Top 10 ecg changes with pictures
Reading File
Finding Sources
Searching Images
ECG electrocardiogram changes patterns STEMI ST elevation
Finding Sources
Searching Images
atrial fibrillation ECG heart block bundle branch block
Searching Images
hyperkalemia peaked T waves ECG ventricular tachycardia
Searching Images
Wolff-Parkinson-White WPW delta wave PR interval short ECG long QT torsades de pointes
Searching Images
long QT interval torsades de pointes ECG pericarditis diffuse ST elevation saddle
Searching Images
left ventricular hypertrophy ECG voltage criteria complete heart block third degree
I now have excellent ECG images. Let me compile the top 10 ECG changes with the best representative images from the searches.
Top 10 ECG Changes (with Images)
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
Key Features: ST elevation ≥1 mm in ≥2 contiguous leads, reciprocal ST depression, hyperacute T-waves, Q-wave development, tombstone morphology.
Lead patterns by territory:
- Inferior STEMI (RCA/LCx): elevation in II, III, aVF + reciprocal depression in I, aVL
- Anterior STEMI (LAD): elevation in V1–V4
- Lateral STEMI: elevation in I, aVL, V5–V6
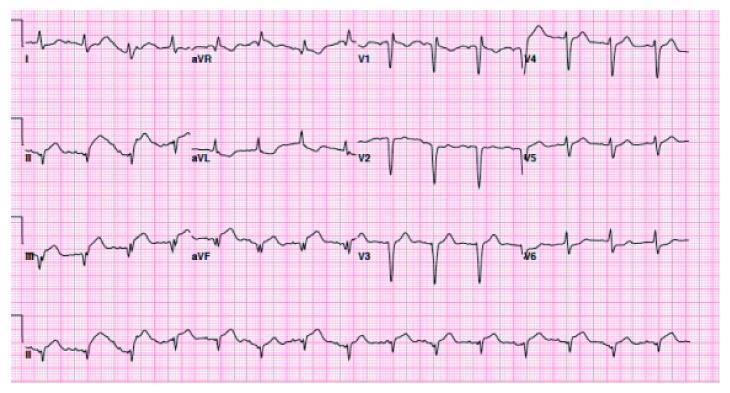
Inferior STEMI (RCA occlusion):
Anterolateral STEMI (LAD occlusion):
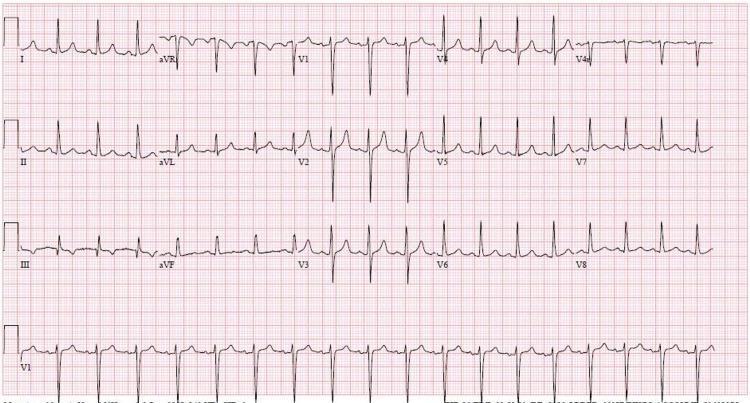
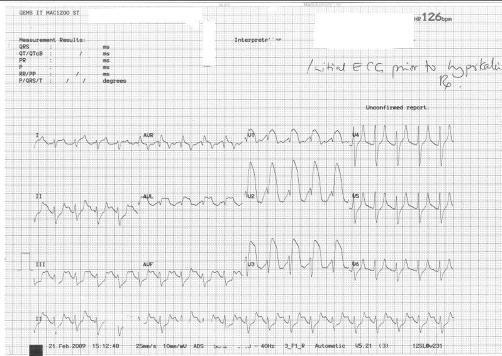
2. 🔥 Hyperkalemia
Key Features (progressive with rising K⁺):
- Peaked, narrow-based (tented) T-waves — first sign
