I now have everything needed for a comprehensive, well-sourced answer. Let me compile it.
Myocardial Infarction: ECG Presentations, Clinical Suspicion, and Management Protocols
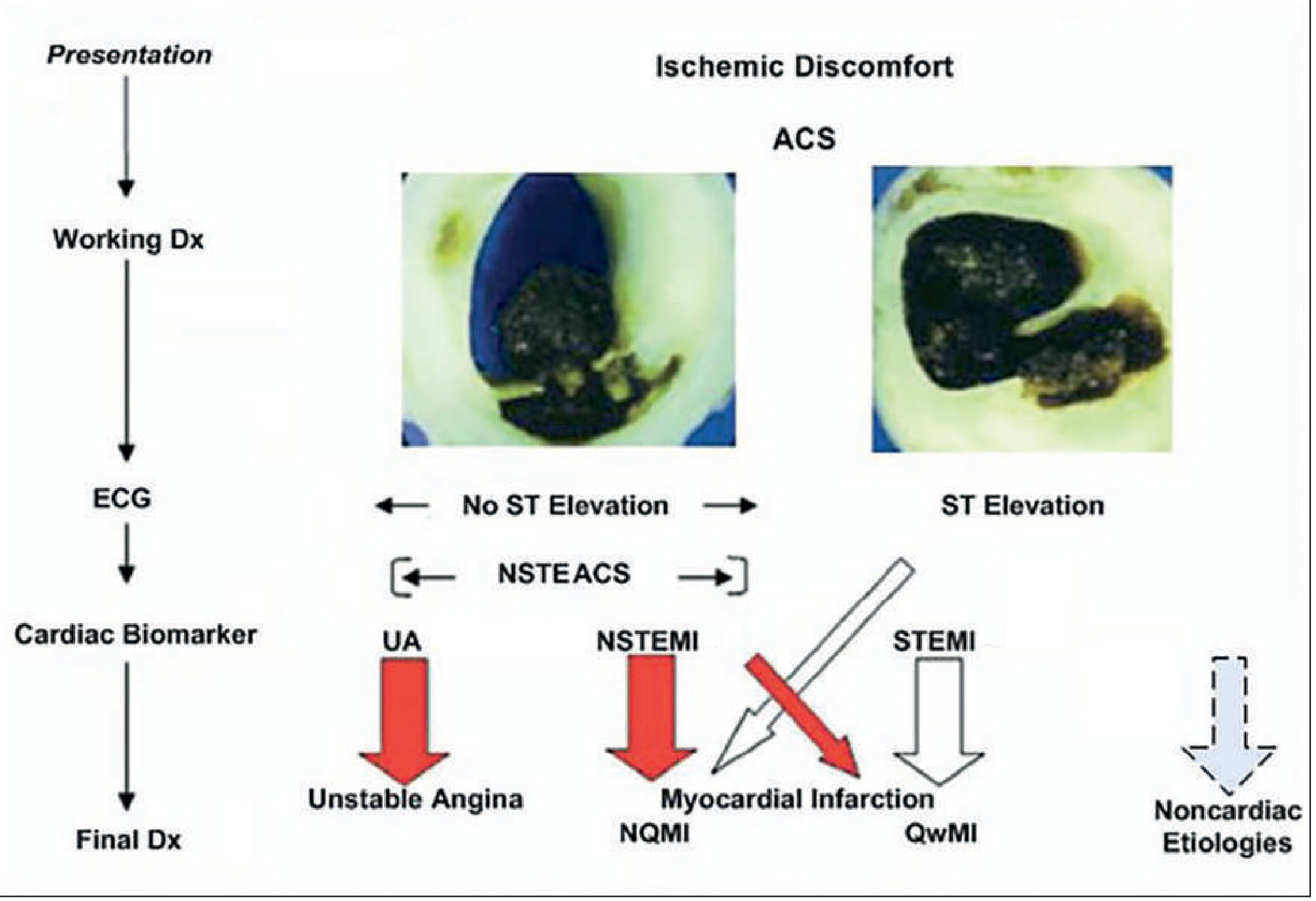
ACS Diagnostic Framework
ACS diagnostic pathways - Goldman-Cecil Medicine
The ECG is the single best initial test for MI but is fallible. The 12-lead should be obtained and interpreted within 10 minutes of patient arrival. - Tintinalli's Emergency Medicine, p. 378
PART 1: ECG PRESENTATIONS OF MI
The Classic Temporal Evolution (Mnemonic: "HATE Q")
| Phase | ECG Finding | Time Frame |
|---|
| H - Hyperacute T waves | Broad, tall, peaked T waves | Minutes (earliest sign) |
| A - sT-segment Ascent (elevation) | Convex upward ST elevation | Hours |
| T - T-wave inversion | Deep symmetric T-wave inversions | Hours-days |
| E - Q waves Established | Pathological Q waves (>0.04s, >25% QRS) | Hours-days |
| (Q) - Q waves persist | May become permanent "tombstone" | Weeks-months |
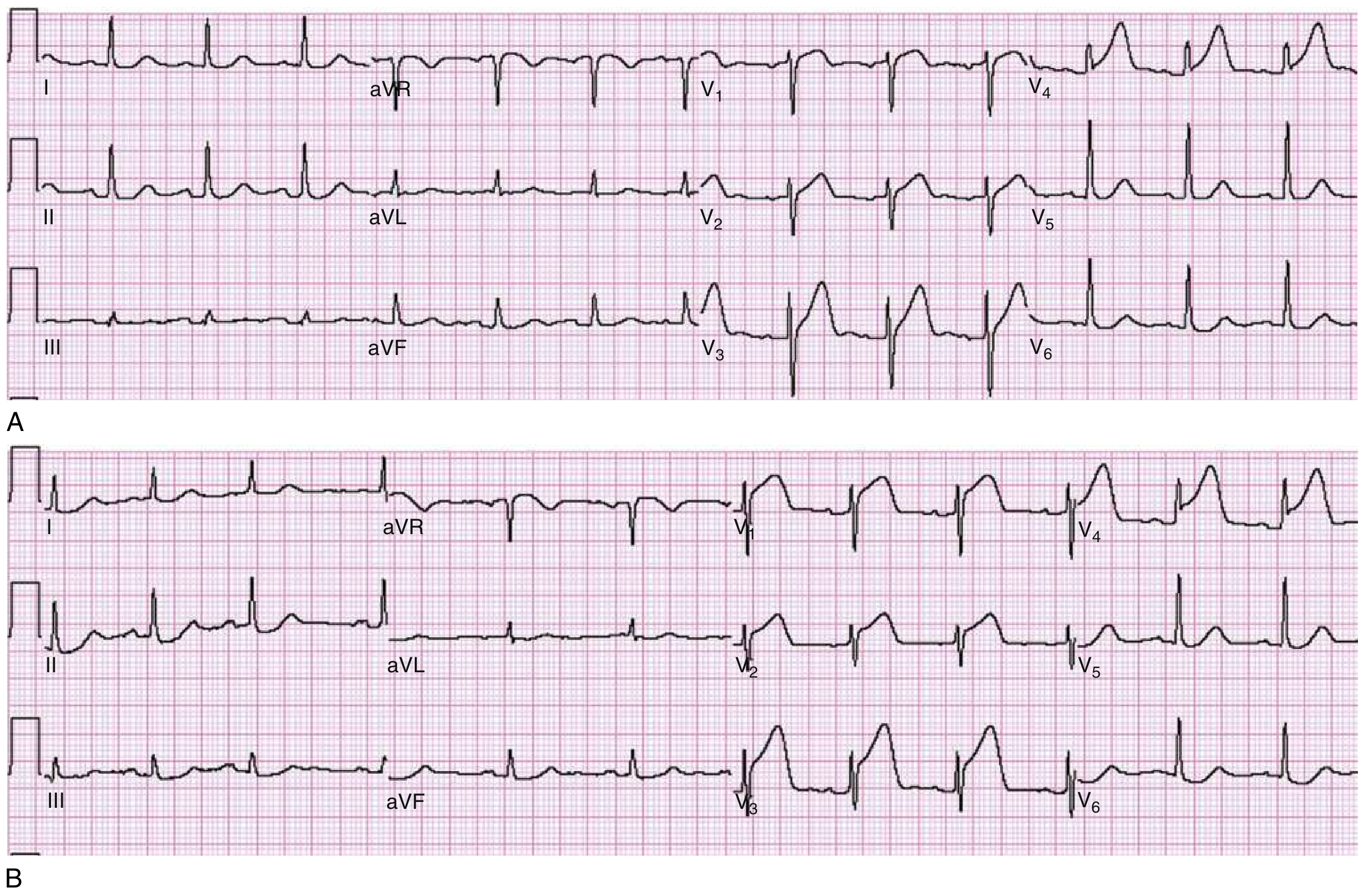
The classic ECG of Anterior STEMI: hyperacute T waves evolving to full ST elevation:
Panel A: hyperacute T waves in V3-V4 with early ST rise in V1-V2. Panel B: Same patient 30 minutes later - full STEMI in V1-V4. - Rosen's Emergency Medicine, Fig. 64.1
1A. STEMI - Anatomic Lead Localization (Mnemonic: "All Indians Lie Poste Right")
| Territory | Leads Involved | Culprit Vessel |
