Write notes for ten marks each for acute angle-closure glaucoma and acute open-angle glaucoma ophthalmology for final year MBBS university exam which should include definition, etiology, pathogenesis, clinical features, investigations, management and complications of each separately for ten marks each with suitable draw able diagrams. Especially visual field changes
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have all the key content and images. Now I'll write the comprehensive notes.
ACUTE ANGLE-CLOSURE GLAUCOMA (AACG)
10-Mark University Examination Notes
1. DEFINITION
Acute angle-closure glaucoma (also called Acute Primary Angle Closure - APAC, or acute congestive glaucoma) is a sudden, dramatic rise in intraocular pressure (IOP) caused by mechanical obstruction of the trabecular meshwork by the peripheral iris, blocking aqueous outflow. It constitutes an ophthalmic emergency. IOP typically rises to 50-80 mmHg.
2. ETIOLOGY
Predisposing anatomical factors:
- Hypermetropic (short, small) eye with shallow anterior chamber
- Short axial length (nanophthalmos - axial length <20 mm carries highest risk)
- Thick, anteriorly placed crystalline lens
- Narrow drainage angle (iridocorneal angle)
- Shallow anterior chamber depth
- Large lens-to-eye volume ratio
Precipitating factors:
- Pharmacological mydriasis (atropine, tropicamide, sympathomimetics)
- Watching TV/reading in a darkened room
- Emotional stress, prolonged semi-prone position
- Systemic medications: anticholinergics, antihistamines, cold/flu remedies, topiramate and sulfa derivatives (cause ciliary body effusion), motion-sickness patches
Risk factors:
- Age: average onset ~62 years
- Female sex (more commonly affected)
- Asian/East Asian and Indian race (highest global burden)
- Family history of angle closure
- Hypermetropia >1 dioptre
3. PATHOGENESIS
Diagram: Mechanism of Pupillary Block
NORMAL EYE ACUTE ANGLE CLOSURE
Cornea Cornea (oedematous)
| |
Open angle Closed angle
/ \ / \
Iris Trabeculum Iris bowed Blocked
| | forward trabeculum
| Aqueous |
Lens flows freely Iris-lens contact
(pupillary block)
↑ IOP
Step-by-step mechanism (pupillary block - most common):
-
Relative pupillary block: At mid-dilation (~4 mm), the iris is in maximal contact with the anterior lens surface, creating resistance to aqueous flow from the posterior chamber through the pupil to the anterior chamber.
-
Posterior chamber pressure rise: Aqueous accumulates behind the iris, raising posterior chamber pressure above anterior chamber pressure.
-
Iris bombe: The pressure difference pushes the peripheral iris anteriorly (iris bombe configuration), causing the iris to bow forward like a sail.
-
Iridotrabecular contact (ITC): The bowed peripheral iris makes contact with and occludes the trabecular meshwork, the primary outflow pathway for aqueous.
-
IOP spike: With outflow blocked, aqueous accumulates and IOP rises acutely to 50-80 mmHg.
-
Ischaemic damage: Extreme IOP causes ischaemia to the iris sphincter, corneal endothelium, and optic nerve head - all within hours.