- Prolonged PR interval, widening QRS
- Loss of P-waves (sinoventricular rhythm)
- Sine-wave pattern → ventricular fibrillation
Early hyperkalemia — peaked T-waves:
Severe hyperkalemia — wide QRS, sine-wave, absent P-waves:
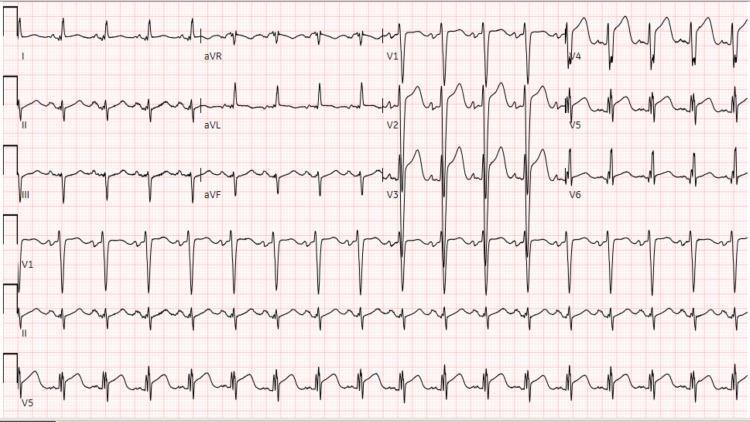
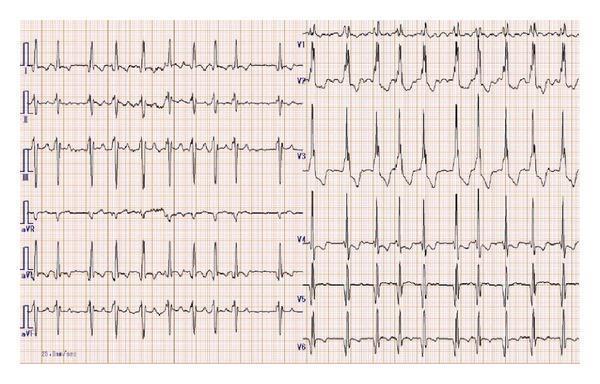
3. 💙 Atrial Fibrillation (AF)
Key Features:
- Irregularly irregular rhythm — no two R-R intervals equal
- Absent P-waves, replaced by fibrillatory (f) waves (best seen in V1)
- Narrow QRS (unless aberrant conduction/BBB)
- Ventricular rate variable (controlled: 60–100; rapid response: >100)
AF with Right Bundle Branch Block (RBBB):
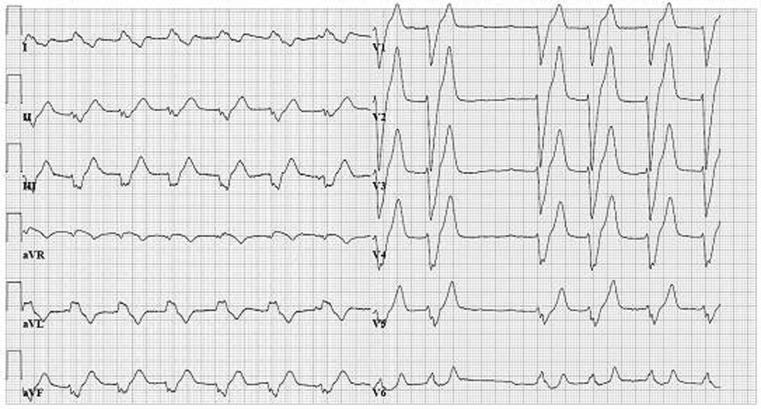
4. 🔵 Left Bundle Branch Block (LBBB)
Key Features (WiLLiaM — W in V1, M in V5/V6):
- QRS duration >120 ms
- Broad, notched R in I, aVL, V5–V6 (M pattern)
- Deep QS in V1–V3 (W pattern)
- Discordant ST-T changes (ST/T opposite to QRS)
- New LBBB + chest pain = treat as STEMI equivalent (Sgarbossa criteria)
AF with LBBB:
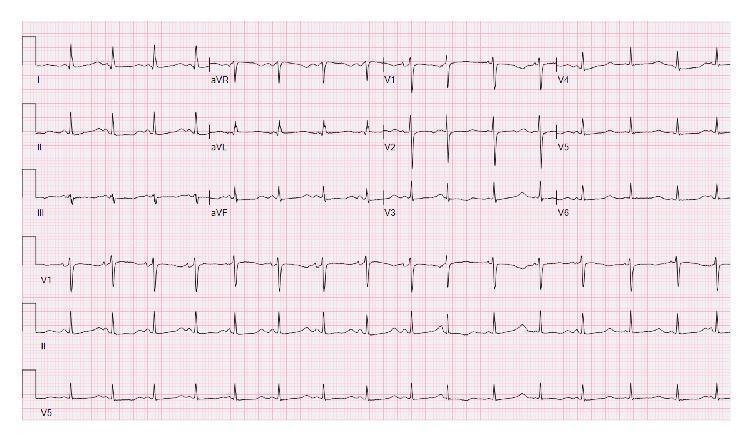
5. 🟠 Right Bundle Branch Block (RBBB)
Key Features (MaRRoW — M in V1, W in V5/V6):
- QRS duration >120 ms
- rsR' ("M" shape) or RSR' in V1–V2
- Broad, slurred S-wave in I, aVL, V5–V6 (W pattern)
- T-wave inversion in V1–V3 (normal secondary change)
AF with RBBB:
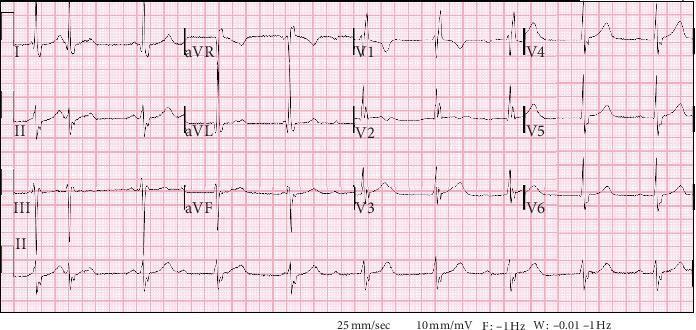
6. ⚡ Wolff-Parkinson-White (WPW) Syndrome
Key Features (Pre-excitation triad):
- Short PR interval (<120 ms)
- Delta wave (slurred upstroke of QRS)
