Pancreatitis in detail point wise
Reading File
Finding Sources
Searching PubMed
"pancreatitis"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is the comprehensive, point-wise breakdown of pancreatitis from multiple authoritative medical textbooks:
PANCREATITIS - Detailed Point-Wise Notes
1. DEFINITION & OVERVIEW
- Pancreatitis = inflammation of the pancreas caused by autodigestion of pancreatic tissue by its own enzymes
- Divided into acute (reversible if underlying cause removed) and chronic (irreversible destruction of exocrine pancreas)
- Acute pancreatitis: annual incidence 33-74 per 100,000 globally; 5-35 per 100,000 in the Western world
- Overall mortality ~5% for acute pancreatitis; up to 30% in severe necrotizing cases
- Most common pancreatic disease worldwide; one of the top GI causes of hospitalization in the USA
2. ANATOMY RELEVANT TO PANCREATITIS
- Pancreas is a retroperitoneal organ with three segments: head, body, and tail
- Head sits within the C-loop of the duodenum; body passes posterior to the stomach; tail abuts the splenic hilum
- Main pancreatic duct (duct of Wirsung) meets the common bile duct to form the ampulla of Vater, draining into the duodenum via the sphincter of Oddi
- Exocrine function: secretion of digestive enzymes (trypsinogen, lipase, amylase, etc.)
- Endocrine function: insulin, glucagon, somatostatin secretion from islets of Langerhans
3. ETIOLOGY / CAUSES
Gallstones and alcohol = ~80% of all cases
Mechanical/Obstructive
- Gallstones impacting ampulla of Vater (40-70% of cases) - "gallstone pancreatitis"
- Post-ERCP (endoscopic retrograde cholangiopancreatography)
- Pancreatic cancer or periampullary neoplasms
- Pancreas divisum, annular pancreas
- Ampullary dysfunction or stenosis
- Duodenal diverticulum
- Biliary sludge / microlithiasis
- Trauma / perioperative injury
Toxic/Metabolic
- Chronic alcohol use (25-35% of cases)
- Hypertriglyceridemia (triglycerides >1000 mg/dL) - 5-10% of cases
- Hypercalcemia / hyperparathyroidism
- Uremia
- Drugs: azathioprine, thiazide diuretics, estrogens, anticonvulsants, cancer chemotherapeutic agents, many others
- Scorpion venom
Infectious
- Mumps virus (directly infects exocrine cells)
- Coxsackievirus
- Parasites: Ascaris lumbricoides, Clonorchis sinensis
Genetic
- PRSS1 mutations (cationic trypsinogen) - autosomal dominant hereditary pancreatitis
- SPINK1 mutations (trypsin inhibitor) - autosomal recessive
- CFTR mutations (symptoms restricted to pancreas)
- CTRC mutations
Vascular
- Shock, atheroembolism, polyarteritis nodosa
Autoimmune
- Type 1 (IgG4-related), Type 2
Idiopathic
- 10-20% of cases; many have occult microlithiasis or underlying genetic mutations
- Smoking and diabetes are independent risk factors
4. PATHOGENESIS (MECHANISM)
The central event: inappropriate intracellular activation of trypsinogen → trypsin → cascade of enzyme activation → autodigestion
Three Pathogenic Pathways (shown in diagram below):
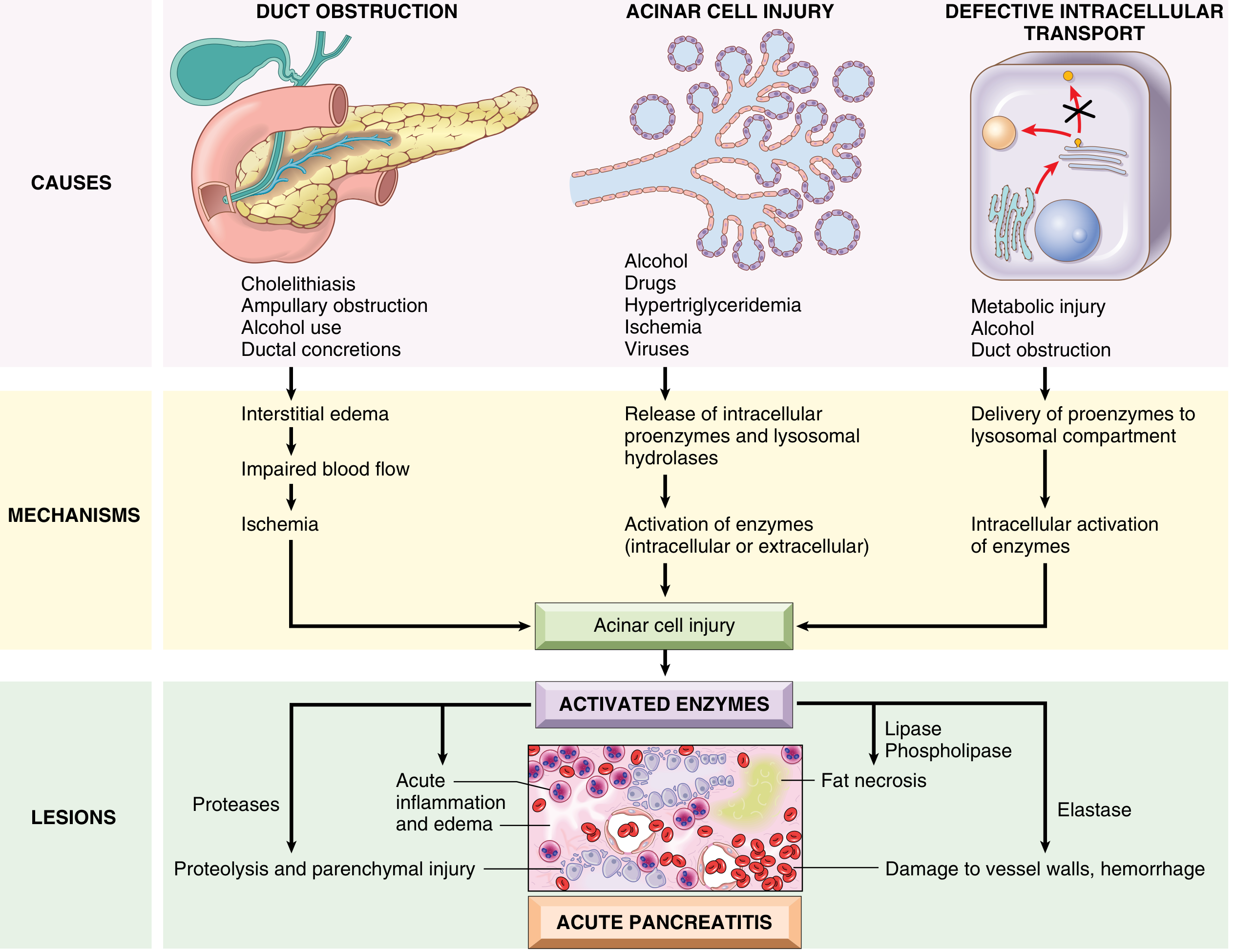
Pathway 1 - Pancreatic Duct Obstruction
- Gallstone/biliary sludge impaction → increased intraductal pressure → enzyme-rich fluid accumulates
