Thoracic and abdominal parts of the aorta arteries and its branches with images . In "detailed notes" for mbbs student from basics to advance level
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
AORTA - THORACIC & ABDOMINAL PARTS: Detailed MBBS Notes
(Basics to Advanced | Based on Gray's Anatomy for Students)
OVERVIEW: THE AORTA AT A GLANCE
The aorta is the largest artery in the body. It originates from the left ventricle and distributes oxygenated blood to the entire systemic circulation. It is divided into:
| Segment | Location | Vertebral Level |
|---|---|---|
| Ascending aorta | Pericardial sac / anterior mediastinum | TIV (starts at aortic valve) |
| Arch of aorta | Superior mediastinum | TIV/V |
| Descending thoracic aorta | Posterior mediastinum | TIV - TXII |
| Abdominal aorta | Posterior abdominal wall | TXII - LIV |
PART 1: THORACIC AORTA
1A. Ascending Aorta
- Arises from the left ventricle at the level of the lower border of TIV
- Enclosed within the pericardial sac
- Only branches: the two coronary arteries (right and left), which arise from the aortic sinuses (sinuses of Valsalva) just above the aortic valve cusps
- Right coronary artery - supplies SA node, AV node, right ventricle, inferior LV
- Left coronary artery - divides into LAD (anterior interventricular) and LCx (circumflex)
- The ascending aorta becomes the arch when it exits the pericardium
Mnemonic for remembering aorta segments: "All Anatomy Describes Aorta" = Ascending, Arch, Descending, Abdominal
1B. Arch of Aorta
Location: Superior mediastinum, at the level of TIV/V
The arch begins when the ascending aorta exits the pericardial sac. It courses upward, backward, and to the LEFT - reaching the mid-level of the manubrium of the sternum. It ends on the left side at vertebral level TIV/V.
The arch is initially anterior and finally lateral to the trachea.
Fig. 3.93 - Arch of Aorta and its Branches (Gray's Anatomy for Students):
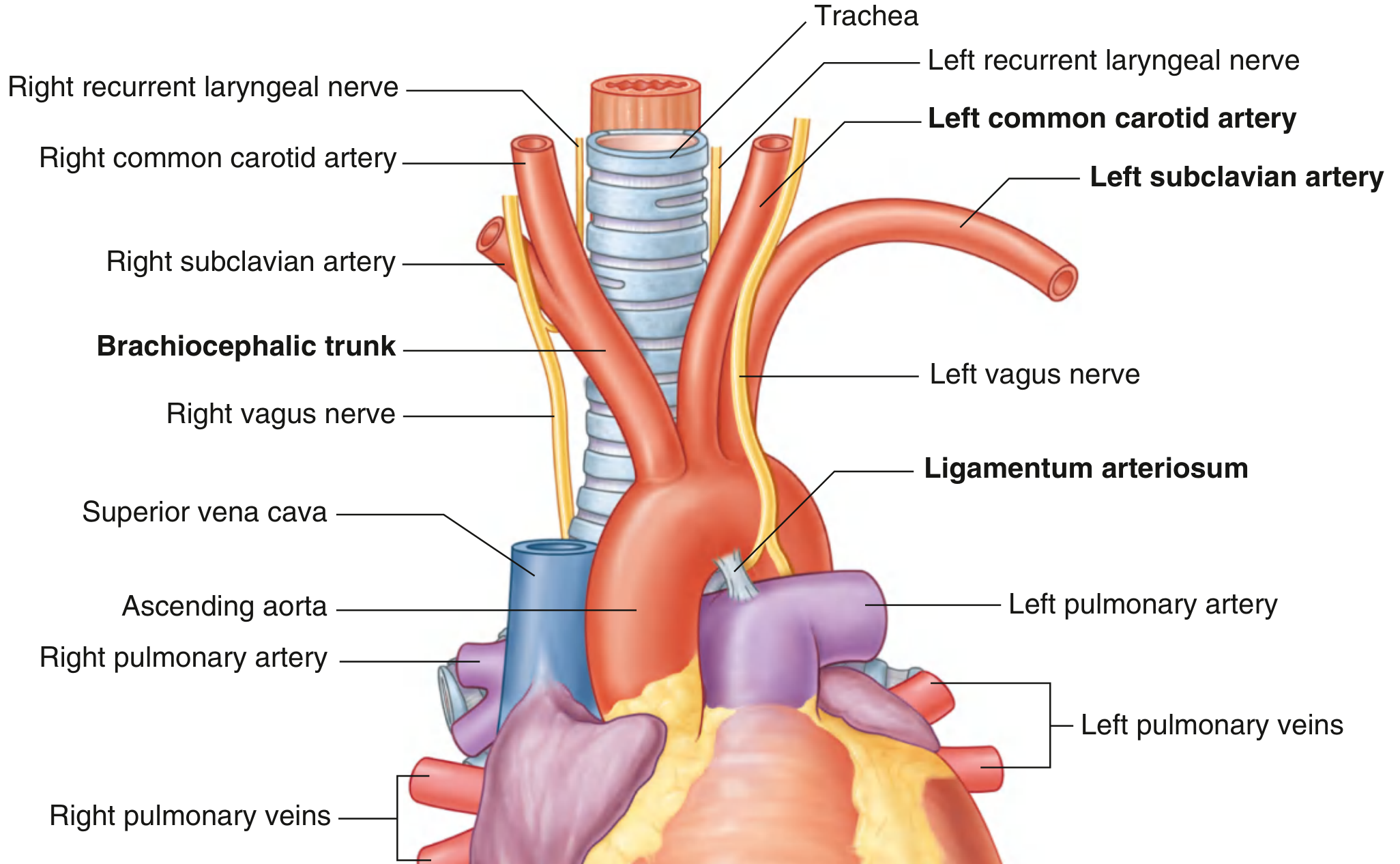
Three Branches from the Superior Border of the Arch
All three branches are crossed anteriorly by the left brachiocephalic vein at their origins.
| Branch | Order | Description | Supply |
|---|---|---|---|
| Brachiocephalic trunk | 1st (rightmost) | Largest branch; arises behind manubrium; divides at upper edge of right sternoclavicular joint into right common carotid + right subclavian arteries | Right side of head/neck + right upper limb |
| Left common carotid artery | 2nd | Arises just left and slightly posterior to brachiocephalic trunk; ascends along left side of trachea | Left side of head and neck |
| Left subclavian artery | 3rd | Arises just left of and slightly posterior to left common carotid artery; ascends along left side of trachea | Left upper limb (major supply) |
Mnemonic for arch branches (Right to Left): "Big Cats Swim" = Brachiocephalic, Common carotid (left), Subclavian (left)
Variant: Thyroid Ima Artery
Occasionally, the brachiocephalic trunk gives off a small thyroid ima artery that contributes additional vascular supply to the thyroid gland.
