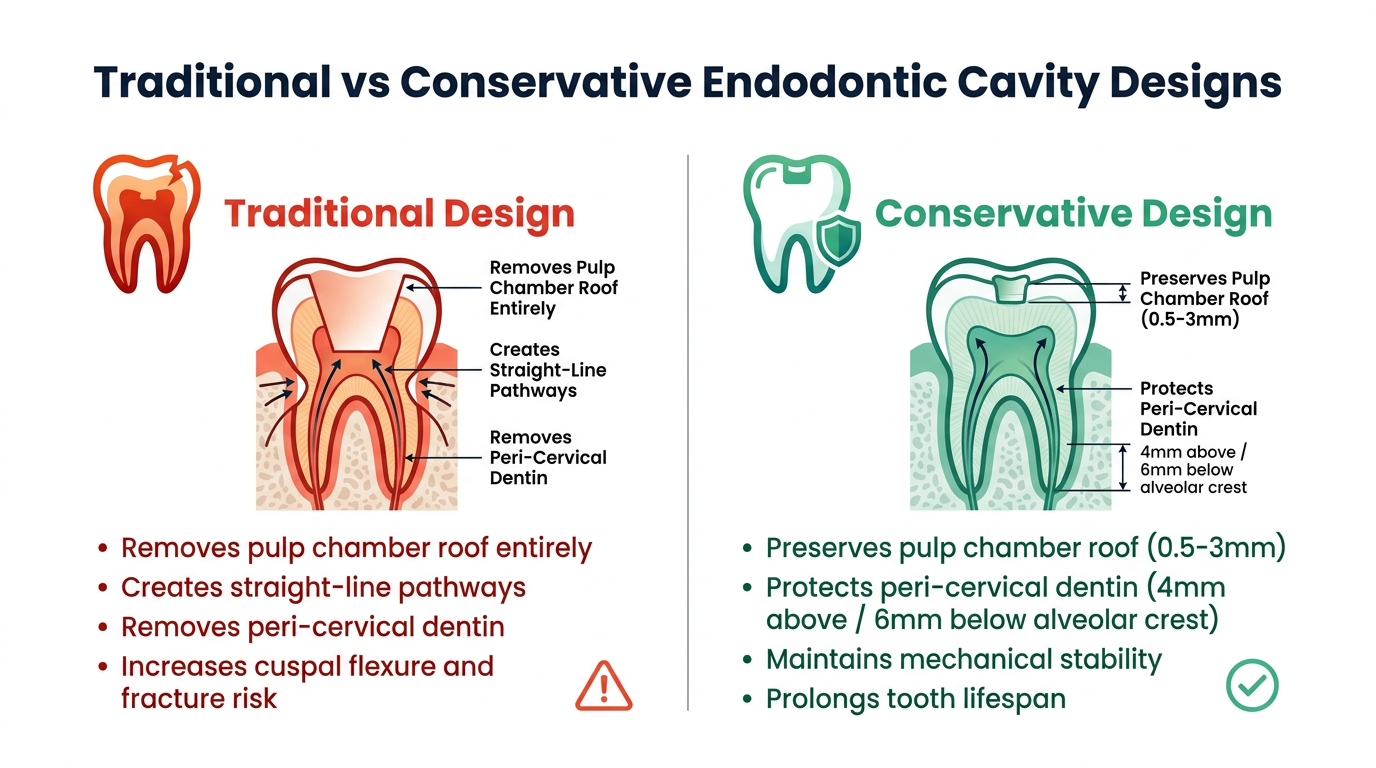
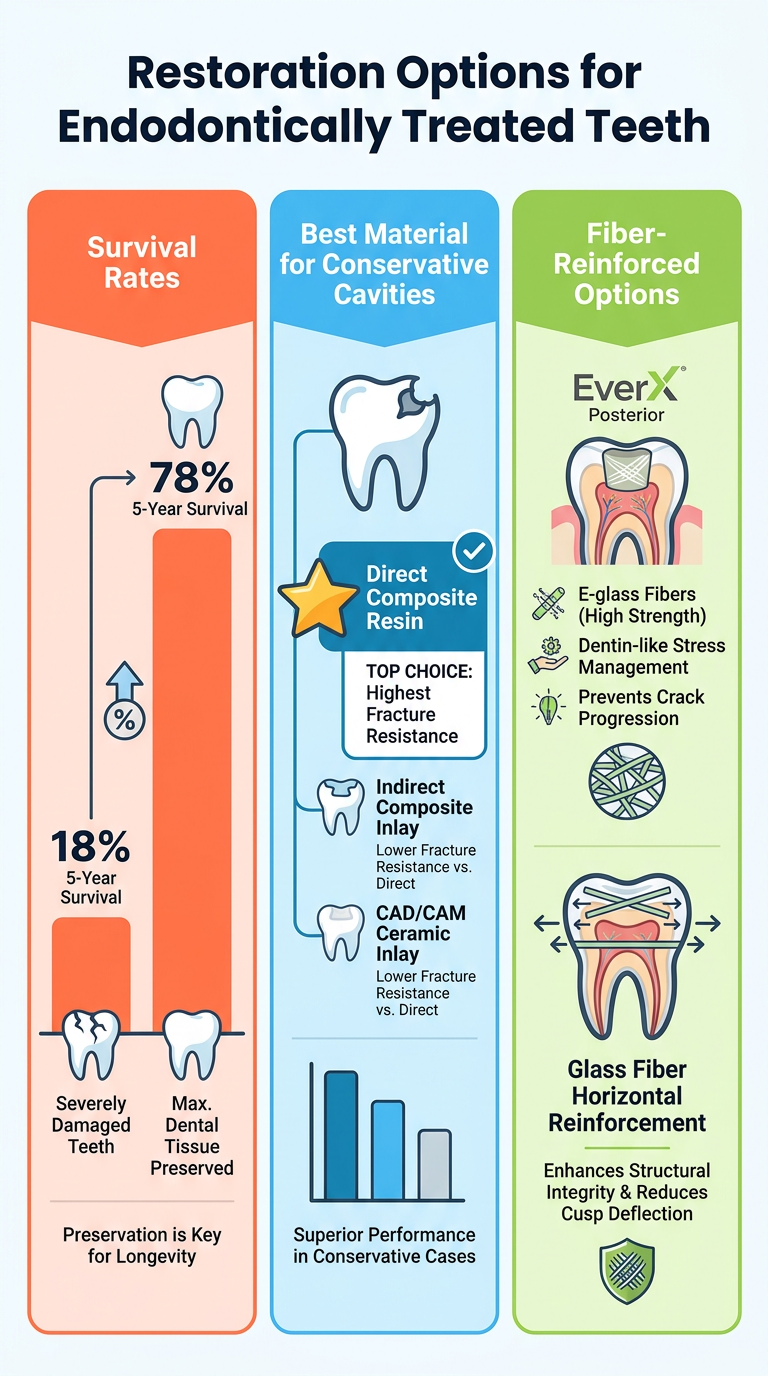
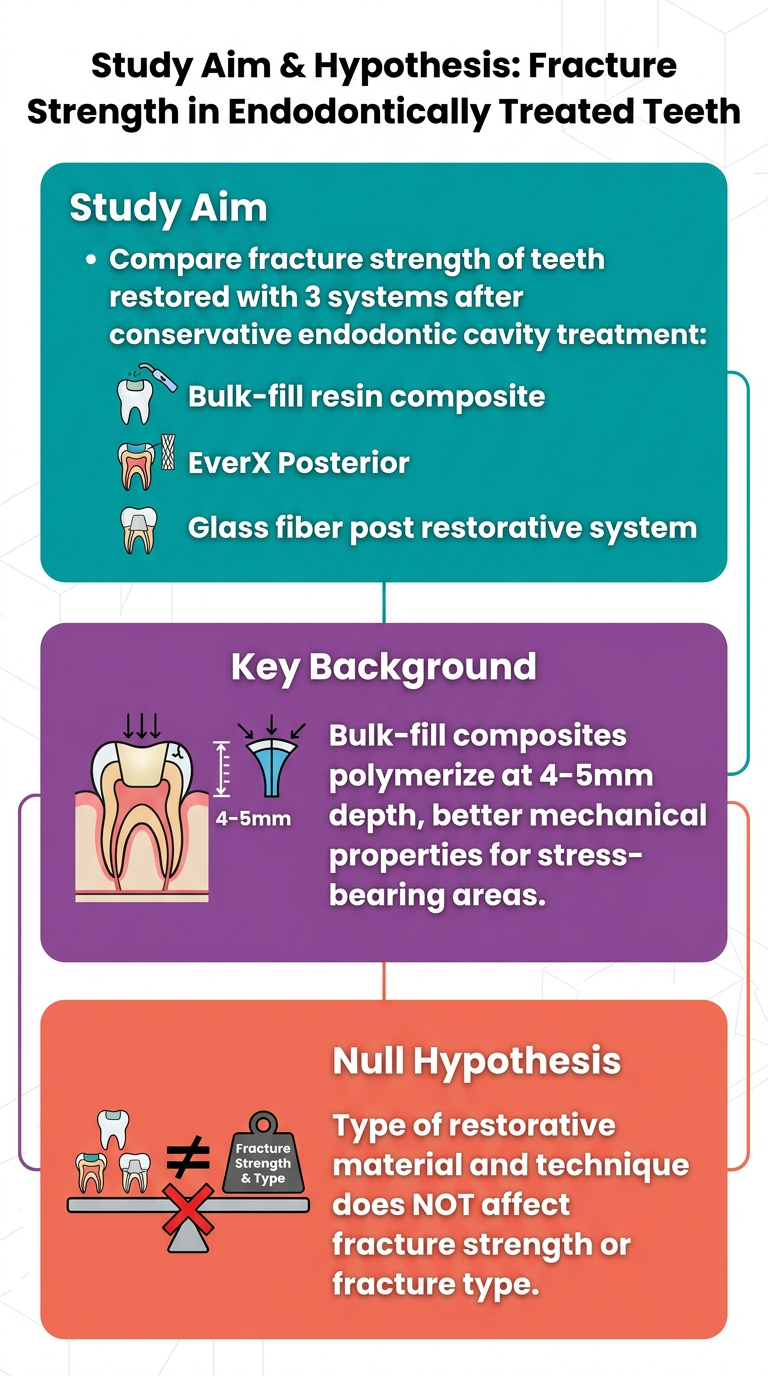
convert this into sepearte images for my presentation: The long-term success of endodontic treatment is affected by an endodontic access cavity design that preserves the tooth structure as much as possible, the quality of root canal treatment procedures, the type of ideal restoration to com pensate for the loss of coronal tooth structure and the appli cation technique [1, 2]. For decades, traditional endodontic cavity designs, whose outlines are standardized for each tooth type, have remained virtually unchanged, completely removing the pulp chamber roof to detect root canals and creating straight-line pathways into the canals to increase the effectiveness of instrumentation [3–5]. However, such peri-cervical dentin [3]. Positioned roughly 4 mm above and 6 mm below the alveolar bone crest, the peri-cervical dentin is recognized as a vital component for the overall longevity and proper functioning of the tooth [6], playing a critical role in distributing forces from the occlusal aspect to the root(s) [7]. Increasing cuspal flexure by removing peri cervical dentin during traditional endodontic cavity prepa ration increases the stress on the crown and root surfaces of teeth, which may increase the possibility of fracture in endodontically treated teeth when subjected to functional loads [8–10]. Clark et al. [11] suggested that preserving a 0.5–3 mm pulp chamber roof is the most secure approach to avoid causing harm to this dentin. Therefore, with advancements in magnification and imaging techniques as well as endodontic instruments, con servative endodontic cavity designs, which aim to protect the remaining tooth tissue during access