Diagram: Aqueous Flow in Normal vs. Angle Closure
NORMAL ANGLE CLOSURE
┌──────────────────────┐ ┌────────────────────────────┐
│ Ciliary processes │ │ Ciliary processes │
│ ↓ │ │ ↓ │
│ Posterior chamber │ │ Posterior chamber │
│ ↓ (pupil) │ │ ↑ pressure (blocked) │
│ Anterior chamber │ │ IRIS BOMBE ←──────────── │
│ ↓ │ │ Peripheral iris blocks │
│ Trabecular meshwork│ │ trabeculum │
│ ↓ │ │ ✗ │
│ Schlemm's canal │ │ IOP ↑↑ (50-80 mmHg) │
└──────────────────────┘ └────────────────────────────┘
4. CLINICAL FEATURES
Symptoms
- Sudden severe unilateral eye pain (may radiate to forehead, temple, jaw)
- Dramatic decrease in vision (VA typically 6/60 to hand movements)
- Coloured haloes around lights - from corneal epithelial oedema
- Nausea and vomiting (can dominate, causing misdiagnosis as acute abdomen)
- Headache, photophobia
Signs (Classic Triad: Red eye + Hazy cornea + Mid-dilated pupil)
| Sign | Description |
|---|---|
| IOP | Markedly elevated: 50-80 mmHg (normal: 10-21 mmHg) |
| Pupil | Mid-dilated (4-6 mm), vertically oval, non-reactive to light |
| Cornea | Steamy/hazy due to epithelial oedema |
| Anterior chamber | Shallow, with aqueous flare |
| Conjunctiva | Intense redness - violaceous circumcorneal (ciliary) injection |
| Iris | Congested; later shows spiral atrophy |
| Fellow eye | Shallow AC, occludable narrow angle |
Clinical photograph from Kanski's - Acute primary angle closure:
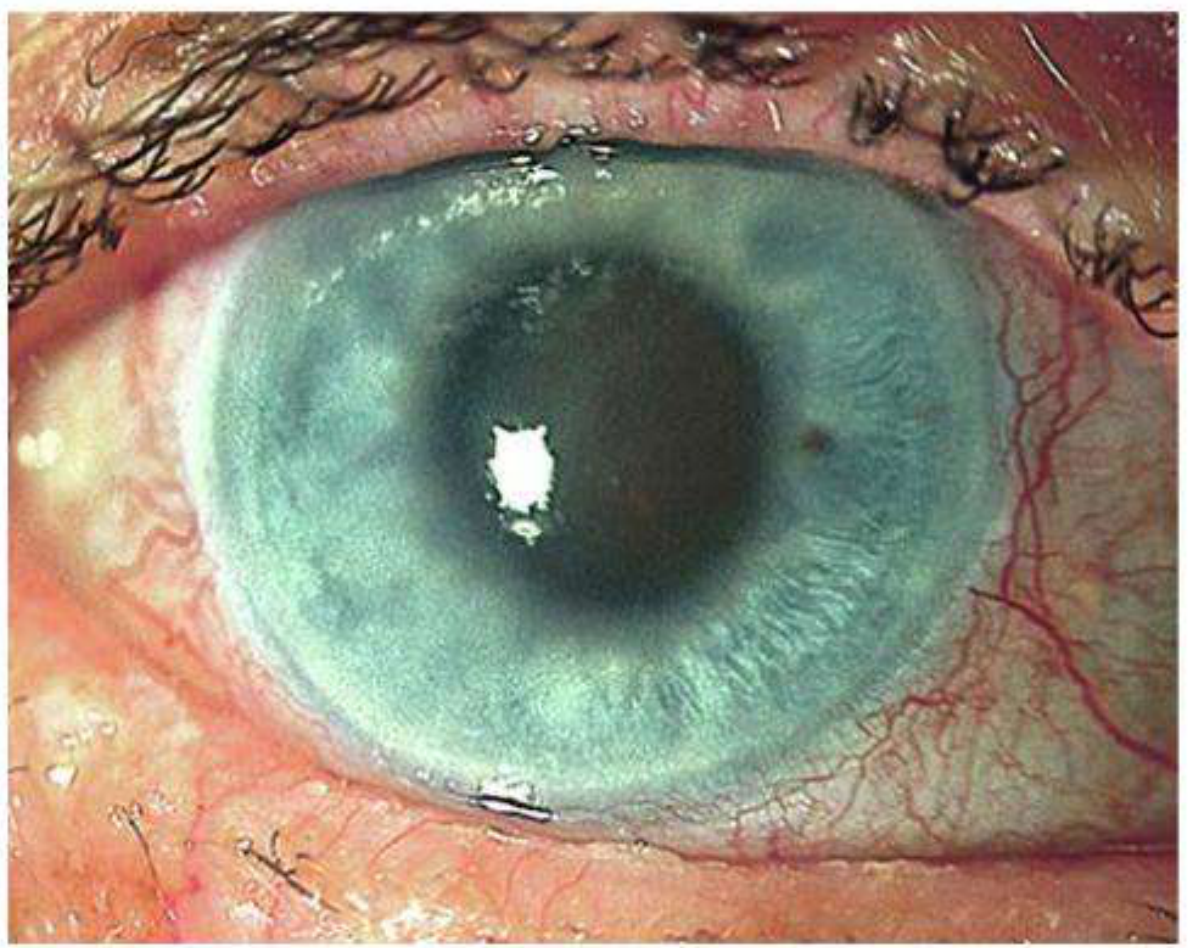
Note the mid-dilated vertically oval pupil, steamy cornea, and ciliary injection - classic signs of AACG (Kanski's Clinical Ophthalmology, 10th ed.)