- Widened QRS (>120 ms)
- Secondary ST-T changes
- Risk: AF with rapid conduction → ventricular fibrillation (avoid AV nodal blockers!)
Classic WPW pattern:

WPW with pseudoinfarction pattern (negative delta waves inferior leads):

7. ⏱️ Long QT Syndrome / Torsades de Pointes
Key Features:
- QTc >440 ms (men), >460 ms (women) — clinically significant >500 ms
- T-wave broad and prominent
- T-wave alternans = high-risk sign
- Torsades de Pointes: twisting polymorphic VT around isoelectric line, triggered by R-on-T
Causes: Electrolyte disturbances (↓K⁺, ↓Mg²⁺, ↓Ca²⁺), drugs (quinidine, sotalol, haloperidol, macrolides, methadone), congenital LQTS
Prolonged QTc (QTc 632 ms):
Torsades de Pointes initiation (short-long-short sequence + R-on-T):

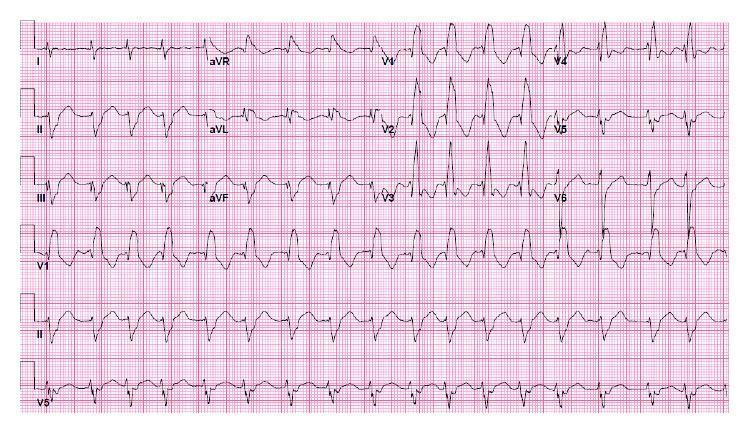
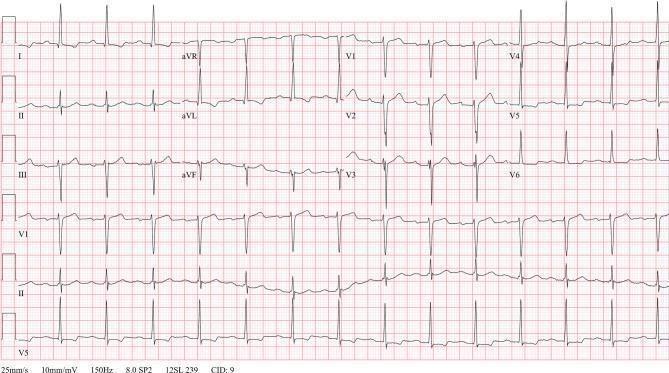
8. 🫁 Left Ventricular Hypertrophy (LVH)
Key Features:
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥35 mm (or R in aVL ≥11 mm)
- Cornell criteria: R in aVL + S in V3 >28 mm (men) or >20 mm (women)
- LV strain pattern: ST depression + asymmetric T-wave inversion in I, aVL, V5–V6
- Left axis deviation
- Associated with hypertension, aortic stenosis, HOCM
LVH with strain pattern + first-degree AV block:
9. 🚨 Complete (Third-Degree) AV Block
Key Features:
- Complete AV dissociation — P-waves and QRS complexes occur independently
- Atrial rate faster than ventricular rate