cavity prepara tion, have been developed as an alternative to traditional endodontic cavity designs [12]. In conservative endodontic cavity designs, the removal of restorative materials instead of enamel or dentin and the removal of occlusal structures instead of peri-cervical dentin are preferred. This approach preserves parts of the pulp chamber’s roof while safe guarding the peri-cervical dentin, which helps maintain the mechanical stability of the tooth, ultimately prolonging its lifespan and enhancing its functionality [6, 7, 13]. However, conservative cavity designs may limit proper irrigation and instrumentation, obturate root canals, and lead to more errors during endodontic procedures [14]. Several studies have proposed new, more conservative and ultraconservative approaches for preparing endodontic access cavities, such as the conservative, Ninja and truss access designs [12, 15]. The Ninja endodontic access cav ity design consists of opening a small hole from the central fossa or the deepest part of the occlusal surface, allowing the clinician to locate and access all canal orifices [15]. The truss endodontic access cavity design uses direct access from the occlusal surface to each canal orifice and main tains a dentin bridge between the canal orifices [16]. In addi tion, some new conservative approaches for access cavity preparations have also been introduced, as sometimes the tooth already has restorations or has some caries patterns in which traditional or conservative access cavity preparation cannot be achieved (For example, as in this study, the mesial canals are accessed from the mesio occlusal cavity, which is opened due to caries or old restoration in the mandibu lar first molar tooth. For the distal canal, a truss endodontic access