Folate trap
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the information needed for a comprehensive answer.
The Folate Trap (Methyl-Trap Hypothesis)
Core Concept
The folate trap (also called the methyl-trap hypothesis) describes how vitamin B12 deficiency produces a functional folate deficiency even when total body folate is normal. The folate pool becomes "trapped" in a metabolically useless form.
The Biochemical Mechanism
Normal state
Dietary folates enter cells and are converted to tetrahydrofolate (THF), the active form that carries one-carbon units for DNA synthesis (purines and thymidylate) and amino acid metabolism.
The folate cycle has a critical junction:
- Methylene-THF is irreversibly reduced by methylenetetrahydrofolate reductase (MTHFR) to N5-methyl-THF (5-methyltetrahydrofolate, or methyl-THF)
- This is the most thermodynamically stable form of folate in the cell
- The only reaction that can remove the methyl group from methyl-THF and release free THF is the methionine synthase reaction
The methionine synthase reaction (the exit door)
Methionine synthase uses methyl-THF as the methyl donor to convert homocysteine → methionine, with vitamin B12 (methylcobalamin) as the essential cofactor:
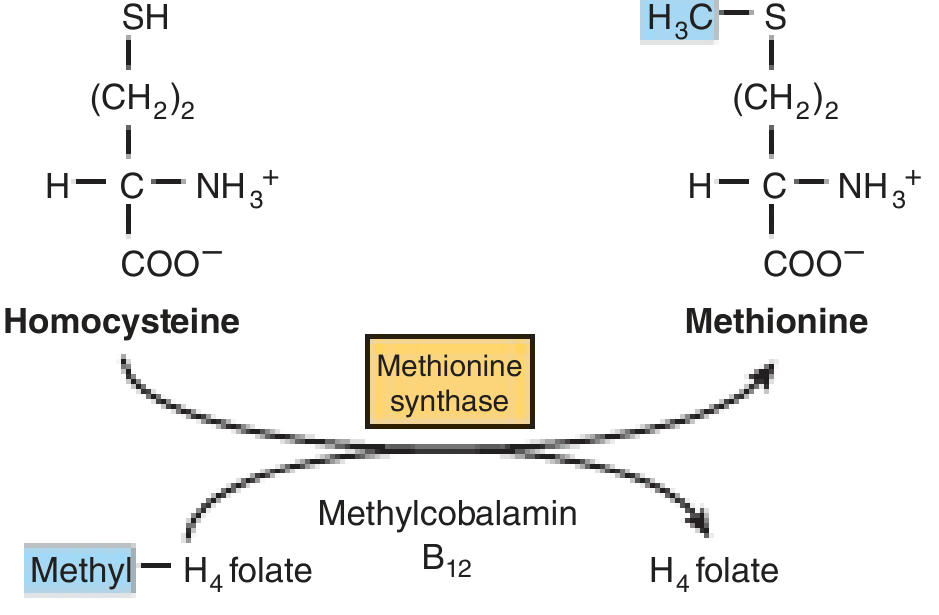
Fig: Methionine synthase converts homocysteine to methionine, transferring the methyl group from methyl-THF to release free THF. This requires vitamin B12 (methylcobalamin) as cofactor.
When B12 is deficient
- Methionine synthase activity is impaired (no B12 cofactor)
- Methyl-THF cannot donate its methyl group - it accumulates
- Over time, nearly the entire folate pool is sequestered as methyl-THF
- Free THF (and its other active derivatives - methylene-THF, formyl-THF, etc.) become unavailable
- Result: functional folate deficiency - folate is present in serum but cannot be used
This is the "trap": folate is locked in the methyl-THF form, which is a one-way street with a blocked exit.