- Lipase (secreted in active form) causes local fat necrosis
- Injured tissues + leukocytes release proinflammatory cytokines → interstitial edema → vascular insufficiency → acinar cell ischemia
Pathway 2 - Primary Acinar Cell Injury
- Mechanism in alcohol, hypertriglyceridemia, ischemia, viral infections, drugs
- Large triglyceride-rich chylomicrons retard capillary circulation → ischemic injury
- Injured cells release lipase → hydrolysis of triglycerides → toxic free fatty acids
Pathway 3 - Defective Intracellular Transport
- Normally, digestive enzymes (for secretion) and lysosomal hydrolases are transported in separate pathways
- In metabolic injury: proenzymes and lysosomal hydrolases get packaged together → proenzyme activation → lysosomal rupture → intracellular release of activated enzymes
Downstream Cascade:
- Activated trypsin converts prekallikrein → kallikrein (kinin system activation)
- Activates Factor XII (Hageman factor) → clotting + complement systems
- Proteases → proteolysis and parenchymal injury
- Lipase + phospholipase → fat necrosis
- Elastase → damage to vessel walls → hemorrhage
- Cytokine release → increased vascular permeability → edema, hemorrhage, necrosis
- Bacteremia from intestinal flora translocation
- SIRS, sepsis, shock in severe cases
Alcohol-specific mechanisms:
- Transient increase in pancreatic exocrine secretion + sphincter of Oddi contraction
- Direct toxic effects on acinar cells
- May alter enzyme activation, increase oxygen-derived free radicals
5. MORPHOLOGY / PATHOLOGY
Mild Acute Pancreatitis (Interstitial Edematous Pancreatitis)
- Interstitial edema
- Focal areas of fat necrosis in pancreas and peripancreatic fat
- Released fatty acids combine with calcium → insoluble calcium soaps precipitate in situ
Severe Acute Pancreatitis (Necrotizing Pancreatitis)
- Damage extends to acinar cells, ductal cells, islets of Langerhans, and blood vessels
- Macroscopically: red-black hemorrhagic areas interspersed with yellow-white chalky fat necrosis
- Fat necrosis can extend to omentum, mesentery, even subcutaneous fat
- Peritoneum contains serous, brown-tinged fluid with fat globules

Hemorrhagic Pancreatitis (Most Severe Form)
- Extensive parenchymal necrosis with diffuse hemorrhage within the gland
Basic Pathological Alterations:
- Microvascular leakage causing edema
- Necrosis of fat by lipases
- Acute inflammatory reaction
- Proteolytic destruction of pancreatic parenchyma and blood vessels → interstitial hemorrhage
6. CLINICAL FEATURES
Symptoms
- Abdominal pain - cardinal manifestation; persistent epigastric or left upper quadrant pain
- Radiation to the back, chest, or flanks
- Pain is constant, severe, not relieved by change of position but may be alleviated by sitting forward/bending
- Intensity of pain does NOT correlate with clinical severity
- Nausea, vomiting, anorexia (oral intake worsens pain)
Signs
- Vital signs: may be normal in mild disease; fever, tachycardia, tachypnea in severe disease
- Hypotension and shock signs in severe/complicated cases
- Jaundice - suggests obstructive etiology (gallstone/tumor)