Ligamentum Arteriosum
- Located in the superior mediastinum
- Connects the pulmonary trunk to the arch of the aorta
- Remnant of the fetal ductus arteriosus (which allowed blood to bypass the lungs during fetal life)
- Closes after birth to form this ligament
- Clinical importance: The ligamentum arteriosum is one of the THREE fixed attachment points of the aorta
1C. Descending Thoracic Aorta
Course: Begins at the lower edge of TIV (where arch ends) → passes through the aortic hiatus of the diaphragm → ends anterior to the lower edge of TXII
- Situated to the left of the vertebral column superiorly
- Approaches the midline inferiorly, lying directly anterior to the lower thoracic vertebral bodies
Fig. 3.104 - Thoracic Aorta and its Branches:
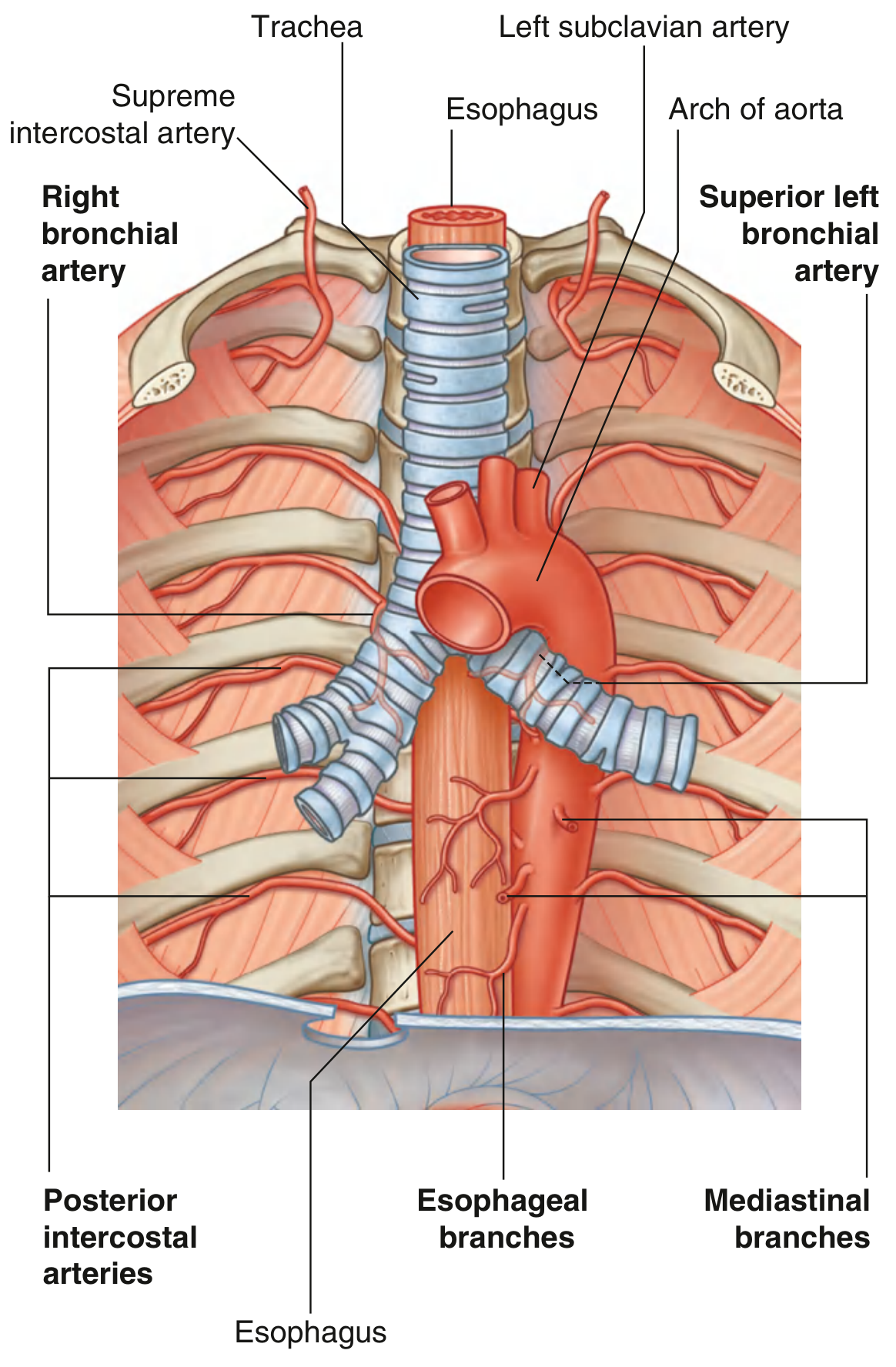
Branches of the Descending Thoracic Aorta (Table 3.3)
| Branch | Details |
|---|---|
| Posterior intercostal arteries | 9 pairs (lower 9 intercostal spaces); arise from posterior surface; upper 2 spaces are supplied by the supreme intercostal artery (branch of costocervical trunk from subclavian) |
| Subcostal artery | Lowest pair of branches; located inferior to rib XII |
| Bronchial arteries | Variable; usually two LEFT bronchial arteries from thoracic aorta; one RIGHT from third posterior intercostal artery or superior left bronchial artery; supply lung parenchyma (not for gas exchange) |
| Esophageal branches | 4-5 vessels from anterior aspect; form a continuous anastomotic chain; anastomose superiorly with inferior thyroid artery branches and inferiorly with left gastric artery branches |
| Pericardial branches | Small vessels to posterior surface of pericardial sac |
| Mediastinal branches | Small branches to lymph nodes, vessels, nerves, and areolar tissue in posterior mediastinum |
| Superior phrenic arteries | From lower thoracic aorta; supply posterior part of superior diaphragm surface; anastomose with musculophrenic and pericardiophrenic arteries |
Key point: The right bronchial artery arises from the third posterior intercostal artery, NOT directly from the thoracic aorta (unlike the two left bronchial arteries).
CLINICAL CORRELATIONS - THORACIC AORTA
Three Fixed Points of the Aorta (High-Yield for Exams)
- The aortic valve
- The ligamentum arteriosum
- The point of passing behind the median arcuate ligament of the diaphragm
These are the sites most vulnerable to traumatic injury in rapid deceleration accidents (road traffic accidents). The rest of the aorta is relatively free from mediastinal attachments.