cavity design is used to provide direct access from the occlusal surface) [17, 18]. A recent study showed that a truss endodontic access cavity could increase the frac ture strength of endodontically treated teeth compared with other conservative endodontic cavity designs and traditional endodontic access cavity design [4]. In the literature, there are treatment options for the res toration of endodontically treated teeth, such as post-core and total or partial crowns, and advancements in adhesive technologies provide the opportunity to create conservative and aesthetically pleasing dental restorations entirely with composite resin materials [19, 20]. A retrospective study reported that the 5-year survival rate of severely damaged endodontically treated molars restored directly with com posite resin was 18%, while the cumulative survival rate increased to 78% when the maximum amount of dental tis sue was present [21]. For endodontically treated posterior teeth exhibiting conservative endodontic cavity designs, the most suitable access restoration consists of a direct restora tion using a resin composite due to its high bond strength to the dental substrate [22]. The comparison of fracture resistance of endodontically treated upper premolar teeth after restoration of the two-walled access cavity preparation using direct composite, indirect composite and computer aided design/computer aided manufacturing CAD/CAM ceramic inlays showed that composite resins have the high est fracture resistance [23]. To strengthen direct composite resin restorations, glass fiber can be added horizontally to the coronal structure, or fiber-reinforced resin composites can be used to increase the fracture resistance of the core structure due to their suit able physical