- Cullen sign - bluish periumbilical discoloration (due to hemoperitoneum) - rare, poor prognosis
- Grey Turner sign - reddish-brown discoloration around flanks (retroperitoneal bleeding) - rare, poor prognosis
- Abdomen: normal or distended; epigastric tenderness with or without guarding
- Rebound tenderness - less common
- Absent or diminished bowel sounds (ileus)
- Murphy sign may be present in gallstone pancreatitis
Systemic Complications
- SIRS (Systemic Inflammatory Response Syndrome) - most important early complication
- ARDS - increased microvascular permeability; enzymatic degradation of surfactant
- Pleural effusions (up to 50% of patients; more commonly left-sided)
- Cardiovascular collapse - fluid shifts + volume loss
- Renal failure - hypoperfusion + inflammatory mediators
- Coagulopathy / DIC - cytokine-mediated activation of coagulation
- Hyperglycemia - decreased insulin production
- Hypocalcemia - low albumin and magnesium; calcium soap formation
Local Complications (Atlanta Classification 2012)
| Type | Complication | Timing |
|---|---|---|
| Interstitial Edematous | Acute peripancreatic fluid collection (homogeneous, no wall) | <4 weeks |
| Interstitial Edematous | Pancreatic pseudocyst (homogeneous, well-defined wall) | >4 weeks |
| Necrotizing | Acute necrotic collection (heterogeneous fluid + necrosis) | <4 weeks |
| Necrotizing | Walled-off necrosis (heterogeneous, well-defined wall) | >4 weeks |
Other local complications: bowel necrosis, splenic/portal vein thrombosis, GI bleeding, gastric outlet obstruction, pseudoaneurysm
7. DIAGNOSIS
Diagnostic Criteria (Atlanta Classification)
At least 2 of 3 criteria:
- Abdominal pain characteristic of acute pancreatitis
- Serum lipase or amylase >3x upper limit of normal
- Characteristic findings on abdominal imaging
Laboratory Tests
- Serum lipase - preferred test; greater sensitivity and specificity than amylase; also elevated in renal failure, appendicitis, cholecystitis
- Serum amylase - produced by pancreas AND salivary glands; less specific; may be falsely negative in alcohol/hypertriglyceridemia pancreatitis
- Neither enzyme elevation correlates with disease severity or prognosis
- Testing both enzymes does NOT improve diagnostic sensitivity
- ALT - specific for biliary pancreatitis (PPV 95% if elevated)
- AST, bilirubin - evaluate for obstructive etiology
- Serum calcium - rule out hypercalcemia as cause; monitor for hypocalcemia
- Triglyceride levels - if no gallstones/alcohol history
- CBC - evaluate SIRS
- BMP/BUN/creatinine - organ failure assessment
Imaging
Ultrasound (US)
- First-line; best for gallbladder and biliary tract
- Limited for direct pancreatic visualization (bowel gas interference)
- Can identify gallstones as etiology
CT Scan (with IV contrast)
- NOT routinely recommended at first presentation
- Indicated when: (1) diagnostic uncertainty, (2) rule out other pathology, (3) no response to treatment after 48-72 hours
- Best performed 3-7 days after symptom onset (necrosis may not be evident earlier)
- Sensitivity/specificity >90% for acute pancreatitis
- Findings: pancreatic enlargement, loss of texture/borders, peripancreatic fat stranding, areas of non-enhancement (necrosis)