Coarctation of the Aorta
- Congenital narrowing of the aortic lumen just distal to the left subclavian artery origin
- Blood supply to abdomen and lower limbs is diminished
- Collateral vessels develop over time through the chest wall and abdomen
- Rib notching - dilated tortuous intercostal vessels erode inferior rib margins - visible on CXR
- Cardiac effects: increased afterload → cardiac failure
- Blood pressure difference between arms and legs is a key clinical sign
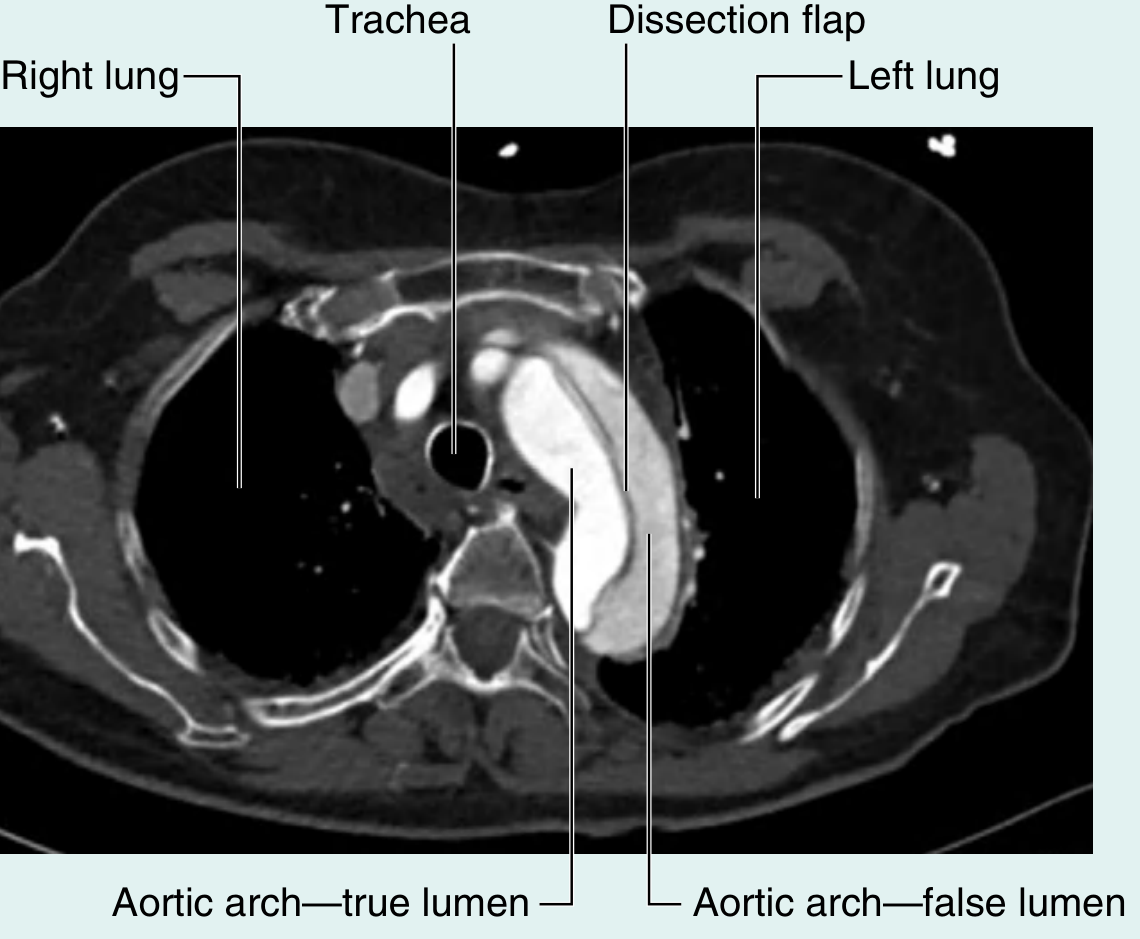
Aortic Dissection
- Splitting of the aortic wall longitudinally between the intima and media
- Creates a "false channel" (true lumen + false lumen)
- Can occur anywhere along the aorta
- If in ascending aorta/arch: can disrupt coronary and cerebral arterial flow → MI or stroke
- If in abdomen: can compromise visceral vessels → bowel or renal ischemia
- Stanford Type A (involves ascending) = surgical emergency; Stanford Type B (descending only) = medical management
CT scan showing aortic dissection (Gray's Anatomy for Students, Fig. 3.94):
Aortic Arch Anomalies
- Right-sided aortic arch: aorta courses to the right of trachea and passes over right main bronchus; can be associated with dextrocardia or complete situs inversus; also associated with aberrant left subclavian artery
- Common origin of brachiocephalic trunk + left common carotid: seen in ~25% of people (a normal variant)
- Aberrant right subclavian artery (arteria lusoria): the right subclavian arises as the last branch of the arch, passes posterior to the esophagus → can cause dysphagia (dysphagia lusoria)
PART 2: ABDOMINAL AORTA
Course and Surface Marking
- Begins: aortic hiatus of the diaphragm at the lower level of vertebra TXII (as a midline structure)
- Ends: just left of midline at the lower level of vertebra LIV, where it bifurcates
- Surface anatomy of bifurcation: approximately 2.5 cm below the umbilicus OR at the level of a line connecting the highest points of the iliac crest (intercristal plane)
- Passes downward on the anterior surface of L1-L4 vertebral bodies
Relations of the Abdominal Aorta
| Direction | Structures |
|---|---|
| Anterior | Prevertebral nerve plexus; pancreas and splenic vein; left renal vein; inferior duodenum |
| Posterior | Vertebral bodies (L1-L4); left lumbar veins (cross posteriorly to IVC) |
| Right | Cisterna chyli, thoracic duct, azygos vein, right crus of diaphragm, inferior vena cava |
| Left | Left crus of diaphragm |
Branches of the Abdominal Aorta - Overview
Branches are classified into three groups:
ABDOMINAL AORTA BRANCHES
├── VISCERAL (supplying organs)
│ ├── Unpaired (anterior)
│ │ ├── Celiac trunk (L1 - foregut)
│ │ ├── Superior mesenteric artery (L1 - midgut)
│ │ └── Inferior mesenteric artery (L3 - hindgut)
│ └── Paired (lateral/anterior)
│ ├── Middle suprarenal arteries
│ ├── Renal arteries (L1-L2)
│ └── Testicular / Ovarian arteries
├── POSTERIOR (body wall / diaphragm)
│ ├── Inferior phrenic arteries
│ ├── Lumbar arteries (4 pairs)
│ └── Median sacral artery
└── TERMINAL
├── Right common iliac artery
└── Left common iliac artery
Complete Table (Table 4.3 from Gray's Anatomy for Students):
| Artery | Branch type | Vertebral level of origin | Parts supplied |
|---|---|---|---|
| Celiac trunk | Anterior (unpaired) | Just inferior to aortic hiatus (L1) | Abdominal foregut |
| Superior mesenteric | Anterior (unpaired) | Just inferior to celiac trunk (L1) | Abdominal midgut |
| Inferior mesenteric | Anterior (unpaired) | L3 (below renal arteries) | Abdominal hindgut |
| Middle suprarenal | Lateral (paired) | Just above renal arteries | Suprarenal glands |
| Renal arteries | Lateral (paired) | L1-L2 (below SMA) | Kidneys |
| Testicular/ovarian | Paired anterior | Below renal arteries | Testes / ovaries |