|---|
| Anteroseptal | V1-V3 | Proximal LAD |
| Anterior | V1-V4 | LAD |
| Anterolateral | V1-V6, I, aVL | Proximal LAD or LCx |
| Lateral (high) | I, aVL | Diagonal or LCx |
| Inferior | II, III, aVF | RCA (85%) or LCx |
| Posterior (true) | Tall R in V1-V2, R/S ≥1, ST depression V1-V3 (mirror image) | RCA or LCx |
| Right Ventricular | II, III, aVF + ST elevation in V3R-V6R | Proximal RCA |
Key rule: Any inferior STEMI (II, III, aVF elevation) - always obtain a right-sided ECG for RV infarction. ST elevation ≥1mm in V4R is the most sensitive finding. - Tintinalli's, Table 49-4
1B. STEMI Equivalents (Mnemonic: "WDAP" - these do NOT look like classic STEMI but require emergent cath)
1. Wellens Syndrome
- Type A (25%): Biphasic T waves in V2-V3 (negative then positive)
- Type B (75%): Deep symmetric T inversions in V2-V3
- ECG features: isoelectric or minimally elevated ST (<1mm), no Q waves, no significant R-wave loss
- Represents LAD stenosis - natural history is progression to massive anterior STEMI
- Key point: patient may be pain-free when this is seen; do NOT stress test these patients - Rosen's EM, p. 1001
2. De Winter Pattern
- Upsloping ST depression at the J point with tall, symmetric (hyperacute) T waves in precordial leads V1-V6
- ST elevation in aVR
- Represents proximal LAD occlusion - functionally equivalent to anterior STEMI