Late/Resolved Signs
- Glaukomflecken: white foci of anterior lens capsule/cortex necrosis (pathognomonic of past attack)
- Iris atrophy with spiral-like configuration
- Irregular pupil, posterior synechiae
- Optic disc pallor + cupping (glaucomatous atrophy)
5. INVESTIGATIONS
- Tonometry (Goldmann applanation) - confirms high IOP (50-80 mmHg)
- Gonioscopy - shows closed angle (Grade 0-1 Shaffer); iridotrabecular contact; peripheral anterior synechiae (PAS); performed after attack subsides
- Slit lamp examination - corneal oedema, shallow AC, flare, iris changes, glaukomflecken
- Visual acuity - markedly reduced
- Anterior segment OCT (AS-OCT) - images anterior chamber depth, iris profile, angle anatomy without contact
- Ultrasound biomicroscopy (UBM) - shows plateau iris configuration, ciliary body position, narrow angle
- Fundoscopy - optic disc congestion/oedema acutely; later pallor and cupping
- Visual field testing - generalized depression acutely; if chronic component: inferior altitudinal loss, arcuate defects
- B-scan ultrasonography - in atypical cases to exclude secondary causes
- Biometry - if lens extraction is considered as definitive treatment
6. MANAGEMENT
Emergency/Immediate (Break the Attack)
Step 1 - Lower IOP medically:
| Drug | Route | Dose | Mechanism |
|---|---|---|---|
| Acetazolamide | IV if IOP >50 mmHg; oral if <50 mmHg | 500 mg | Carbonic anhydrase inhibitor - reduces aqueous production |
| Timolol 0.5% | Topical | 1 drop | Beta-blocker - reduces aqueous production |
| Apraclonidine 0.5-1% | Topical | 1 drop | Alpha-2 agonist - reduces aqueous production + increases uveoscleral outflow |
| Pilocarpine 2% | Topical (affected eye) | 1 drop × 2 (30 min apart) | Miotic - opens angle by pulling iris away from trabeculum; not repeated if IOP >40 mmHg (ischaemic iris is unresponsive) |
| Prednisolone 1% | Topical | 1 drop | Anti-inflammatory |
| Analgesia + antiemetic | Systemic | As needed | Symptomatic relief |
Step 2 - Resistant/Refractory cases:
- IV Mannitol 20% at 1-2 g/kg over 1 hour (hyperosmotic agent)
- Oral glycerol 50% (1 g/kg) or isosorbide
- Central corneal indentation (squint hook) to mechanically force aqueous into angle
- Topical 50% glycerol to clear corneal oedema for better visualization
- Early laser iridotomy/iridoplasty once oedema clears
Definitive Treatment
1. Laser Peripheral Iridotomy (LPI) - Treatment of choice
- Performed bilaterally (fellow eye has occludable angle)
- Creates a full-thickness hole in peripheral iris
- Allows aqueous to bypass pupillary block directly from posterior to anterior chamber
- Performed once the attack is broken (clear cornea, preferably normal IOP)
- Nd:YAG laser or argon laser
2. Subsequent medical treatment:
- Pilocarpine 2% four times daily (affected eye) + 1% four times daily (fellow eye)
- Topical steroid four times daily if acutely inflamed
- Timolol 0.5% twice daily, apraclonidine 1% three times daily, acetazolamide 250 mg four times daily as needed
3. Surgical options (if medical/laser fails):
- Peripheral iridectomy (surgical iridotomy)
- Lens extraction (clear lens extraction) - definitive, also deepens AC
- Goniosynechialysis - break down PAS
- Trabeculectomy - if significant angle damage with residual high IOP
- Cyclodiode laser (ciliary body ablation) in refractory cases
Diagram: Laser Peripheral Iridotomy
BEFORE LPI AFTER LPI
Iris bombe Flat iris
(bowed forward) (decompressed)
↑
Aqueous trapped Aqueous bypasses pupil