- CT is normal in 15-30% of mild cases
MRI/MRCP
- Similar diagnostic utility to CT
- Superior for gallbladder/biliary tract imaging
- Preferred when contrast contraindicated or for choledocholithiasis
Plain films - may show ileus pattern, "sentinel loop" of dilated small bowel in left upper quadrant
8. SEVERITY SCORING SYSTEMS
Ranson Criteria
At admission:
- Age >55 years
- WBC >16,000/mm³
- Glucose >200 mg/dL
- AST >250 IU/L
- LDH >350 IU/L
At 48 hours:
- Hematocrit drop >10%
- BUN rise >5 mg/dL
- Calcium <8 mg/dL
- PaO₂ <60 mmHg
- Base deficit >4 mEq/L
- Fluid needs >6 L
(Biliary pancreatitis uses slightly modified thresholds: Age >70, WBC >18,000, Glucose >220, LDH >400)
Score: 0-2 = mild; 3-4 = moderate; 5-6 = severe; >6 = very severe
BISAP Score (simpler, ED-friendly)
- BUN >25 mg/dL
- Impaired mental status (disorientation, lethargy, somnolence, coma)
- SIRS criteria present
- Age >60 years
- Pleural effusion present
Score ≥3 = severe disease
APACHE II - Uses 12 physiological variables (temperature, MAP, HR, RR, PaO₂, pH, sodium, potassium, creatinine, hematocrit, WBC, Glasgow Coma Scale) + age + chronic health problems
Modified CT Severity Index (CTSI)
- Pancreatic inflammation score (0-4) + necrosis score (0-4) + extrapancreatic complications (+2)
- Total 0-10; higher = more severe
9. DIFFERENTIAL DIAGNOSIS
Abdominal:
- Peptic ulcer disease / perforated peptic ulcer
- Cholecystitis / cholelithiasis / cholangitis / choledocholithiasis
- Gastritis, gastroenteritis
- Mesenteric ischemia / bowel obstruction
- Abdominal aortic aneurysm
- Nephrolithiasis
- Ectopic pregnancy
Cardiopulmonary:
- Myocardial infarction (lower thoracic/upper abdominal pain)
- Pneumonia, pericarditis, pleural effusion
Systemic:
- Sickle cell crisis
- Diabetic ketoacidosis
10. MANAGEMENT OF ACUTE PANCREATITIS
Initial/General
- Hospitalization; most cases (80%) are mild and self-limiting
- NPO initially; advance diet as tolerated
Fluid Resuscitation
- Aggressive IV hydration is a mainstay of treatment
- Correct hypovolemia from third-spacing and vomiting
- Lactated Ringer's preferred over normal saline (lower risk of hyperchloremic acidosis)
Pain Management
- IV opioid analgesics as needed
- Pain control does not worsen clinical outcomes
Nutrition (Major paradigm shift)
- Old practice: NPO to avoid stimulating pancreatic secretion
- Current evidence: Early enteral nutrition (EN) initiated within 24-36 hours
- Benefits of early EN: lower risk of multi-organ failure, operative interventions, systemic infections, septic complications, mortality
- If ICU admission (severe SIRS): nasogastric (NG) or nasojejunal (NJ) tube + EN within 24-36 hours
- If mild SIRS on wards: offer oral diet as tolerated; start EN only if diet fails after 4 days
- Gastric vs. jejunal feeding: no significant difference in outcome in severe AP
- Enteral vs. parenteral (PN): EN significantly reduces risk of infected peripancreatic necrosis (OR 0.28), single organ failure (OR 0.25), MOF (OR 0.41), and death (~2.5x reduction)
- Caution: EN in hemodynamically unstable patients requiring inotropes risks non-occlusive mesenteric ischemia