properties [24, 25]. Using glass fibers in the restoration of access cavity restoration enhances the flex ural properties of composite resin, providing effective force transmission and high fracture resistance [26]. EverX Poste rior has been introduced to the market as a dentine replace ment material, featuring E-glass fibers in its composition [27]. The manufacturer claims that using EverX Posterior (GC, Tokyo, Japan) in stress-bearing areas enables the resto ration to exhibit dentin-like stress management, preventing the progression of formed cracks [28]. High-tech production of this special component composite has allowed us to pro vide the high fracture resistance of composite restorations, even in large posterior cavities [29]. The introduction of bulk-fill resin composites has recently gained attention due to their translucency, allowing for an induced degree of conversion rates and the ability to polymerize effectively at a thickness of 4–5 mm [30]. An increased degree of conversion allows the material to have better mechanical properties and enables its use in stress bearing areas, especially in post endodontic restorations [31]. Information on the effects of minimally invasive access cavity design, optimal restoration techniques and the use of optimal material is limited. Hence, the present study aimed to compare the fracture strength of teeth restored with a bulk-fill resin composite, EverX Posterior and a glass fiber post restorative system after endodontic treatment, utilizing a conservative endodontic cavity design. The null hypothesis of this study was that the type of restorative material and technique used would not affect the fracture strength or fracture type of endodontically treated teeth with a conservative endodontic cavity design.