behind iris through iridotomy hole
↓
Angle closed ✗ Angle opens ✓
IOP ↑↑ IOP normalizes
7. VISUAL FIELD CHANGES IN AACG
- During acute attack: generalized constriction of visual field due to corneal oedema and extreme IOP elevation
- After resolution: if optic nerve damage has occurred - inferior altitudinal defect (most common), arcuate scotoma, or generalized depression
- Severe/prolonged attack: can result in profound visual loss with only a small central island remaining or complete blindness
8. COMPLICATIONS
| Complication | Description |
|---|---|
| Permanent visual loss | From optic nerve ischaemia during prolonged IOP elevation |
| Glaukomflecken | Anterior lens opacity (pathognomonic, permanent) |
| Corneal decompensation | Bullous keratopathy from endothelial damage |
| Cataract | From ischaemic lens damage (subcapsular) |
| Iris atrophy | Spiral-shaped ischaemic iris necrosis |
| Peripheral anterior synechiae (PAS) | Permanent angle closure; correlates with poor IOP control |
| Posterior synechiae | Irregular pupil, risk of seclusio pupillae |
| Optic atrophy | Pallor + cupping; permanent visual field loss |
| Malignant glaucoma | Post-treatment aqueous misdirection (rare) |
| Fellow eye attack | 50% risk within 5 years without prophylactic LPI |
PRIMARY OPEN-ANGLE GLAUCOMA (POAG)
10-Mark University Examination Notes
1. DEFINITION
Primary open-angle glaucoma (POAG) is a chronic, progressive optic neuropathy of adult onset characterized by:
- Retinal nerve fibre layer (RNFL) thinning
- Glaucomatous optic nerve head damage (increased cup-to-disc ratio)
- Characteristic progressive visual field loss
- Open anterior chamber angle on gonioscopy
- No secondary cause for the optic neuropathy
IOP is a key modifiable risk factor, though POAG can occur at normal IOP (normal tension glaucoma, IOP <21 mmHg). It is the most common type of glaucoma worldwide (most prevalent in Black and White populations).
2. ETIOLOGY
Primary Risk Factors
| Risk Factor | Significance |
|---|---|
| Elevated IOP | The higher the IOP, the greater the likelihood; asymmetry ≥4 mmHg is significant |
| Age | More common with increasing age; prevalence ~6% in White >70 yr |
| Race | 4× more common in Black populations; earlier onset, harder to control |
| Family history | Siblings: 4× risk; offspring: 2× risk (first-degree relatives) |
| Myopia | Associated with increased incidence; myopic eyes more susceptible to damage |
| Large optic disc | More vulnerable to glaucomatous damage |
| Low ocular perfusion pressure | Difference between arterial BP and IOP |
Genetic Factors
- MYOC gene mutation (myocilin - found in trabecular meshwork)
- OPTN gene mutation (optineurin)
- At least 127 loci associated with POAG in genome-wide association studies
Other Risk Factors
- Vascular disease (systemic hypertension, cardiovascular disease, migraine/vasospasm)
- Translaminar pressure gradient (difference between IOP and CSF pressure)
- Systemic calcium-channel blockers (meta-analysis: higher glaucoma prevalence)
- Diabetes mellitus (association less clear-cut)
- Anti-VEGF therapy (sustained IOP elevation, especially bevacizumab, after recurrent injections)
3. PATHOGENESIS
POAG has two major theories (likely both contribute):
A. Mechanical Theory
Elevated IOP causes direct mechanical deformation of the lamina cribrosa (a fenestrated collagen plate through which axons of the retinal ganglion cells pass at the optic nerve head).