Antibiotics
- NOT routinely indicated in acute pancreatitis
- Reserved for confirmed infected necrosis or other documented infection
- Prophylactic antibiotics do not reduce mortality in sterile necrosis
ERCP
- Indicated urgently in acute biliary pancreatitis with concurrent cholangitis or persistent biliary obstruction
- Cholecystectomy should be performed after resolution (same admission for mild cases)
ICU / Organ Support
- ICU admission for severe cases: SIRS, organ failure
- Mechanical ventilation, vasopressors, renal replacement therapy as needed
Surgical/Interventional
- Reserved for infected pancreatic necrosis - typically via step-up approach:
- Percutaneous/endoscopic drainage first
- Video-assisted retroperitoneal debridement (VARD) or surgical necrosectomy if above fails
- Pseudocyst drainage (if symptomatic/complicated): endoscopic, radiologic, or surgical
11. CHRONIC PANCREATITIS
Definition
- Long-standing inflammation causing irreversible destruction of the exocrine pancreas, eventually also the islets of Langerhans
- Recurrent bouts of acute pancreatitis can evolve into chronic pancreatitis
- Prevalence: 0.04-5% of US population; 9-62 per 100,000 globally
Most Common Causes (TIGAR-O Classification)
- Toxic-metabolic: Chronic alcohol use (most common)
- Idiopathic: 40% of cases; many have CFTR/PRSS1/SPINK1 mutations
- Genetic: PRSS1, SPINK1, CFTR, CTRC mutations
- Autoimmune: Type 1 (IgG4-related, responds to steroids), Type 2
- Recurrent and severe acute pancreatitis
- Obstructive: Pancreas divisum, sphincter of Oddi disorders, malignant obstruction
Morphology
- Gross: Hard gland, dilated ducts, visible calcific concretions
- Microscopic: Parenchymal fibrosis, reduced/absent acini, dilated ducts, chronic inflammatory infiltrate, ductal epithelial changes (atrophy/hyperplasia/squamous metaplasia)
- Islets of Langerhans initially relatively spared, eventually destroyed
- Autoimmune pancreatitis: striking lymphocyte/plasma cell infiltration, IgG4+ cells, "swirling" fibrosis, venulitis ("lymphocytic sclerosing pancreatitis")
Clinical Features
- Severe postprandial epigastric pain radiating to the back; sitting forward helps
- Associated nausea and vomiting
- Exocrine insufficiency: steatorrhea, weight loss, malnutrition, malabsorption
- Endocrine insufficiency: Type 3c diabetes; increased risk of hypoglycemia (loss of counterregulatory glucagon)
- Jaundice (biliary obstruction or alcoholic cirrhosis)
- Palpable mass (pseudocyst or tumor)
- Weight loss from hypermetabolism + malabsorption + pain-related food avoidance
Complications of Chronic Pancreatitis
- Pancreatic pseudocysts
- Pancreatic ascites
- Ductal strictures
- Duodenal stenosis
- Pleural effusions
- Pseudoaneurysms (splenic, hepatic, gastroduodenal, pancreaticoduodenal arteries)
- Portal and splenic vein thrombosis
- Increased risk of pancreatic adenocarcinoma
Diagnosis
- Serum lipase/amylase: may be normal (less helpful than in acute)
- CT (imaging of choice): Intraductal pancreatic calcifications are the most specific finding; duct dilation, parenchymal atrophy, pseudocysts