- Present in ~2% of LAD occlusions; does NOT evolve to classic ST elevation
- 2026 systematic review: thrombolysis is considered when PCI is delayed (PMID: 41663344)
3. aVR Elevation Pattern
- ST elevation in aVR (≥1mm) with diffuse ST depression in ≥8 leads
- Indicates left main or proximal LAD occlusion (severe multivessel disease / ischemia)
- High mortality; treated as emergent - newly reclassified from "STEMI equivalent" to "High-Risk NOMI" in 2026 literature (PMID: 41798790)
4. Posterior MI
- Classic 12-lead shows: ST depression in V1-V3, tall/broad R wave in V1-V2, R/S ratio ≥1, upright T in V1
- These are reciprocal of posterior ST elevations
- Confirm with posterior leads (V7-V9): ST elevation ≥0.5mm
- Always associated with inferior or lateral MI
1C. NSTEMI and Non-Diagnostic ECG Changes
| Finding | Significance |
|---|
| Horizontal or downsloping ST depression | Subendocardial ischemia, NSTEMI |
| Diffuse ST depression in multiple leads with ST elevation in aVR | Left main / proximal LAD disease |
| Symmetric, narrow T-wave inversions | Ischemia (especially Wellens) |
| Nonspecific ST-T changes | May be only finding in NSTEMI |
| Normal ECG | Present in 1-6% of AMI patients at first presentation |
Harrison's 22e, p. 1915: "With ischemia confined primarily to the subendocardium, the ST vector shifts toward the subendocardium and ventricular cavity, so overlying leads show ST depression with ST elevation in aVR."