- Escape rhythm: narrow QRS = junctional escape (~40–60 bpm); wide QRS = ventricular escape (~20–40 bpm)
- Causes: inferior MI (usually transient), Lyme disease, medications, degenerative disease
Complete AV block with ventricular escape:
10. ❤️🔥 Inferolateral STEMI (Extensive / Wraparound LAD)
Key Features: ST elevation in both inferior (II, III, aVF) AND lateral (V4–V6) leads — characteristic of either a "wraparound" distal LAD or simultaneous RCA + LCx territory involvement.
Inferolateral STEMI — extensive territory:

Quick Reference Table
| # | ECG Change | Key Finding | Clinical Pearl |
|---|---|---|---|
| 1 | Anterior STEMI | ST↑ V1–V4 | LAD occlusion; cath-lab activation |
| 2 | Inferior STEMI | ST↑ II, III, aVF | Check right-sided leads for RV infarct |
| 3 | Hyperkalemia | Peaked T → wide QRS → sine wave | Emergent calcium gluconate |
| 4 | Atrial Fibrillation | Irregularly irregular, no P-waves | Rate vs. rhythm control decision |
| 5 | LBBB | Wide QRS, W in V1, M in V5-V6 | New LBBB + pain = STEMI equivalent |
| 6 | RBBB | rsR' in V1, slurred S in V5-V6 | May indicate acute PE if new |
| 7 | WPW | Short PR, delta wave | Avoid adenosine/digoxin in AF-WPW |
| 8 | Long QT/TdP | QTc >500 ms, twisting VT | IV magnesium sulfate for TdP |
| 9 | LVH | High voltage + strain pattern | Hypertension/valvular disease marker |
| 10 | Complete AV Block | AV dissociation, escape rhythm | Urgent pacing if hemodynamically unstable |
This is a shared conversation. Sign in to Orris to start your own chat.