Mi
It looks like your message got cut off! Could you finish your thought? What would you like help with?
Myocardial infaction
Asking for Preferences
Reading File
Finding Sources
Searching PubMed
"myocardial infarction"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive, authoritative content. Let me compile the full answer.
Myocardial Infarction: Clinical Presentation & Diagnosis
The ACS Spectrum
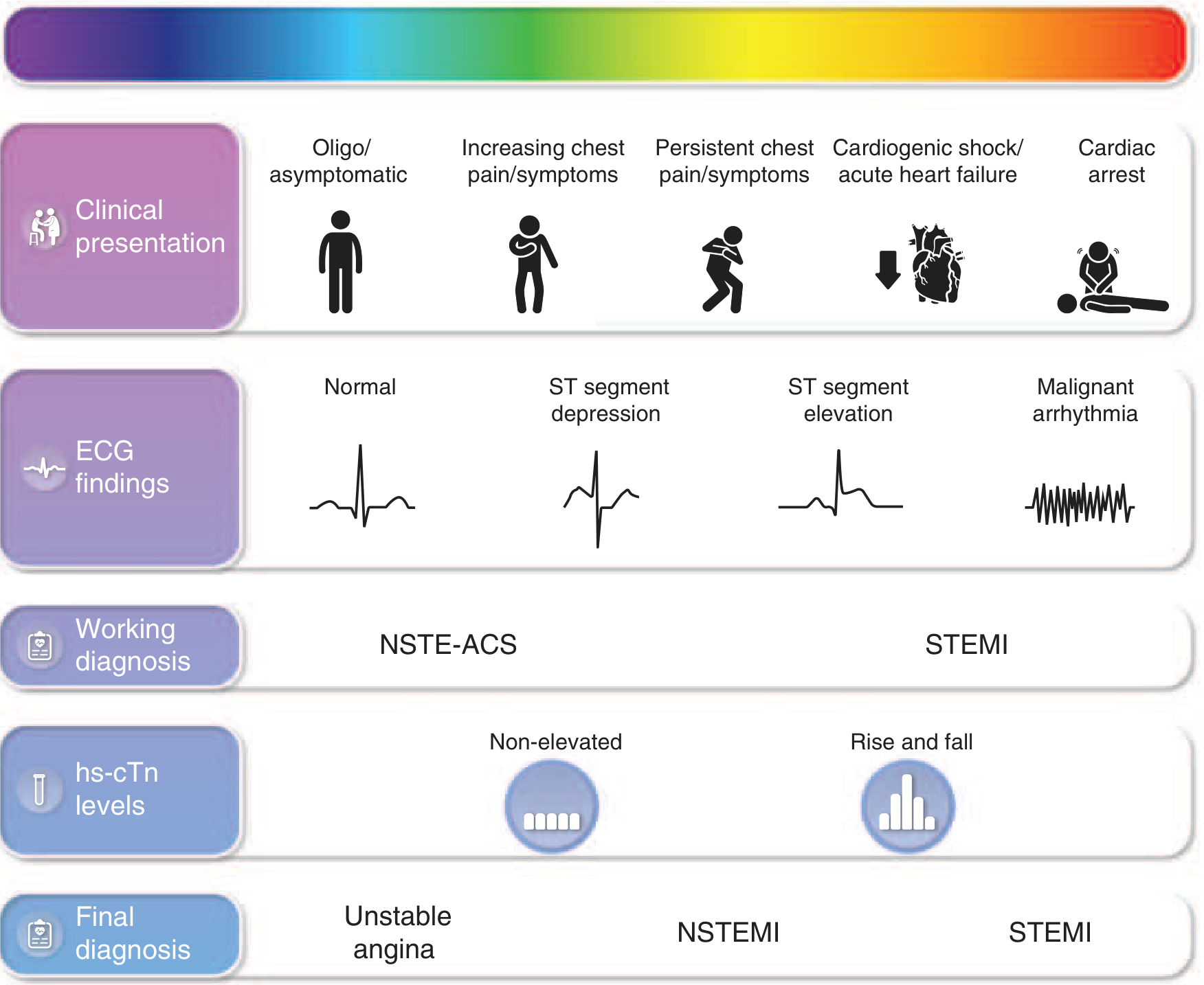
MI exists along a continuum with unstable angina (UA). The key distinction:
- UA: ischemic chest pain at rest/minimal exertion, no biomarker elevation
- NSTEMI: same presentation + elevated troponin, no ST elevation on ECG
- STEMI: ischemic symptoms + persistent ST elevation on ECG → total coronary occlusion by fresh thrombus
Clinical Presentation
Symptoms
Chest discomfort is typically substernal, and must have ≥1 of:
- Occurs at rest or with minimal exertion, lasting >10 minutes
- New onset within the prior 2 weeks
- Crescendo pattern — more severe, prolonged, or frequent than prior episodes
Radiation: left arm, left shoulder, neck, jaw.