| Inferior phrenic | Lateral (paired) | Just below aortic hiatus | Diaphragm (inferior surface) |
| Lumbar arteries | Posterior (paired) | 4 pairs | Posterior abdominal wall + spinal cord |
| Median sacral | Posterior (unpaired) | Just above bifurcation | Sacrum and coccyx |
| Common iliac arteries | Terminal | LIV bifurcation | Lower limbs and pelvis |
2A. CELIAC TRUNK (Foregut Artery)
Origin: Anterior surface of abdominal aorta, immediately below the aortic hiatus, anterior to upper vertebra LI
Immediately divides into 3 branches:
Fig. 4.124 - Celiac Trunk Distribution:
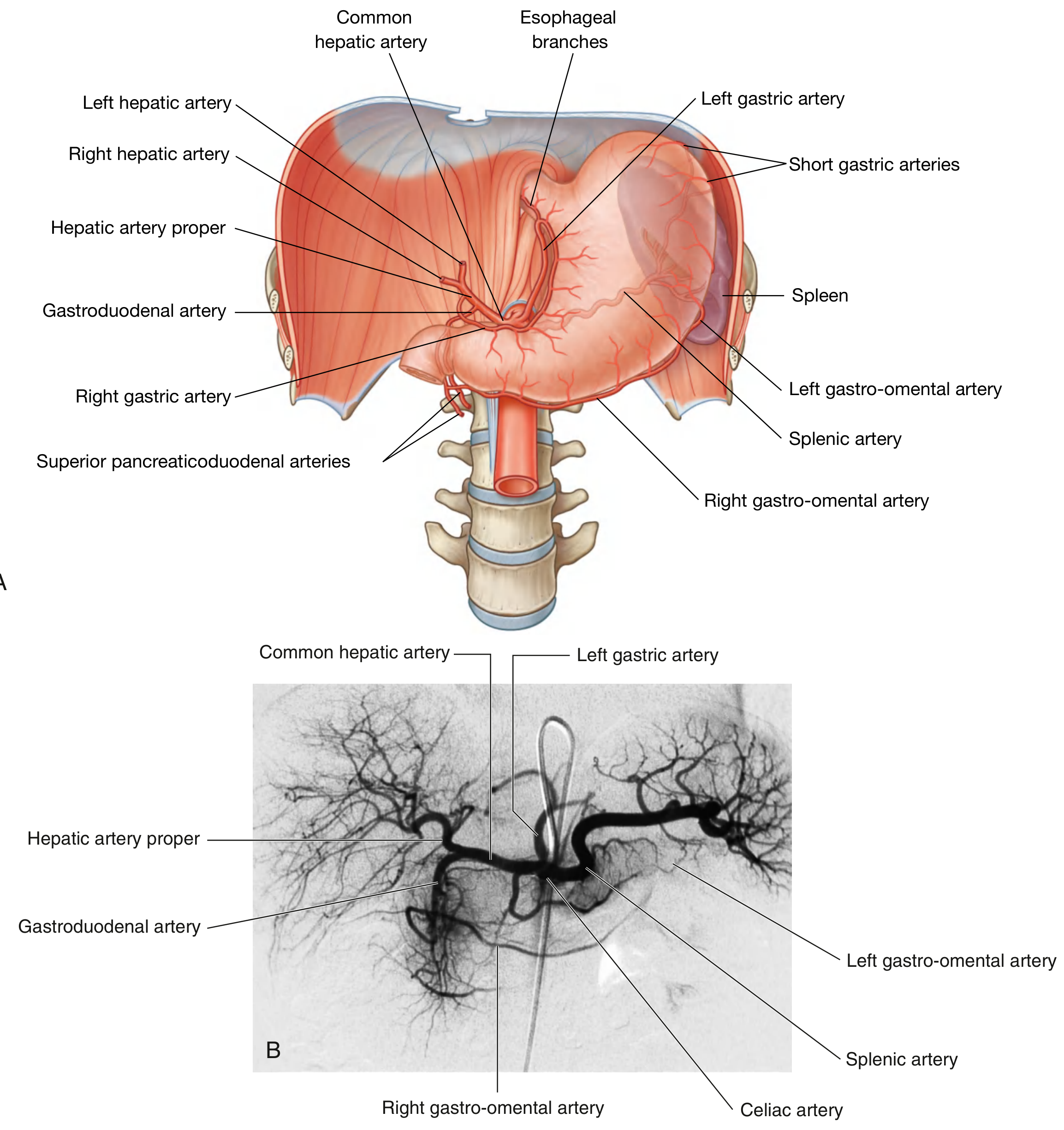
Mnemonic: "Left Spleen Company" = Left gastric, Splenic, Common hepatic
(i) Left Gastric Artery (smallest branch)
- Ascends to the cardioesophageal junction
- Sends esophageal branches upward through the esophageal hiatus (anastomoses with thoracic aorta esophageal branches)
- Turns right and descends along the lesser curvature of the stomach in the lesser omentum
- Anastomoses with right gastric artery
(ii) Splenic Artery (largest branch)
- Takes a tortuous course to the left along the superior border of the pancreas
- Travels in the splenorenal ligament to reach the hilum of the spleen
- Branches along the way:
- Pancreatic branches - supply neck, body and tail of pancreas
- Short gastric arteries - pass through gastrosplenic ligament to supply fundus of stomach
- Left gastro-omental artery - runs along the greater curvature; anastomoses with right gastro-omental artery
(iii) Common Hepatic Artery (medium-sized)
- Runs to the right; divides into:
- Hepatic artery proper - ascends in free edge of lesser omentum; runs LEFT of bile duct, ANTERIOR to portal vein; divides into right and left hepatic arteries near porta hepatis; right hepatic gives the cystic artery to the gallbladder
- Gastroduodenal artery - descends posterior to the first part of the duodenum; divides into right gastro-omental artery and superior pancreaticoduodenal artery
Clinical note: In some individuals, the right hepatic artery arises aberrantly from the SMA (important in liver surgery and transplantation)
2B. SUPERIOR MESENTERIC ARTERY (SMA - Midgut Artery)
Origin: Anterior branch, just below celiac trunk, anterior to lower LI
Anterior relations: Splenic vein, neck of pancreas
Posterior relations: Left renal vein, uncinate process of pancreas, inferior duodenum
Branches (from left and right sides):
Fig. 4.128 - Superior Mesenteric Artery Distribution:
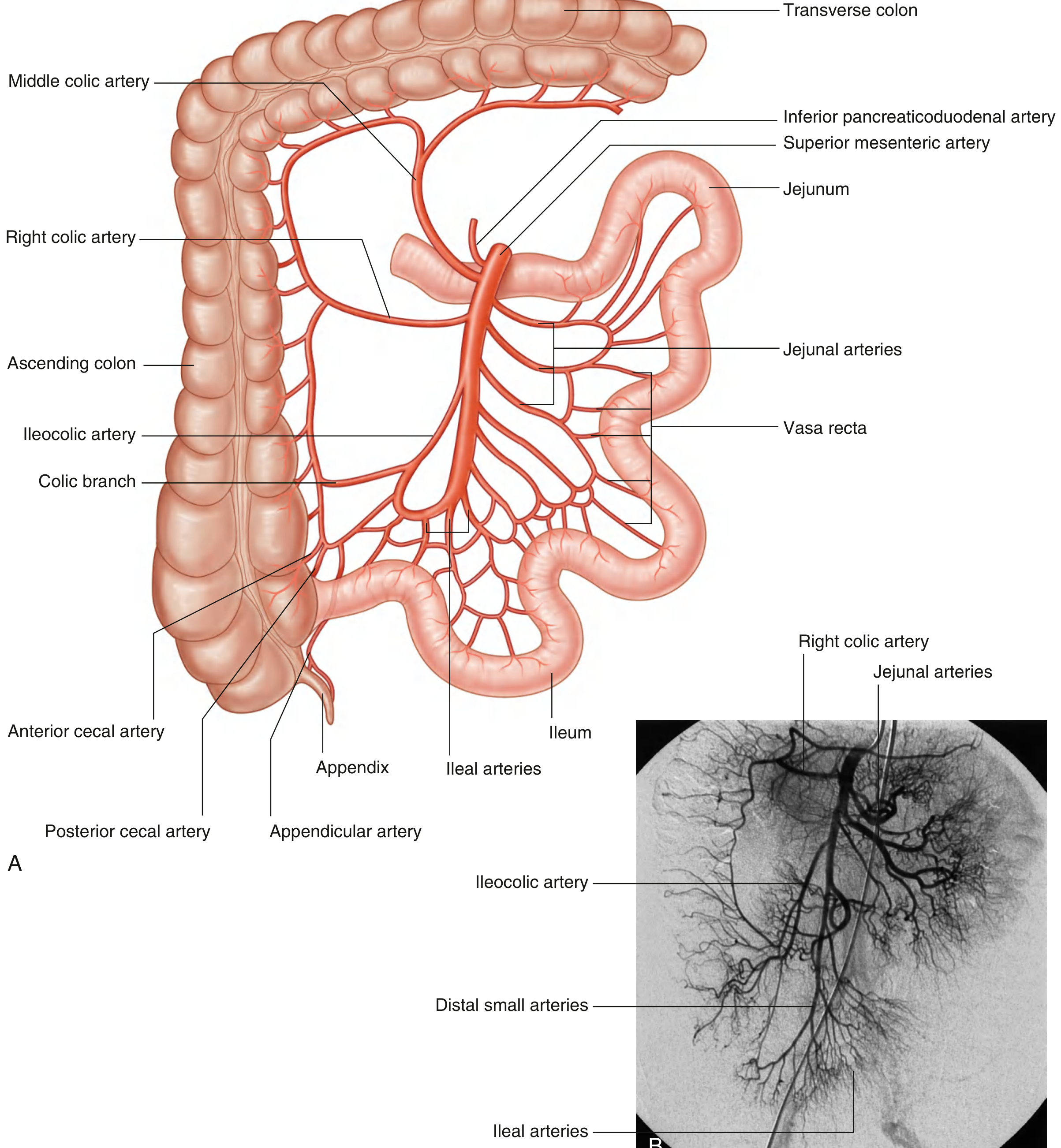
| Branch | Side | Supply |
|---|---|---|
| Inferior pancreaticoduodenal artery | First branch | Head/uncinate of pancreas + duodenum; anastomoses with superior pancreaticoduodenal (from gastroduodenal) |
| Jejunal arteries | Left | Jejunum |
| Ileal arteries | Left | Ileum |
| Middle colic artery | Right | Transverse colon (proximal 2/3) |
| Right colic artery | Right | Ascending colon |
| Ileocolic artery | Right (most distal) | Terminal ileum, cecum, appendix (via appendicular artery) |
Arterial Arcades - High Yield
- Jejunal and ileal arteries form anastomosing arcades in the mesentery before giving off vasa recta (straight arteries) to the bowel wall
- Jejunum: 1-2 arcades; long, closely spaced vasa recta → narrow windows in mesentery
- Ileum: 3-5 arcades; short, widely spaced vasa recta → low, broad windows in mesentery
- This difference is used to distinguish jejunum from ileum during surgery
SMA Syndrome: The SMA passes at an angle over the duodenum; rarely, it can compress the third part of the duodenum causing vomiting (treated with repositioning or surgery)
2C. INFERIOR MESENTERIC ARTERY (IMA - Hindgut Artery)
Origin: Anterior branch, anterior to vertebra LIII (smallest of the three unpaired anterior branches)