- US can show calcifications and ductal dilation
- MRCP: superior for ductal anatomy
Management
- Pain: analgesics (stepwise from NSAIDs to opioids); pancreatic enzyme supplementation (reduces enzyme secretion via negative feedback); celiac plexus block; surgical drainage
- Exocrine insufficiency: pancreatic enzyme replacement therapy (PERT) with meals
- Endocrine insufficiency: diabetes management; insulin therapy
- Nutrition: jejunal feeding to improve weight; reduce abdominal pain
- Antioxidants: selenium, ascorbic acid, β-carotene, α-tocopherol, methionine - may provide pain relief (evidence conflicting)
- Autoimmune pancreatitis: anti-B cell therapy + corticosteroids (responds well)
- Endoscopic: ERCP for ductal strictures, stone removal, stenting
- Surgical: pancreaticojejunostomy (Puestow procedure), Whipple's procedure, distal pancreatectomy for refractory cases
12. PANCREATIC PSEUDOCYST
- Collection of fluid that may be intra- or extrapancreatic, arising weeks after acute pancreatitis
- Walled off by inflammatory and fibrous tissue; lacks an epithelial lining (hence "pseudo")
- Contents: rich in pancreatic enzymes (amylase, lipase)
- Usually solitary; common in lesser omental sac or retroperitoneum between stomach and transverse colon
- Size: 2-30 cm
- Account for ~75% of all pancreatic cysts
- Most resolve spontaneously
- Complications if persistent: infection, compression/obstruction of adjacent structures, rupture, hemorrhage
13. PANCREATITIS IN CHILDREN (Pediatric Points)
- Uncommon especially in those <10 years old
- Common causes in children: trauma, infections, structural anomalies, systemic disease, drugs/toxins
- Idiopathic: 30% of cases
- Biliary disease should be considered in adolescents/teenagers
- Sentinel loop on plain film is a common finding
- Management: similar to adults; NPO initially, analgesics, IV fluids
14. KEY POINTS SUMMARY TABLE
| Feature | Acute Pancreatitis | Chronic Pancreatitis |
|---|---|---|
| Reversibility | Reversible | Irreversible |
| Common causes | Gallstones (40-70%), Alcohol (25-35%) | Alcohol (most common), genetic, autoimmune |
| Key enzyme | Lipase preferred >3x ULN | May be normal |
| Pain | Severe, acute onset | Recurrent, postprandial |
| Key complication | MOF, SIRS, infected necrosis | Exocrine/endocrine insufficiency, pseudocyst |
| Imaging | CT with contrast (if indicated) | CT - calcifications most specific |
| Nutrition | Early EN within 24-36h | Enzyme replacement, jejunal feeding |
| Surgery | Step-up approach for infected necrosis | Drainage procedures, Whipple's |
Sources:
- Robbins & Kumar Basic Pathology
- Rosen's Emergency Medicine (9th/current edition)
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease
- Rosen's Emergency Medicine (Pediatric section)
In short but cover all points
PANCREATITIS - Concise Complete Notes
1. DEFINITION
- Inflammation of the pancreas caused by autodigestion by its own enzymes
- Two forms: Acute (reversible) and Chronic (irreversible)
2. CAUSES (ETIOLOGY)
Gallstones + Alcohol = ~80% of cases
| Category | Examples |
|---|---|
| Mechanical | Gallstones (40-70%), post-ERCP, trauma, pancreas divisum |