HIGH IOP → Lamina cribrosa deformation
→ Compression/distortion of axon bundles
→ Axoplasmic flow obstruction
→ Retinal ganglion cell (RGC) death
→ RNFL thinning
→ Optic cup enlargement (glaucomatous cupping)
→ Visual field defects
B. Vascular Theory
Inadequate perfusion of the optic nerve head (due to low ocular perfusion pressure or vasospasm) leads to ischaemic ganglion cell death independent of IOP level (explains normal tension glaucoma).
Trabecular Meshwork Dysfunction
The fundamental outflow defect is increased resistance in the trabecular meshwork and Schlemm's canal, causing elevated IOP. The angle itself remains open. Causes include:
- Accumulation of extracellular matrix in trabecular beams
- Loss of trabecular endothelial cells
- Increased stiffness of trabecular meshwork (MYOC mutations)
- Oxidative damage to trabecular cells
Diagram: Pathogenesis of POAG
Trabecular meshwork dysfunction
↓
Increased aqueous outflow resistance
↓
ELEVATED IOP (or normal IOP + vascular insufficiency)
↓
Lamina cribrosa deformation + Optic nerve head ischaemia
↓
Retinal ganglion cell (RGC) axon damage/death
↓
Retinal nerve fibre layer (RNFL) thinning
↓
Optic disc cupping (vertical C/D ratio ↑, rim thinning)
↓
Visual field defects (arcuate, nasal step, tunnel vision)
↓
Blindness (if untreated)
4. CLINICAL FEATURES
POAG is the "sneak thief of sight" - it is asymptomatic until advanced.
Symptoms
- Usually none in early-to-moderate disease
- Patients typically present incidentally (routine refraction, screening)
- Late: blurred vision, reduced peripheral vision
- Central vision is preserved until very late stage
Signs
1. IOP Elevation
- Usually >21 mmHg (though may be normal in normal tension glaucoma)
- Diurnal variation: highest in morning
2. Optic Disc Changes (most important)
NORMAL DISC GLAUCOMATOUS DISC
┌────────────┐ ┌────────────┐
│ Rim (pink)│ │ ↑ Cup │
│ ┌──────┐ │ │ ┌──────┐ │ ← Thinned rim
│ │ Cup │ │ │ │Large │ │
│ │ small│ │ │ │cup │ │
│ └──────┘ │ │ └──────┘ │
└────────────┘ └────────────┘
C/D ratio ~0.3 C/D ratio >0.6, asymmetry >0.2
Key optic disc signs:
- Increased cup-to-disc (C/D) ratio (>0.6 suspicious; >0.7 significant; asymmetry >0.2 significant)
- ISNT rule violated: Inferior > Superior > Nasal > Temporal rim thickness (normal order) - glaucoma causes preferential inferior and superior rim thinning
- Notching of the neuroretinal rim (typically inferotemporal or superotemporal)
- Disc haemorrhage (Drance haemorrhage) - splinter haemorrhage at disc margin; indicates progression, especially in NTG
- Bayonetting of blood vessels at disc margin
- Nasal shifting of vessels (vessels appear to emerge from the nasal side of the enlarged cup)
- RNFL defects - wedge-shaped darkening seen with red-free illumination
3. Anterior Segment
- Normal-depth anterior chamber
- Open angle on gonioscopy (Grade 3-4 Shaffer)
- Normal cornea
- IOP usually elevated (10-21 mmHg normal; >21 suspicious)
5. VISUAL FIELD CHANGES (Glaucomatous Visual Field Defects)
Visual field defects in POAG follow the pattern of retinal nerve fibre bundles. They respect the horizontal raphe (nasal field defects have a horizontal step). Damage typically occurs in the arcuate fibre bundles (superior > inferior).