Course: Initially descends anteriorly to the aorta, then passes to the LEFT as it continues inferiorly
Branches:
Fig. 4.129 - Inferior Mesenteric Artery Distribution:
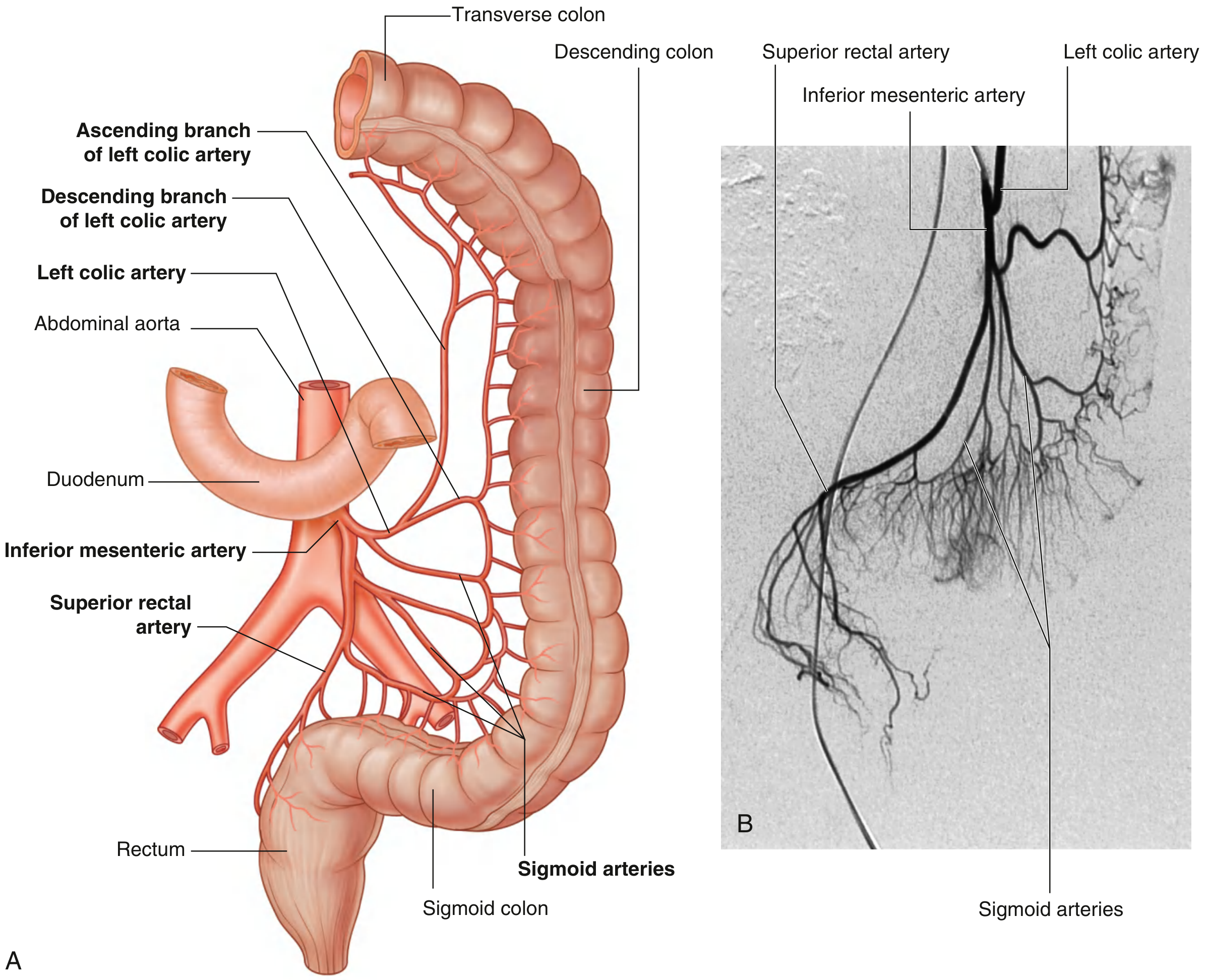
| Branch | Supply |
|---|---|
| Left colic artery (first branch) | Ascending branch: upper descending colon + distal transverse colon (anastomoses with middle colic); Descending branch: lower descending colon |
| Sigmoid arteries (2-4 branches) | Lowest descending colon + sigmoid colon |
| Superior rectal artery (terminal) | Upper rectum; descends into pelvis, crosses left common iliac vessels; anastomoses with middle rectal (internal iliac) and inferior rectal arteries (internal pudendal) |
Marginal Artery of Drummond
- A continuous arterial arcade formed by anastomoses between branches of the SMA and IMA, running along the inner border of the colon from the ileocecal junction to the rectosigmoid junction
- Clinically important as a collateral pathway when either the SMA or IMA is occluded
Critical Point (Sudeck's Point)
- The anastomosis between the last sigmoid artery and the superior rectal artery may be poor near the rectosigmoid junction
- This area (Sudeck's critical point) is at risk of ischemia after IMA ligation in colorectal surgery
2D. PAIRED VISCERAL BRANCHES
Renal Arteries (L1-L2)
- Arise as lateral branches just inferior to the SMA, between L1 and L2
- Right renal artery is longer - passes posterior to the IVC, right renal vein, head of pancreas, and descending duodenum
- Left renal artery is shorter - passes posterior to the left renal vein and the body of the pancreas
- Each artery gives off an inferior suprarenal artery before entering the kidney at the hilum
- The renal artery divides into an anterior and posterior division, then into segmental arteries (5 segments - each is an end artery = no anastomosis → infarction if blocked)
Middle Suprarenal Arteries
- Small lateral branches arising just above the renal arteries
- Part of the triple arterial supply to the adrenal gland:
- Superior suprarenal artery (from inferior phrenic)
- Middle suprarenal artery (from aorta)
- Inferior suprarenal artery (from renal artery)
Gonadal Arteries (Testicular / Ovarian)
- Arise as anterior branches below the renal arteries
- Long slender vessels that pass downward and laterally on the anterior surface of psoas major
- Cross over the ureter ("water under the bridge" - ureter crosses anterior to gonadal vessels)
- In males: pass through the inguinal canal into the scrotum as testicular arteries
- In females: enter the pelvic cavity and pass in the suspensory ligament of the ovary as ovarian arteries
- Embryological note: The gonads develop retroperitoneally at L1 level, which explains the long course of these vessels
2E. POSTERIOR BRANCHES
Inferior Phrenic Arteries
- Arise from the abdominal aorta immediately below the aortic hiatus (or occasionally from the celiac trunk)
- Pass upward to supply the inferior surface of the diaphragm
- Give superior suprarenal branches to the adrenal gland
Lumbar Arteries (4 pairs)
- Arise from the posterior surface of the abdominal aorta in 4 pairs (corresponding to L1-L4)
- Each lumbar artery passes posteriorly around the sides of the vertebral bodies
- Each gives off a dorsal branch (supplies back muscles and skin) and a spinal branch (enters the intervertebral foramen to supply the spinal cord and meninges)
- Clinical note: Lumbar arteries are at risk during abdominal aortic aneurysm repair; their spinal branches can supply the artery of Adamkiewicz
Median Sacral Artery
- Single posterior branch arising just above the aortic bifurcation at LIV
- Passes inferiorly across the lumbar vertebrae, sacrum, and coccyx
- A remnant of the embryonic caudal aorta
2F. TERMINAL BRANCHES