1D. Confounding Patterns - When ECG Interpretation Is Difficult
Left Bundle Branch Block (LBBB) - Modified Sgarbossa Criteria
LBBB normally produces discordant ST-T changes (ST moves opposite to QRS). AMI is diagnosed when you see concordant or disproportionate changes:
Original Sgarbossa (scored):
- Concordant ST elevation ≥1mm in leads with positive QRS = 5 points
- Concordant ST depression ≥1mm in V1-V3 = 3 points
- Discordant ST elevation ≥5mm = 2 points
- Score ≥3 = highly specific for AMI
Modified (Smith) Criteria - more sensitive:
- Concordant ST elevation ≥1mm = positive
- Concordant ST depression ≥1mm in V1-V3 = positive
- Proportionally excessive discordant ST elevation: ST/S ratio ≤ -0.25 (ST:S ratio <-0.25)
Important update: A new LBBB alone is NO LONGER a STEMI equivalent in 2025 ACC/AHA guidelines. <10% of new LBBB patients have AMI. Sgarbossa criteria are required. - Rosen's EM, p. 1028
Ventricular Paced Rhythm (VPR)
- Mimics LBBB pattern; apply same Sgarbossa criteria
- Pacemaker spikes precede QRS; leads V5-V6 often predominantly negative (unlike true LBBB)
Right Bundle Branch Block (RBBB) in ACS
- RBBB does NOT obscure inferior or anterior ST elevations as much as LBBB
- New RBBB with ACS presentation carries independent adverse prognosis (PMID: 39546998)
- ST elevation in V1-V3 behind RBBB can still indicate STEMI
Left Ventricular Aneurysm
- Persistent ST elevation after old MI (weeks to months)
- Well-formed Q waves in V2-V5 with absent reciprocal changes - key differentiator from acute STEMI
PART 2: WHEN TO SUSPECT MI EVEN WITH A NORMAL ECG
The 3 Groups Where ECG Fails Most Often
Group 1: Posterior MI
- Standard ECG shows only mirror-image changes (tall R, upright T, ST depression V1-V3)
- If suspected: perform posterior leads (V7, V8, V9)
- Mnemonic: "POSTERIOR = MIRROR" - everything is flipped
Group 2: Right Ventricular MI
- Inferior STEMI is the giveaway - then look for RV involvement
- ST elevation in V4R is diagnostic; often isoelectric on standard ECG
- Clinical triad: hypotension + clear lungs + elevated JVP in setting of inferior STEMI = RV infarct
- AVOID nitrates (preload-dependent); give IV fluids first
Group 3: Very Early Presentation (<2 hours)
- May show only nonspecific changes or be completely normal
- Serial ECGs every 15-30 minutes mandatory
- High-sensitivity troponin is the key adjunct
Clinical Suspicion When ECG Is Normal - Patient-Specific Red Flags
Use the mnemonic "DOWE SAD" for high-risk groups with normal ECGs:
| Letter | Group | Why ECG Can Be Normal/Misleading |
|---|
| D | Diabetics | Silent ischemia - neuropathy blunts chest pain and autonomic response; may present with fatigue, nausea, or hyperglycemia alone |
| O | Older adults (>75y) | Atypical presentation common; dyspnea, confusion, syncope, or weakness as primary complaint |
| W | Women | More likely to present with dyspnea, nausea, jaw pain, fatigue, or back pain rather than classic chest pain; higher false-negative ECG rate |
| E | Early presenters (<2h) | ECG changes may not have developed yet |
| S | Posterior/lateral MI | Not well-represented on standard 12-lead |
| A | aVR/left main occlusion | May look like diffuse ischemia rather than focal STEMI |
| D | Deep circumflex occlusion | LCx is "ECG-silent" - very posterior territory; standard leads miss it |
"Silent ischemia and silent MI are most common in diabetics, older adults, and women." - US Pharmacist review of 2025 ACC/AHA guidelines
Risk Stratification Scores for Suspected ACS
TIMI Risk Score (0-7 points):
- Age ≥65 years (+1)
- ≥3 CAD risk factors (+1)
- Known coronary stenosis ≥50% (+1)
- Aspirin use in past 7 days (+1)
- ≥2 anginal events in past 24h (+1)
- ST deviation ≥0.5mm (+1)
- Elevated cardiac markers (+1)
GRACE Score: preferred in 2023 ESC guidelines for continuous risk stratification using 8 variables. Score >140 = high-risk, warrants early invasive strategy.
HEART Score (most ED-friendly): History, ECG, Age, Risk factors, Troponin - uses only high-sensitivity troponin.