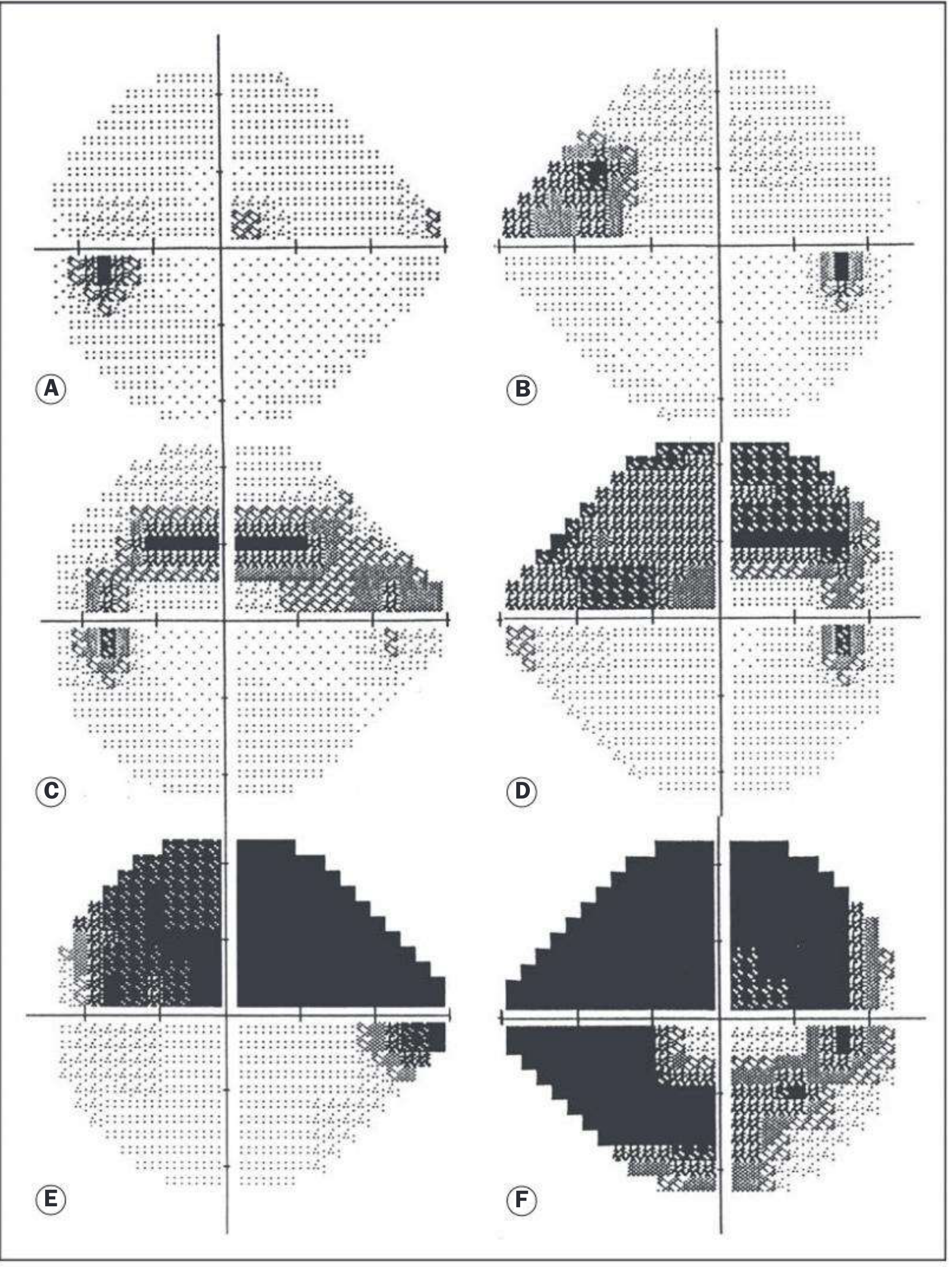
Sequence of visual field defects (A-F as shown above):
Diagram: Progressive Visual Field Loss in POAG
STAGE 1 - Early STAGE 2 - Moderate
┌─────────────────┐ ┌─────────────────┐
│ Normal │ │ Arcuate scotoma │
│ ●blind │ │ ██████████● │
│ spot │ │ ██ (Bjerrum) │
│ │ │ Nasal step │
└─────────────────┘ └─────────────────┘
Small paracentral Arcuate defect from
depressions (superonasal) 10°-20° of fixation;
or nasal step Nasal step (bounded
by horizontal midline)
STAGE 3 - Advanced STAGE 4 - End Stage
┌─────────────────┐ ┌─────────────────┐
│ █████████████ │ │ ████████████│
│ ████ Ring ████│ │ ███ Temporal │
│ ████scotoma████│ │ ███ island │
│ █████████████ │ │ (no nasal │
│ Small │ │ field) │
│ central area │ └─────────────────┘
└─────────────────┘
Ring (annular) scotoma
Named Visual Field Defects in POAG
| Defect | Description | Stage |
|---|---|---|
| Paracentral scotoma | Small depressions within 20° of fixation, often superonasal | Earliest |
| Nasal step (of Ronne) | Sensitivity difference above/below horizontal midline in nasal field; bounded by horizontal raphe | Early |
| Temporal wedge | Less common than nasal step; similar significance | Early |
| Bjerrum/arcuate scotoma | Arcuate defect from blind spot arching around fixation between 10°-20°; follows arcuate fibre bundles | Moderate |
| Double arcuate (ring/annular) scotoma | Superior and inferior arcs coalesce | Advanced |
| Tubular vision (tunnel vision) | Only small central and/or temporal island remains | Advanced |
| Temporal island | Last remaining vision (temporal fibres spared longest) | End stage |