Bifurcation: At the lower level of LIV, just to the LEFT of the midline, approximately 2.5 cm below the umbilicus
The aorta bifurcates into:
- Right common iliac artery
- Left common iliac artery
Each common iliac artery divides at the sacroiliac joint into:
- External iliac artery → becomes the femoral artery (lower limb supply)
- Internal iliac artery → pelvic viscera, perineum, gluteal region
SUMMARY COMPARISON TABLE: FOREGUT vs MIDGUT vs HINDGUT SUPPLY
| Feature | Celiac Trunk | SMA | IMA |
|---|---|---|---|
| Gut territory | Foregut | Midgut | Hindgut |
| Vertebral level | L1 (just below diaphragm) | L1 (just below celiac) | L3 |
| GI structures | Lower esophagus, stomach, duodenum (1st & proximal 2nd part), liver, spleen, pancreas | Rest of duodenum, jejunum, ileum, ascending colon, proximal 2/3 transverse colon | Distal 1/3 transverse colon, descending colon, sigmoid, upper rectum |
| Key anastomosis | Right and left gastric; gastro-omentals | Middle and right colic with marginal artery | Marginal artery; superior rectal with middle/inferior rectal |
HIGH-YIELD CLINICAL TOPICS (Advanced Level)
Abdominal Aortic Aneurysm (AAA)
- Defined as aortic diameter > 3 cm (or > 1.5x normal)
- Most are infrarenal (between renal arteries and bifurcation)
- Risk factors: atherosclerosis, hypertension, smoking, male sex, family history
- Clinically: pulsatile abdominal mass, abdominal/back pain; rupture = life-threatening emergency
- Screening: Ultrasound once in men aged 65 (smokers/ex-smokers)
- Surgery indicated when diameter > 5.5 cm or growing > 1 cm/year
Aortic Occlusion (Leriche Syndrome)
- Chronic occlusion at the aortic bifurcation
- Classic triad: (1) Bilateral hip/buttock/thigh claudication, (2) Impotence, (3) Absent femoral pulses
Celiac Artery Compression Syndrome (Median Arcuate Ligament Syndrome)
- Compression of the celiac trunk by the median arcuate ligament of the diaphragm
- Presents with postprandial epigastric pain, weight loss, and an epigastric bruit
Mesenteric Ischemia
- Acute: Usually from SMA embolus (from cardiac thrombus) or thrombosis - surgical/interventional emergency
- Chronic: Progressive occlusion ("intestinal angina") - postprandial pain, weight loss, food fear
- IMA is less commonly implicated as collateral supply is rich
Renovascular Hypertension
- Renal artery stenosis (usually atherosclerosis in adults, fibromuscular dysplasia in young women) reduces renal blood flow → activates RAAS → hypertension
- Diagnosed by Doppler US, CT angiography, or renal arteriography
EMBRYOLOGICAL NOTES
- The aorta develops from the paired dorsal aortae that fuse in the embryo
- Celiac trunk, SMA, and IMA represent persistent vitelline arteries supplying the yolk sac-derived gut
- The ductus arteriosus connects the pulmonary trunk to the aortic arch in the fetus; after birth it closes → ligamentum arteriosum
- Failure to close = Patent Ductus Arteriosus (PDA) - a congenital heart disease
- Coarctation of the aorta occurs because of abnormal development at the site of the ductus arteriosus
QUICK REVISION MNEMONICS
| Topic | Mnemonic |
|---|---|
| Arch branches (R→L) | Big Cats Swim = Brachiocephalic, (left) Common carotid, (left) Subclavian |
| Celiac trunk branches | Left Spleen Company = Left gastric, Splenic, Common hepatic |
| Abdominal aorta segment order (top to bottom) | I Smell Rotten Gas Today Morning = Inferior phrenic, Superior mesenteric, Renal, Gonadal, Three unpaired (celiac/SMA/IMA), Middle suprarenal (use as a checklist) |
| Gut supply vessels | "Cool Students Inspire" = Celiac (foregut), SMA (midgut), IMA (hindgut) |
| Right renal artery relations | Longer; passes BEHIND IVC |
| Gonadal vs Ureter relation | "Ureter = Umbrella over Gondola" = ureter crosses anterior to gonadal vessels |