Colorful infographic portrait slide titled "Factors Affecting Endodontic Treatment Success". Content includes 4 key factors listed with icons: 1) Access cavity design that preserves tooth structure, 2) Quality of root canal treatment procedures, 3) Type of ideal restoration to compensate for lost coronal tooth structure, 4) Application technique. Include a small dental tooth diagram in the center. Bright modern colors (teal, coral, purple, yellow), bold headings, clean layout, white background with colored accent blocks.
Colorful infographic portrait slide titled "Traditional vs Conservative Endodontic Cavity Designs". Two-column comparison layout. Left column "Traditional Design" (red/orange tones): removes pulp chamber roof entirely, creates straight-line pathways, removes peri-cervical dentin, increases cuspal flexure and fracture risk. Right column "Conservative Design" (green/teal tones): preserves pulp chamber roof (0.5-3mm), protects peri-cervical dentin (4mm above / 6mm below alveolar crest), maintains mechanical stability, prolongs tooth lifespan. Include small tooth cross-section diagrams in each column. Bold icons, modern fonts, white background.
Colorful infographic portrait slide titled "Types of Conservative Endodontic Access Cavity Designs". Three distinct sections with bright color blocks (blue, purple, orange): 1) "Conservative Design" - removes restorative materials instead of enamel/dentin, preserves peri-cervical dentin; 2) "Ninja Design" - small hole from central fossa/deepest occlusal surface, locates all canal orifices; 3) "Truss Design" - direct access from occlusal surface to each canal orifice, maintains dentin bridge between canals, increases fracture strength. Include simple top-down tooth diagrams showing each approach. Modern colorful infographic style, portrait orientation.
Colorful infographic portrait slide titled "Restoration Options for Endodontically Treated Teeth". Three sections with bright colors (coral, blue, green): 1) "Survival Rates" - bar chart showing 18% 5-year survival with severely damaged teeth vs 78% with maximum dental tissue preserved; 2) "Best Material for Conservative Cavities" - Direct composite resin highlighted as top choice: highest fracture resistance vs indirect composite and CAD/CAM ceramic inlays; 3) "Fiber-Reinforced Options" - EverX Posterior (E-glass fibers, dentin-like stress management, prevents crack progression), glass fiber horizontal reinforcement. Bold stats, icons, modern fonts, white background, portrait orientation.
Colorful infographic portrait slide titled "Study Aim & Hypothesis: Fracture Strength in Endodontically Treated Teeth". Clean modern layout. Top section "Study Aim" (teal): Compare fracture strength of teeth restored with 3 systems after conservative endodontic cavity treatment - Bulk-fill resin composite, EverX Posterior, Glass fiber post restorative system. Middle section "Key Background" (purple): Bulk-fill composites polymerize at 4-5mm depth, better mechanical properties for stress-bearing areas. Bottom section "Null Hypothesis" (coral/orange): Type of restorative material and technique does NOT affect fracture strength or fracture type. Include small icons for each material type. Bold text, colorful blocks, portrait format.

- What determines endodontic success (the 4 key factors)
- Traditional vs conservative design comparison (with the peri-cervical dentin concept)
- Ninja, Truss, and conservative cavity designs explained
- Restoration materials - survival rates, composite resin, fiber-reinforced options
- Study aim and null hypothesis for the research being presented