| Toxic/Metabolic | Alcohol (25-35%), hypertriglyceridemia (>1000 mg/dL), hypercalcemia, drugs (thiazides, azathioprine, estrogens) |
| Infectious | Mumps, coxsackievirus, Ascaris, Clonorchis |
| Genetic | PRSS1, SPINK1, CFTR, CTRC mutations |
| Vascular | Shock, polyarteritis nodosa |
| Autoimmune | Type 1 (IgG4), Type 2 |
| Idiopathic | 10-20% of cases |
3. PATHOGENESIS
Key event: Inappropriate activation of trypsinogen → trypsin → cascade
Three pathways:
- Duct obstruction → increased intraductal pressure → enzyme accumulation → edema → ischemia
- Acinar cell injury → direct toxic damage (alcohol, drugs, viruses) → intracellular enzyme release
- Defective intracellular transport → proenzymes + lysosomal hydrolases packaged together → intracellular activation
Downstream:
- Proteases → parenchymal destruction
- Lipase/phospholipase → fat necrosis (chalk-white deposits = calcium soaps)
- Elastase → vessel wall damage → hemorrhage
- Cytokines → SIRS → MOF
4. MORPHOLOGY / PATHOLOGY
| Form | Gross / Micro Features |
|---|---|
| Mild (interstitial edematous) | Edema, focal fat necrosis only |
| Severe (necrotizing) | Red-black hemorrhagic + yellow-white chalky fat necrosis areas |
| Hemorrhagic (worst) | Diffuse hemorrhage throughout gland |
- Fat necrosis can extend to omentum, mesentery, subcutaneous fat
- 4 basic changes: microvascular leakage, fat necrosis, acute inflammation, proteolytic parenchymal destruction
5. CLINICAL FEATURES
Symptoms:
- Severe constant epigastric pain radiating to the back
- Relieved by leaning forward
- Nausea, vomiting, anorexia
- Pain intensity does NOT correlate with severity
Signs:
- Fever, tachycardia, hypotension (severe cases)
- Jaundice → obstructive etiology
- Cullen sign - periumbilical bruising (hemoperitoneum) - rare, poor prognosis
- Grey Turner sign - flank bruising (retroperitoneal bleed) - rare, poor prognosis
- Epigastric tenderness ± guarding
- Absent bowel sounds (ileus)
Systemic Complications (SIRS → MOF):
- ARDS (left-sided pleural effusion in 50%)
- Cardiovascular collapse / shock
- Renal failure
- DIC / coagulopathy
- Hyperglycemia, hypocalcemia
Local Complications (Atlanta 2012):
| Type | <4 weeks | >4 weeks |
|---|---|---|
| Interstitial | Acute peripancreatic fluid collection | Pseudocyst |
| Necrotizing | Acute necrotic collection | Walled-off necrosis |
6. DIAGNOSIS
Criteria (Atlanta) - 2 of 3:
- Characteristic abdominal pain
- Lipase or amylase >3× upper limit of normal
- Imaging findings
Labs:
- Lipase - preferred (more sensitive/specific than amylase)
- Amylase - less specific; falsely negative in alcohol/hypertriglyceridemia cases
- Elevation level does NOT predict severity
- ALT: PPV 95% for biliary pancreatitis
- CBC, BMP, triglycerides, calcium
Imaging:
- US - first-line; best for gallstones; limited for pancreas
- CT (IV contrast) - NOT routine; use at 48-72h if no improvement; >90% sensitivity; shows fat stranding, non-enhancement (necrosis)
- MRI/MRCP - best for biliary anatomy; preferred if contrast contraindicated
- Plain film - sentinel loop (dilated small bowel in LUQ)
7. SEVERITY SCORING
| Score | Components | Severe if |