Key principle: The defects respect the horizontal meridian in the nasal field (horizontal raphe of retinal nerve fibres). Central vision is preserved until very late.
6. INVESTIGATIONS
- Tonometry (Goldmann applanation) - IOP measurement; check diurnal curve
- Corneal pachymetry (CCT) - thin cornea (<520 µm) is independent risk factor; thick cornea may give falsely elevated IOP
- Gonioscopy - confirms open angle; grades angle width (Shaffer Grade 3-4)
- Optic disc evaluation - slit lamp biomicroscopy (78D/90D lens) or stereoscopic disc photography; assess C/D ratio, rim, notching, disc haemorrhage
- Visual field testing - Standard Automated Perimetry (SAP, Humphrey Field Analyzer); frequency doubling technology (FDT); detects and monitors progression
- OCT (Optical Coherence Tomography) - quantifies RNFL thickness (superior and inferior poles most sensitive); ganglion cell complex (GCC); detects pre-perimetric changes; monitors progression
- Heidelberg Retinal Tomography (HRT) - 3D optic disc imaging; Moorfields regression analysis
- GDx VCC (Scanning Laser Polarimetry) - RNFL analysis with variable corneal compensation
- Colour fundus photography - disc documentation; RNFL defects with red-free filter
- Blood pressure measurement - to calculate ocular perfusion pressure
7. MANAGEMENT
Target IOP (Key Concept)
A target pressure is set below which further optic nerve damage is considered unlikely. A reasonable initial goal is IOP <18 mmHg (AGIS study showed no significant field progression below this level). Target is individualized based on: existing damage severity, pre-treatment IOP, CCT, age, and rate of progression.