Consequences of the Folate Trap
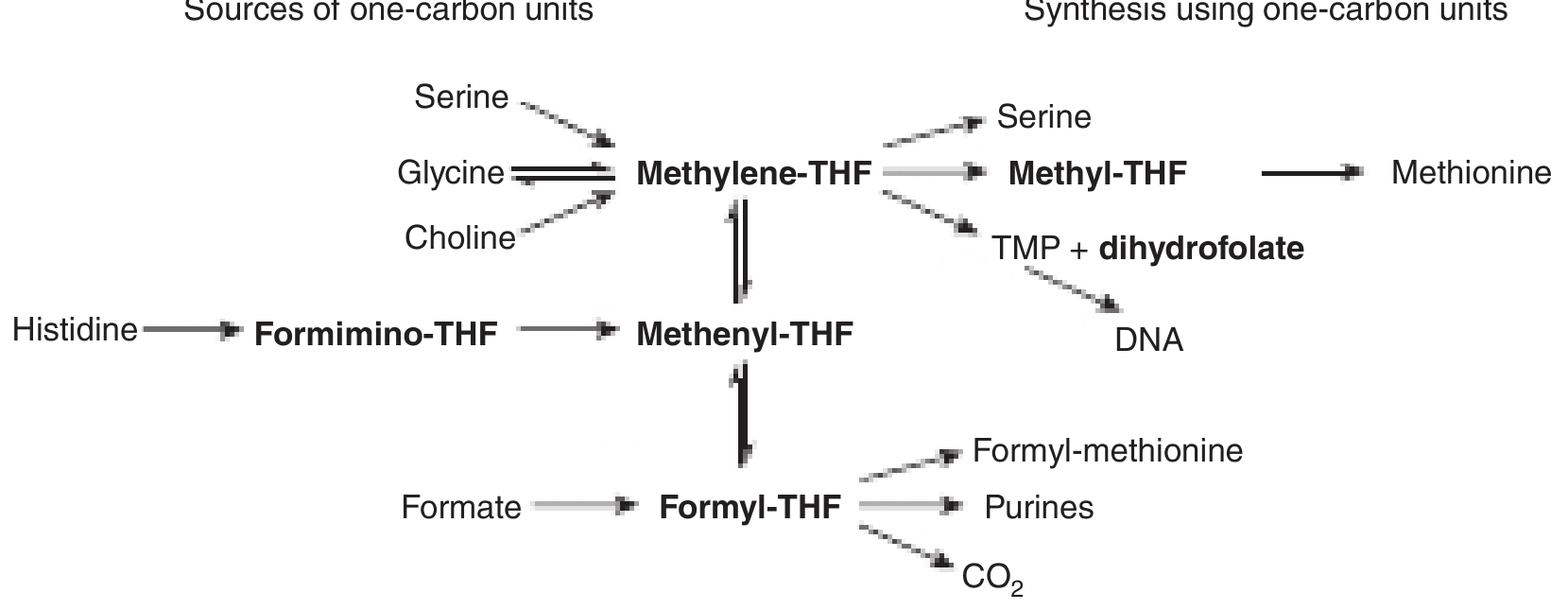
Fig: Sources and utilization of one-carbon substituted folates. In the folate trap, the entire pool is stuck as Methyl-THF and cannot feed into TMP synthesis or purine synthesis.
1. Megaloblastic anemia
- Methylene-THF is needed by thymidylate synthase to convert dUMP → dTMP (for DNA synthesis)
- Formyl-THF is needed for purine synthesis
- With the trap engaged, both pathways fail → impaired DNA synthesis → large, poorly dividing RBC precursors → megaloblastic anemia
- This is the same presentation as primary folate deficiency - the two are clinically indistinguishable on peripheral smear
2. Hyperhomocysteinemia
- The methionine synthase reaction is blocked → homocysteine accumulates
- Elevated homocysteine is a cardiovascular and neurological risk factor
3. SAM depletion (neurological effects)
- Methionine → S-adenosylmethionine (SAM) is the universal methyl donor in the CNS
- B12 deficiency → less methionine regenerated → reduced SAM → hypomethylation of DNA, histones, and myelin proteins
- The nervous system lacks the alternative betaine pathway for methionine regeneration, making it especially vulnerable
- Combined with methylmalonyl-CoA accumulation and branched-chain fatty acid incorporation into myelin → subacute combined degeneration of the spinal cord
The Dangerous Clinical Trap: Giving Folate Alone to a B12-Deficient Patient
This is the most important clinical implication of the folate trap:
| Action | Effect |
|---|---|
| Give folate alone to a B12-deficient patient | Partially corrects megaloblastic anemia (bypasses the trap by providing extra THF for dTMP/purine synthesis), but does NOT fix B12 deficiency |
| Neurological disease continues to progress silently while the anemia improves | Subacute combined degeneration can become irreversible |
| Why this happens | Extra folate bypasses the blocked step; the underlying B12 deficiency and SAM/methylmalonate pathway problems remain |
"If folate is given without cobalamin to a B12-deficient patient, the drug only partially corrects the megaloblastic anemia... However, the neurological syndrome may progress unless the physician realizes that B12 supplementation is required." - Basic Medical Biochemistry, 6e
This is why it is mandatory to rule out B12 deficiency before treating megaloblastic anemia with folate.
Key Enzymes and Cofactors
| Enzyme | Cofactor | Reaction | What fails in B12 deficiency |
|---|---|---|---|
| MTHFR (methylenetetrahydrofolate reductase) | NADPH | Methylene-THF → Methyl-THF (IRREVERSIBLE) | Works normally - continues trapping folate |
| Methionine synthase | Vitamin B12 (methylcobalamin) | Methyl-THF + Homocysteine → THF + Methionine | BLOCKED - this is the trap |
| Thymidylate synthase | Methylene-THF | dUMP → dTMP | Starved of substrate |
| Methylmalonyl-CoA mutase | Adenosylcobalamin (B12) | Methylmalonyl-CoA → Succinyl-CoA | Also fails - separate B12 pathway |
Summary
The folate trap = B12 deficiency → methionine synthase failure → methyl-THF accumulates → active THF pools depleted → functional folate deficiency → megaloblastic anemia + homocysteinemia
The neurological damage (subacute combined degeneration) is a separate B12-dependent mechanism (SAM depletion + methylmalonate accumulation) that giving folate alone will not address.
Sources: Harper's Illustrated Biochemistry 32e, p.556-557 | Basic Medical Biochemistry: A Clinical Approach 6e, pp.1393-1398 | Katzung's Basic and Clinical Pharmacology 16e | Quick Compendium of Clinical Pathology 5e
This is a shared conversation. Sign in to Orris to start your own chat.