|---|---|---|
| Ranson | 5 at admission + 6 at 48h | ≥3 |
| BISAP | BUN >25, impaired mentation, SIRS, Age >60, Pleural effusion | ≥3 |
| APACHE II | 12 physiological variables + age + chronic disease | >8 |
| Modified CTSI | CT inflammation (0-4) + necrosis (0-4) + extrapancreatic (+2) | >4 |
8. MANAGEMENT - ACUTE
| Aspect | Action |
|---|---|
| Fluids | Aggressive IV resuscitation; Lactated Ringer's preferred |
| Pain | IV opioid analgesics |
| Nutrition | Early EN within 24-36h; NG/NJ tube if ICU-level SIRS; oral diet if mild |
| Antibiotics | NOT routine; only for confirmed infected necrosis |
| ERCP | Urgent if biliary pancreatitis + cholangitis or obstruction |
| Cholecystectomy | Same admission (mild); after recovery (severe) |
| Surgery | Step-up: drainage first → necrosectomy if needed (only for infected necrosis) |
EN vs PN: EN reduces infected necrosis (OR 0.28), organ failure (OR 0.25), MOF (OR 0.41), death (2.5× reduction)
9. CHRONIC PANCREATITIS
Definition: Irreversible exocrine (eventually endocrine) destruction with fibrosis
Causes (TIGAR-O): Toxic-metabolic (alcohol #1), Idiopathic (40%), Genetic, Autoimmune, Recurrent acute, Obstructive
Morphology: Hard gland, dilated ducts, calcific concretions, parenchymal fibrosis, acinar loss, islets initially spared
Clinical:
- Recurrent postprandial epigastric pain → back radiation
- Exocrine insufficiency: steatorrhea, malabsorption, weight loss
- Endocrine insufficiency: Type 3c diabetes + hypoglycemia risk
- Jaundice if biliary obstruction
Diagnosis:
- CT: intraductal calcifications (most specific), ductal dilation, atrophy
- Lipase/amylase may be normal
- MRCP for ductal anatomy
Complications: Pseudocysts, ductal strictures, pancreatic ascites, duodenal stenosis, pseudoaneurysms, portal/splenic vein thrombosis, pancreatic adenocarcinoma risk
Management:
- Pain: analgesics, enzyme supplements, celiac plexus block, surgery
- PERT (pancreatic enzyme replacement) for exocrine insufficiency
- Insulin for diabetes
- Jejunal feeding for nutrition
- Autoimmune type: steroids + anti-B cell therapy (responds well)
- Endoscopic: stricture dilation, stone extraction, stenting
- Surgical: Puestow procedure, Whipple's, distal pancreatectomy
10. PSEUDOCYST
- Fluid collection walled off by fibrous/inflammatory tissue; no epithelial lining
- Arises weeks after acute pancreatitis; rich in enzymes
- ~75% of all pancreatic cysts; most resolve spontaneously
- Complications: infection, compression, rupture, hemorrhage
- Treatment if symptomatic: endoscopic, radiologic, or surgical drainage
11. SPECIAL NOTES
- Autoimmune pancreatitis (IgG4): IgG4+ plasma cells, "swirling" fibrosis, venulitis; responds to steroids
- Hereditary pancreatitis: PRSS1 mutation → trypsin can't self-inactivate → hyperactivation
- Pediatric pancreatitis: trauma, infections, structural anomalies > gallstones/alcohol
- Scorpion envenomation: causes pancreatitis in tropical regions
- Smoking + diabetes = independent risk factors
Sources: Robbins & Kumar Basic Pathology | Rosen's Emergency Medicine | Sleisenger & Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.