Anginal equivalents (more common in women, elderly, diabetics):
- Dyspnea
- Epigastric discomfort / nausea
- Diaphoresis
- Generalized weakness or fatigue
Up to 20–30% of MIs are "silent" or atypical — women, diabetics, and the elderly most at risk for atypical presentation.
Physical Examination
The exam may be unremarkable in many patients. Signs of large infarction include:
- Diaphoresis, pale cool skin
- Sinus tachycardia
- S3 and/or S4 heart sound
- Basilar rales (pulmonary edema)
- Hypotension or cardiogenic shock (most severe)
Critical exam goal: exclude life-threatening mimics — aortic dissection, pulmonary embolism, cardiac tamponade.
ECG Diagnosis
STEMI Criteria
Transmural ischemia → ST elevation (current of injury):
- ≥2 contiguous leads:
- ≥2 mm in V2–V3 (men ≥40 yr), ≥2.5 mm (men <40 yr), ≥1.5 mm (women)
- ≥1 mm in all other leads
- New LBBB in the right clinical context is treated as STEMI-equivalent
- Posterior MI: ST depression V1–V3 + tall R waves (mirror image); confirm with V7–V9
Hyperacute T waves may precede ST elevation in the earliest minutes.
Evolutionary changes: ST elevation → Q waves → T-wave inversion → resolution (or permanent Q waves)
NSTEMI / UA (NSTE-ACS) Criteria
- ST depression ≥0.5 mm (subendocardial ischemia)
- T-wave inversions (especially ≥1 mm in multiple leads)
- ECG may be normal (does not exclude NSTEMI)
- Differentiated from UA by troponin elevation
Biomarker Diagnosis — Cardiac Troponin
High-Sensitivity Cardiac Troponin (hs-cTn)
Current standard. Key principles per Tietz Textbook of Laboratory Medicine:
| Strategy | Criteria | Performance |
|---|---|---|
| Single hs-cTnI <LOD (2 ng/L, Abbott) at presentation | Rule-out MI | NPV 99.8%, sensitivity 100% |
| Single hs-cTnT <LOD (5 ng/L, Roche) + non-ischemic ECG | Rule-out MI (~31% classified low risk) | Sensitivity 98.7%, NPV 99.3% |
| hs-cTn 0h/1h algorithm | Δhs-cTn within 1 hour determines rule-in or rule-out | ESC-validated pathway |
Rule-in: moderately elevated hs-cTn at baseline or significant rise (Δ) within 1 hour → high likelihood of NSTEMI → admit to CCU.
Important caveat: Elevated troponin ≠ MI. Causes of Type 2 MI / myocardial injury include PE, decompensated HF, severe hypertension, tachycardia, anemia, sepsis. Clinical context is mandatory.
Older Markers (now largely replaced by hs-cTn)
- CK-MB: rises 4–6h, peaks 12–24h, normalizes by 48–72h (useful for reinfarction detection)
- Myoglobin: earliest but non-cardiac-specific
Risk Stratification
TIMI Score (NSTE-ACS) — 1 point each:
| Risk Factor |
|---|
| Age ≥65 years |
| ≥3 CAD risk factors |
| Known CAD (≥50% stenosis) |
| ST deviation >0.5 mm on presenting ECG |
| ≥2 anginal episodes in prior 24 hours |
| Aspirin use in prior 7 days |
| Elevated cardiac markers (troponin or CK-MB) |
Score 0–2: low risk; 3–4: intermediate; 5–7: high risk for death/MI/urgent revascularization at 14 days.
GRACE Score
Incorporates: age, HR, systolic BP, creatinine, Killip class, ST deviation, cardiac arrest at admission, elevated markers. More continuously calibrated than TIMI.
Diagnostic Mimics to Exclude
| Condition | Distinguishing Feature |
|---|---|
| Aortic dissection | Tearing pain radiating to back, pulse differentials, widened mediastinum |
| Pulmonary embolism | Pleuritic component, hypoxia, S1Q3T3 ECG, D-dimer, CT-PA |
| Acute pericarditis | Diffuse ST elevation (saddle-shaped) in all leads except aVR, pleuritic quality, friction rub |
| Myocarditis | Chest pain + troponin + ECG changes → coronary imaging first; CMR for definitive diagnosis |
| Takotsubo syndrome | Post-stress, apical ballooning, usually post-menopausal women |
| Vasospastic angina (Prinzmetal) | ST elevation during pain, resolves spontaneously or with nitrates |
Summary: Diagnostic Algorithm
Ischemic symptoms?
↓
12-lead ECG within 10 min
├── Persistent STE or new LBBB → STEMI → Activate cath lab
└── No STE → hs-cTn at 0h (±1h)
├── <LOD + non-ischemic ECG → Low risk (rule-out)
├── Intermediate → Serial troponin at 3h; risk score
└── Elevated or rising → NSTEMI → Admit, anticoagulate, risk-stratify
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 285
- Goldman-Cecil Medicine International Edition, Chapter 57
- Tietz Textbook of Laboratory Medicine 7th Ed., Chapter on AMI biomarkers
This is a shared conversation. Sign in to Orris to start your own chat.