Sources: Gray's Anatomy for Students (9780323934237), p. 257-267, p. 407-454 | General Anatomy and Musculoskeletal System - THIEME Atlas | Bailey and Love's Short Practice of Surgery 28th Edition
Can you give me the arteries and it's branches like a column and step wise
Here is the complete stepwise columnar breakdown of the aorta and all its branches:
AORTA - Complete Stepwise Branch Tree
THORACIC AORTA
SEGMENT 1: ASCENDING AORTA
ASCENDING AORTA
├── Right Coronary Artery (RCA)
│ ├── Conus artery (to right ventricular outflow tract)
│ ├── SA nodal artery (60% of people)
│ ├── Right marginal artery
│ ├── AV nodal artery (80% of people)
│ └── Posterior descending artery (PDA) - in right dominant circulation
│
└── Left Coronary Artery (LCA)
├── Left Anterior Descending (LAD)
│ ├── Diagonal branches (D1, D2)
│ └── Septal perforators
└── Left Circumflex (LCx)
├── Obtuse marginal branches (OM1, OM2)
└── SA nodal artery (40% of people)
SEGMENT 2: ARCH OF AORTA
ARCH OF AORTA
├── 1st Branch → BRACHIOCEPHALIC TRUNK (largest)
│ ├── Right Common Carotid Artery
│ │ ├── Right Internal Carotid Artery
│ │ │ ├── Ophthalmic artery
│ │ │ ├── Anterior cerebral artery
│ │ │ ├── Middle cerebral artery
│ │ │ └── Posterior communicating artery
│ │ └── Right External Carotid Artery
│ │ ├── Superior thyroid artery
│ │ ├── Ascending pharyngeal artery
│ │ ├── Lingual artery
│ │ ├── Facial artery
│ │ ├── Occipital artery
│ │ ├── Posterior auricular artery
│ │ ├── Superficial temporal artery
│ │ └── Maxillary artery
│ └── Right Subclavian Artery
│ ├── Vertebral artery
│ ├── Internal thoracic (mammary) artery
│ │ ├── Anterior intercostal arteries (upper 6 spaces)
│ │ ├── Pericardiophrenic artery
│ │ └── Musculophrenic artery
│ ├── Thyrocervical trunk
│ │ ├── Inferior thyroid artery
│ │ ├── Suprascapular artery
│ │ └── Transverse cervical artery
│ ├── Costocervical trunk
│ │ ├── Supreme intercostal artery (→ 1st & 2nd posterior intercostals)
│ │ └── Deep cervical artery
│ └── Dorsal scapular artery
│
├── 2nd Branch → LEFT COMMON CAROTID ARTERY
│ ├── Left Internal Carotid Artery
│ │ └── (same branches as right - cerebral circulation)
│ └── Left External Carotid Artery
│ └── (same 8 branches as right side)
│
└── 3rd Branch → LEFT SUBCLAVIAN ARTERY
└── (same branches as right subclavian)
SEGMENT 3: DESCENDING THORACIC AORTA
DESCENDING THORACIC AORTA (T4 → T12)
│
├── Pericardial branches (small, to posterior pericardium)
│
├── Bronchial arteries
│ ├── Left Superior Bronchial artery (from thoracic aorta)
│ ├── Left Inferior Bronchial artery (from thoracic aorta)
│ └── Right Bronchial artery (from 3rd posterior intercostal artery)
│
├── Esophageal branches (4-5 vessels, anterior aspect)
│ ├── Superiorly anastomose with esophageal br. of inferior thyroid artery
│ └── Inferiorly anastomose with esophageal br. of left gastric artery
│
├── Mediastinal branches (to lymph nodes, nerves, areolar tissue)
│
├── Posterior Intercostal Arteries — 9 PAIRS (spaces 3 to 11)
│ Each intercostal artery gives:
│ ├── Dorsal branch
│ │ ├── Spinal branch (to spinal cord via intervertebral foramen)
│ │ └── Muscular/cutaneous branches (back muscles & skin)
│ ├── Collateral branch (runs along upper border of rib below)
│ └── Lateral cutaneous branch
│ [Note: Spaces 1 & 2 → from Supreme Intercostal Artery (costocervical trunk)]
│
├── Superior Phrenic Arteries (paired, small)
│ └── Posterior superior surface of diaphragm
│
└── Subcostal Arteries (1 pair — below rib 12)
└── Posterior abdominal wall
ABDOMINAL AORTA
SEGMENT 4: ABDOMINAL AORTA (T12 → L4)
UNPAIRED ANTERIOR BRANCHES
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
CELIAC TRUNK (L1 — FOREGUT)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
│
├── LEFT GASTRIC ARTERY (smallest)
│ ├── Esophageal branches (→ anastomose with thoracic aorta esophageal br.)
