pulsatile pain behind the last molar or wisdom teeth
Reading File
Finding Sources
Finding Sources
Searching PubMed
pericoronitis third molar treatment
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough clinical breakdown of pulsatile (throbbing) pain behind the last molar / wisdom tooth area, drawn from Rosen's Emergency Medicine, Scott-Brown's Otorhinolaryngology, Tintinalli's Emergency Medicine, and Harrison's Internal Medicine.
Pulsatile/Throbbing Pain Behind the Last Molar (Wisdom Tooth Area)
Most Likely Diagnosis: Pericoronitis
The #1 cause of throbbing pain behind the last molar is pericoronitis - inflammation of the operculum (the flap of gum tissue overlying a partially erupted or impacted wisdom tooth).
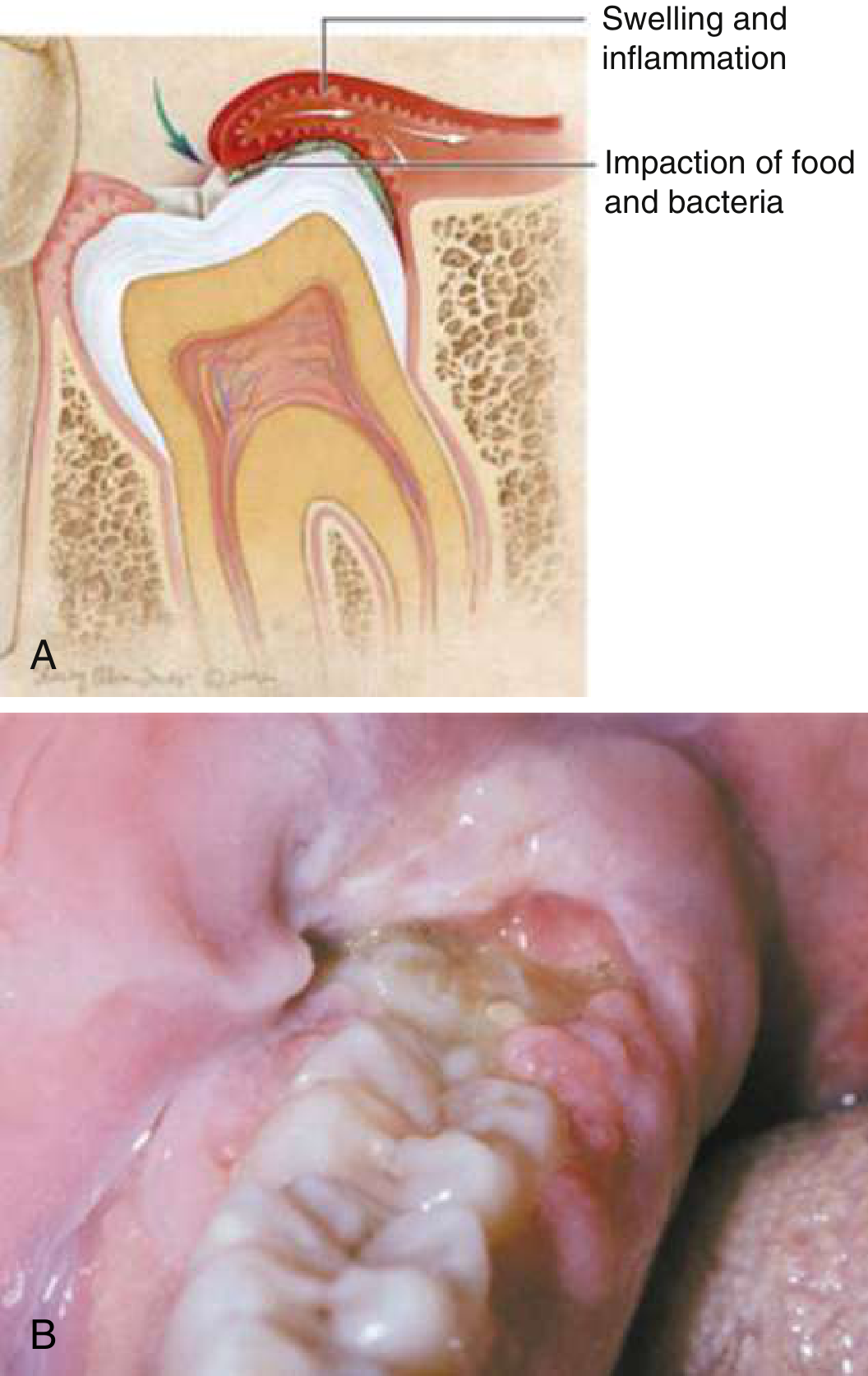
Pathophysiology: As the third molar partially erupts, food debris and bacteria accumulate under the operculum. This triggers a severe localized inflammatory response, producing the classic pulsatile/throbbing pain. The inflammatory pressure buildup accounts for the pulsatile quality of pain.