PART 3: ACUTE MI PROTOCOL - WHEN AND WHAT TO GIVE
Immediate "MONA BASH" Protocol (first 10-30 minutes)
| Drug | Indication | Dose |
|---|
| M - Morphine | Pain unresponsive to nitrates (use cautiously - may impair P2Y12 absorption) | 2-4mg IV titrate |
| O - Oxygen | Only if SpO2 <90% - do NOT give routinely (worsens outcomes if normoxic) | Titrate to >90% |
| N - Nitrates | Chest pain relief, hypertension, pulmonary edema | SL 0.4mg q5min x3, then IV |
| A - Aspirin | ALL suspected ACS immediately | 162-325mg chewed (non-enteric coated) |
| B - Beta-blocker | HR control, anti-ischemic | Oral metoprolol; avoid IV if any signs of HF/shock |
| A - Anticoagulation | All STEMI and NSTEMI | UFH (preferred if going to PCI) or LMWH |
| S - Statin (high-intensity) | All ACS | Atorvastatin 80mg or rosuvastatin 40mg |
| H - Heparin (P2Y12 inhibitor) | STEMI: before PCI; NSTEMI: after risk stratification | Ticagrelor 180mg or clopidogrel 600mg loading |
Key caveat on Nitrates: CONTRAINDICATED in:
- RV infarction (causes fatal hypotension - preload dependent)
- Recent phosphodiesterase-5 inhibitor use (sildenafil/tadalafil within 24-48h)
- Systolic BP <90 mmHg
STEMI-Specific: Reperfusion Strategy
Primary PCI is the gold standard if:
- Door-to-balloon time <90 minutes (or <120 min if transfer needed)
- Available 24/7 at a capable center
Fibrinolysis if PCI not available within 120 minutes:
- Give within 30 minutes of ED arrival (door-to-needle time)
- Agents: tPA, tenecteplase (TNK), reteplase
- Window: symptoms <12 hours (can extend to 24h if ongoing symptoms/ECG changes)
Contraindications to fibrinolysis:
- Prior intracranial hemorrhage (absolute)
- Active bleeding (absolute)
- BP >180/110 unresponsive to treatment (relative)
- Recent surgery within 3 weeks (relative)
- NOT for NSTEMI or ST depression (UNLESS posterior MI suspected)
- NOT for patients presenting >24 hours after symptom onset who are now asymptomatic - Washington Manual of Medical Therapeutics
NSTEMI/Unstable Angina Protocol (2025 ACC/AHA & 2023 ESC Guidelines)
| Risk Level | Strategy | Timing |
|---|
| Immediate-risk (ongoing ischemia, hemodynamic instability, life-threatening arrhythmia) | Emergent invasive | <2 hours |
| High-risk (GRACE >140, dynamic ST/T changes, elevated troponin) | Early invasive | <24 hours |
| Intermediate-risk (GRACE 109-140, rising troponin) | Invasive | 24-72 hours |
| Low-risk (TIMI 0-1, negative troponin, no ECG changes) | Conservative / outpatient | Elective |
Key 2025 guideline update (ACC/AHA): P2Y12 inhibitor loading before coronary angiography is Class IA. The ESC 2023 de-escalated pre-angio P2Y12 loading to Class IIb based on ATLANTIC and SWEDEHEART data showing no mortality benefit in the acute phase.
Dual antiplatelet therapy (DAPT) = Aspirin + P2Y12 inhibitor (ticagrelor preferred over clopidogrel in most patients; prasugrel preferred in PCI if no prior stroke/TIA) for 12 months post-MI.
Prophylactic/Secondary Prevention Protocol (Post-MI)
| Drug | Target | Notes |
|---|
| Aspirin 75-100mg daily | Lifelong | Combined with P2Y12 for first 12 months |
| P2Y12 inhibitor | 12 months | Ticagrelor or clopidogrel |
| High-intensity statin | LDL <55 mg/dL (<1.4 mmol/L) | Atorvastatin 40-80mg or rosuvastatin 20-40mg |
| Beta-blocker | LV dysfunction (EF <40%) or arrhythmia | Indefinite if EF reduced |
| ACE inhibitor/ARB | EF <40%, HTN, DM, CKD | Consider all post-MI |
| Eplerenone/spironolactone (MRA) | EF <35% + DM or HF symptoms | After EPHESUS/RALES evidence |
| SGLT2 inhibitor | DM or HFrEF post-MI | Empagliflozin/dapagliflozin - new indication |
Quick Visual Summary
MI ECG SPECTRUM
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
STEMI → ST elevation in anatomic leads + reciprocals
Equivalents:
Wellens → Deep T inversions V2-V3 (LAD critical stenosis)
De Winter → Upsloping STD + hyperacute T (proximal LAD occlusion)
Posterior → Tall R + STD V1-V3 (check V7-V9)
aVR elev → ST ↑ aVR + diffuse STD (LM/proximal LAD)
NSTEMI → STD ± T inversions ± normal ECG
─ Key: Serial ECGs + hs-Troponin in ALL suspected ACS ─
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 247 - ECG Myocardial Ischemia
- Rosen's Emergency Medicine, 10th Ed - Chapter 64: Acute Coronary Syndromes
- Tintinalli's Emergency Medicine, Table 49-4 - ECG ST-Segment Criteria for AMI
- Goldman-Cecil Medicine, Chapter 57 - ACS Figure 57-1
- Washington Manual of Medical Therapeutics - ACS Reperfusion
- 2023 ESC Guidelines for Management of ACS
- 2025 ACC/AHA Guidelines for Acute Coronary Syndromes
- PMID 41663344 (De Winter + thrombolysis, 2026 systematic review)
- PMID 41798790 (aVR as high-risk NOMI, 2026 review)
- PMID 39546998 (RBBB in ACS, 2024 review)