│ └── Gastric branches (lesser curvature, both surfaces)
│ └── Anastomoses with RIGHT GASTRIC ARTERY
│
├── SPLENIC ARTERY (largest, tortuous)
│ ├── Pancreatic branches
│ │ ├── Dorsal pancreatic artery
│ │ ├── Great pancreatic artery (arteria pancreatica magna)
│ │ └── Caudal pancreatic artery
│ ├── Short gastric arteries (5-7 branches → fundus of stomach)
│ └── Left Gastro-omental (gastro-epiploic) artery
│ └── Anastomoses with RIGHT GASTRO-OMENTAL artery (along greater curvature)
│
└── COMMON HEPATIC ARTERY
│
├── HEPATIC ARTERY PROPER
│ ├── Right Hepatic Artery
│ │ ├── Cystic artery → gallbladder
│ │ └── Right lobe of liver
│ └── Left Hepatic Artery
│ └── Left lobe of liver
│
└── GASTRODUODENAL ARTERY
├── Right Gastro-omental (gastro-epiploic) artery
│ └── Greater curvature of stomach (right side)
└── Superior Pancreaticoduodenal artery
├── Anterior superior pancreaticoduodenal artery
└── Posterior superior pancreaticoduodenal artery
└── Anastomose with INFERIOR pancreaticoduodenal
branches from SMA (forming pancreaticoduodenal arcade)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
SUPERIOR MESENTERIC ARTERY — SMA (L1 — MIDGUT)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
│
├── INFERIOR PANCREATICODUODENAL ARTERY (1st branch)
│ ├── Anterior inferior pancreaticoduodenal artery
│ └── Posterior inferior pancreaticoduodenal artery
│ └── Anastomose with SUPERIOR pancreaticoduodenal arteries (from celiac)
│
├── JEJUNAL ARTERIES (left side — 4-6 branches)
│ └── Form arterial arcades → Vasa recta → jejunum
│ [1-2 arcades; long closely-spaced vasa recta]
│
├── ILEAL ARTERIES (left side — 9-13 branches)
│ └── Form arterial arcades → Vasa recta → ileum
│ [3-5 arcades; short widely-spaced vasa recta]
│
├── ILEOCOLIC ARTERY (right side — most distal right branch)
│ ├── Ileal branch (→ anastomoses with SMA)
│ ├── Anterior cecal artery
│ ├── Posterior cecal artery
│ ├── Appendicular artery → appendix
│ └── Colic branch → ascending colon (lower part)
│
├── RIGHT COLIC ARTERY (right side)
│ ├── Ascending branch → anastomoses with middle colic
│ └── Descending branch → anastomoses with ileocolic
│ → Supply: ascending colon
│
└── MIDDLE COLIC ARTERY (right side — first right branch)
├── Right branch → anastomoses with right colic
└── Left branch → anastomoses with left colic (IMA)
→ Supply: proximal 2/3 of transverse colon
[Forms part of MARGINAL ARTERY OF DRUMMOND]
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
INFERIOR MESENTERIC ARTERY — IMA (L3 — HINDGUT)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
│
├── LEFT COLIC ARTERY (1st branch)
│ ├── Ascending branch
│ │ ├── Upper descending colon
│ │ ├── Distal transverse colon
│ │ └── Anastomoses with MIDDLE COLIC (SMA)
│ └── Descending branch
│ ├── Lower descending colon
│ └── Anastomoses with 1st sigmoid artery
│
├── SIGMOID ARTERIES (2-4 branches)
│ ├── Lowest descending colon
│ ├── Sigmoid colon
│ ├── Anastomose superiorly with left colic branches
│ └── Anastomose inferiorly with superior rectal artery
│
└── SUPERIOR RECTAL ARTERY (terminal branch of IMA)
├── Descends into pelvis in sigmoid mesocolon
├── Crosses left common iliac vessels
├── Divides at SIII → right and left terminal branches
└── Anastomoses:
├── Middle rectal artery (from internal iliac)
└── Inferior rectal artery (from internal pudendal)
PAIRED LATERAL BRANCHES
PAIRED LATERAL BRANCHES
│
├── MIDDLE SUPRARENAL ARTERIES (paired — just above renal arteries)
│ └── Adrenal glands
│ [triple supply: superior suprarenal (inf. phrenic) +
│ middle suprarenal (aorta) + inferior suprarenal (renal artery)]
│
├── RENAL ARTERIES (paired — L1/L2, below SMA)
│ ├── Right renal artery (longer — passes behind IVC)
│ └── Left renal artery (shorter)
│ Each gives:
│ ├── Inferior suprarenal artery → adrenal gland
│ ├── Ureteric branches → upper ureter
│ └── Anterior division + Posterior division
│ └── 5 Segmental arteries (end arteries — no anastomosis)
│ ├── Apical
│ ├── Upper
│ ├── Anterior inferior
│ ├── Posterior
│ └── Lower
│
└── GONADAL ARTERIES (paired — below renal arteries)
├── In Males → Testicular arteries
│ ├── Pass through inguinal canal
│ └── Supply testes + epididymis
└── In Females → Ovarian arteries
├── Pass in suspensory ligament of ovary
└── Supply ovaries + uterine tubes
[Anastomose with uterine artery — branch of internal iliac]
POSTERIOR BRANCHES
POSTERIOR BRANCHES
│
├── INFERIOR PHRENIC ARTERIES (paired)
│ ├── Supply inferior surface of diaphragm
│ └── Superior suprarenal branches → adrenal glands
│
├── LUMBAR ARTERIES — 4 PAIRS (L1-L4)
│ Each lumbar artery gives:
│ ├── Dorsal branch
│ │ ├── Spinal branch (→ spinal cord via intervertebral foramen)
│ │ │ [L1 branch may be the Artery of Adamkiewicz
│ │ │ — main blood supply to lower 2/3 of spinal cord]
│ │ └── Muscular/cutaneous branches (back muscles & skin)
│ └── Abdominal wall branches
│
└── MEDIAN SACRAL ARTERY (single — just above bifurcation)
└── Sacrum, coccyx, posterior rectum
TERMINAL BRANCHES
TERMINAL BRANCHES (at L4 bifurcation)
│
├── RIGHT COMMON ILIAC ARTERY
│ ├── Right External Iliac Artery
│ │ └── → Femoral Artery (below inguinal ligament)
│ └── Right Internal Iliac Artery (Hypogastric)
│ ├── Anterior division
│ │ ├── Superior vesical artery
│ │ ├── Inferior vesical artery (male) / Vaginal artery (female)
│ │ ├── Middle rectal artery
│ │ ├── Uterine artery (female)
│ │ ├── Obturator artery
│ │ ├── Internal pudendal artery
│ │ │ └── Inferior rectal artery
│ │ └── Inferior gluteal artery
│ └── Posterior division
│ ├── Iliolumbar artery
│ ├── Lateral sacral artery
│ └── Superior gluteal artery
│
└── LEFT COMMON ILIAC ARTERY
└── (same divisions as right)
COMPLETE COLUMNAR SUMMARY
AORTA
│
├── ASCENDING AORTA
│ ├── Right Coronary Artery
│ └── Left Coronary Artery (LAD + LCx)
│
├── ARCH OF AORTA
│ ├── Brachiocephalic Trunk → R. Common Carotid + R. Subclavian
│ ├── Left Common Carotid Artery
│ └── Left Subclavian Artery
│
├── DESCENDING THORACIC AORTA
│ ├── Pericardial branches
│ ├── Bronchial arteries (L×2, R×1)
│ ├── Esophageal branches (4-5)
│ ├── Mediastinal branches
│ ├── Posterior Intercostal arteries (9 pairs)
│ ├── Superior Phrenic arteries
│ └── Subcostal arteries (1 pair)
│
└── ABDOMINAL AORTA
├── Celiac Trunk → L. Gastric + Splenic + Common Hepatic
├── Superior Mesenteric Artery → Inf. Pancreat. +
│ Jejunal + Ileal + Ileocolic + R. Colic + M. Colic
├── Middle Suprarenal arteries (paired)
├── Renal arteries (paired)
├── Gonadal arteries (paired)
├── Inferior Phrenic arteries (paired)
├── Lumbar arteries (4 pairs)
├── Inferior Mesenteric Artery → L. Colic +
│ Sigmoid arteries + Superior Rectal
├── Median Sacral artery
└── BIFURCATION (L4)
├── R. Common Iliac → R. External + R. Internal Iliac
└── L. Common Iliac → L. External + L. Internal Iliac
Tip for exams: Remember the order of abdominal aorta branches top to bottom using - "I Can't See My Testis Going In Lumbar Mess" = Inferior phrenic, Celiac, (Superior) Mesenteric, Middle suprarenal, Testicular/ovarian, Gonadal, Inferior phrenic (already counted), Lumbar arteries, Mesenteric inferior, (Median) Sacral
This is a shared conversation. Sign in to Orris to start your own chat.