Classic features (from Scott-Brown's Otorhinolaryngology, p. 702 and Rosen's):
- Throbbing pain aggravated by jaw movement and chewing (mastication)
- Inflamed, red, swollen operculum visible behind the last visible molar
- Trismus (reduced mouth opening)
- Halitosis
- Localized facial swelling
- Regional lymphadenopathy (tender lymph nodes under the jaw)
- Typically occurs in the 2nd or 3rd decade of life
- More common with impacted or malerupted third molars
Differential Diagnosis: Other Causes of Throbbing Pain in This Area
The table below comes directly from Tintinalli's Emergency Medicine:
| Category | Conditions to Consider |
|---|---|
| Odontogenic (most common) | Pericoronitis, irreversible pulpitis, periapical abscess, periradicular periodontitis |
| Periodontal | Periodontal abscess, acute necrotizing gingivostomatitis |
| Neurogenic | Trigeminal neuralgia, temporomandibular disorder (TMD) |
| Nondental infection | Sinusitis (referred pain), parotitis, sialadenitis |
| Serious/rare | Osteonecrosis, squamous cell carcinoma, leukemia |
Key differential features:
Irreversible pulpitis / dental abscess: A carious (decayed) wisdom tooth can develop pulp infection. Pain starts as cold/heat-triggered and evolves into a dull, throbbing, spontaneous pain that is poorly localized. Harrison's (22nd ed.) notes it can have a "sharp or throbbing visceral quality." Tenderness on tapping the tooth (percussion sensitivity) suggests apical periodontitis.
Periapical abscess: Further spread of pulp infection creates visible swelling, erythema, and pus around the tooth apex. The throbbing is usually more intense and constant.
Periodontal abscess: Infection of the gum pocket alongside the tooth; presents with localized throbbing, gum swelling, and may have pus on probing.
Red Flags - When to Worry (Serious Complications)
Because the wisdom tooth sits adjacent to the masticator space (masseteric, pterygomandibular, and temporalis spaces), infection can spread rapidly:
- Trismus (cannot open mouth) - suggests spread to masticator space
- Dysphagia or difficulty breathing - suggests parapharyngeal or retropharyngeal spread - this is life-threatening
- High fever, neck swelling - suggests deep space infection (Ludwig's angina)
- Inability to swallow - emergency referral required
Treatment Summary
| Severity | Treatment |
|---|---|
| Mild pericoronitis | Irrigation under the operculum with chlorhexidine 0.2%; warm saline rinses; NSAIDs (ibuprofen 400-600 mg q6-8h) or acetaminophen 650 mg q6h |
| Moderate (with trismus/lymphadenopathy) | Add systemic antibiotics (see below) |
| Severe/spreading infection | IV antibiotics + urgent surgical consult |
| Definitive | Dental referral for wisdom tooth extraction or excision of the operculum |
Antibiotic choices (from Rosen's Emergency Medicine):
| Antibiotic | Dose | Duration |
|---|---|---|
| Penicillin V | 500 mg PO tid-qid | 10 days |
| Amoxicillin/clavulanate | 500/125 mg PO tid | 10 days |
| Metronidazole | 500 mg PO bid | 10 days (penicillin allergy; also targets gram-negative anaerobes which predominate in pericoronitis) |
| Clindamycin | 300 mg PO qid | 10 days (penicillin allergy) |
Note: Gram-negative anaerobes predominate in pericoronitis, which is why metronidazole is frequently chosen. Systemic antibiotics are not needed for mild, uncomplicated pericoronitis without fever or lymphadenopathy.
Bottom Line
Pulsatile pain behind the last molar is pericoronitis until proven otherwise - especially in a young adult (teens to 30s) with a partially erupted or impacted wisdom tooth. The immediate steps are: chlorhexidine irrigation under the gum flap, NSAIDs for pain, and prompt dental referral for extraction or operculectomy. If fever, trismus, or neck swelling are present, treat as a potential deep-space infection and escalate care urgently.
- Rosen's Emergency Medicine, 9th ed., Ch. 56
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1, Ch. 42
- Tintinalli's Emergency Medicine, 9th ed., Ch. 245
- Harrison's Principles of Internal Medicine, 22nd ed.
This is a shared conversation. Sign in to Orris to start your own chat.