Step 1: Medical Therapy (First-line)
| Drug Class | Examples | Mechanism | IOP Reduction |
|---|---|---|---|
| Prostaglandin analogues (first choice) | Latanoprost 0.005%, Travoprost, Bimatoprost | Increase uveoscleral outflow | 25-33% |
| Beta-blockers | Timolol 0.5% (twice daily), Betaxolol | Reduce aqueous production | 20-25% |
| Alpha-2 agonists | Brimonidine 0.2% | Reduce aqueous production + increase uveoscleral outflow | 20-25% |
| Carbonic anhydrase inhibitors | Dorzolamide (topical), Acetazolamide (oral) | Reduce aqueous production | 15-20% |
| Miotics | Pilocarpine | Open trabecular meshwork by ciliary muscle contraction | 20-25% |
| Rho kinase inhibitors | Netarsudil | Increase trabecular outflow | ~20% |
| Fixed combinations | Timolol-Dorzolamide (Cosopt), Timolol-Bimatoprost | Improve compliance | Additive |
Step 2: Laser Therapy
- Selective Laser Trabeculoplasty (SLT) - selectively targets trabecular meshwork pigmented cells; 40-50 spots at 180° or 360°; can repeat; comparable to medication for initial therapy (LiGHT trial)
- Argon Laser Trabeculoplasty (ALT) - older technique, same principle
Step 3: Surgical Therapy
- Trabeculectomy (guarded filtration surgery) - creates a surgical fistula from anterior chamber to subconjunctival space (filtering bleb); most common glaucoma surgery; mitomycin C (MMC) used to prevent scarring
- Glaucoma drainage devices (tube shunts) - Ahmed, Baerveldt, or Molteno valves; for refractory/complex cases
- Minimally Invasive Glaucoma Surgery (MIGS) - iStent, Hydrus, OMNI (for mild-moderate disease combined with cataract surgery)
- Cyclodiode laser - transscleral ciliary body ablation for refractory glaucoma
Diagram: Trabeculectomy
Conjunctiva
Sclera
┌─────────────────────┐
│ FILTERING BLEB │ ← aqueous collects here subconjunctivally
└────────┬────────────┘
│ fistula
┌────────▼────────────┐
│ Anterior chamber │ ← aqueous drains from here
│ (IOP reduced) │
└─────────────────────┘
Scleral flap + sclerectomy + peripheral iridectomy
8. COMPLICATIONS
Complications of Untreated POAG
| Complication | Description |
|---|---|
| Progressive visual field loss | Arcuate scotomas → ring scotoma → tunnel vision |
| Legal blindness | Visual field <10° (tubular vision); VA may still be 6/6 |
| Total blindness | End-stage optic atrophy |
Complications of Treatment
| Treatment | Complication |
|---|---|
| Prostaglandins | Iris pigmentation, periorbital fat atrophy, hypertrichosis, CME in aphakic eyes |
| Beta-blockers | Bradycardia, bronchospasm, depression, sexual dysfunction |
| Brimonidine | Allergic follicular conjunctivitis (common), CNS depression in children |
| CAIs (oral) | Metabolic acidosis, renal stones, Stevens-Johnson syndrome |
| Trabeculectomy | Bleb failure/leak, endophthalmitis (blebitis), hypotony maculopathy, cataract formation, flat anterior chamber |
COMPARATIVE TABLE: AACG vs. POAG
| Feature | Acute Angle-Closure Glaucoma | Primary Open-Angle Glaucoma |
|---|---|---|
| Onset | Sudden (hours) | Insidious (years) |
| Pain | Severe | None |
| Vision | Severely reduced acutely | Normal until advanced |
| Cornea | Hazy/oedematous | Clear |
| Pupil | Mid-dilated, oval, fixed | Normal (later dilated) |
| AC depth | Shallow | Normal |
| Angle | Closed (Grade 0-1) | Open (Grade 3-4) |
| IOP | 50-80 mmHg (acute) | 22-40 mmHg (chronic) |
| Nausea/vomiting | Yes | No |
| Predisposition | Hypermetropia, shallow AC | None (multifactorial) |
| Race | Asian > European | Black > White > Asian |
| Visual field | Generalized constriction (acute) | Arcuate defects, nasal step, tunnel vision |
| Definitive Rx | Laser peripheral iridotomy (LPI) | Target IOP reduction (medical/SLT/trabeculectomy) |
| Emergency? | Yes - ophthalmic emergency | No - chronic management |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition (Elsevier); Goldman-Cecil Medicine, 2024.
These notes cover all required domains (definition, etiology, pathogenesis, clinical features, investigations, management, complications) at the depth expected for a 10-mark final MBBS examination. The drawable diagrams (aqueous flow, iris bombe mechanism, visual field progression sequence, trabeculectomy, and LPI diagrams) are clearly structured for reproduction in an exam answer. The visual field progression chart from Kanski's (A-F sequence: paracentral scotoma → nasal step → arcuate → double arcuate → ring scotoma → tubular/temporal island) is the single most important diagram for glaucoma questions.
This is a shared conversation. Sign in to Orris to start your own chat.