Myocardial infarction
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"myocardial infarction"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks plus two excellent images. I have everything needed for a complete overview. Let me compile the full answer.
Myocardial Infarction - Complete Overview
Definition
Myocardial infarction (MI), commonly called a "heart attack," is necrosis of heart muscle resulting from ischemia. The 2018 joint U.S./European Cardiology task force defines it as "acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia."
Epidemiology & Risk Factors
- ~10% of MIs occur before age 40; ~45% before age 65
- Men are at greater risk than women, but the gap narrows with age
- Women are relatively protected during reproductive years; risk rises sharply after menopause (declining estrogen)
- Major risk factors mirror those for atherosclerosis: hypertension, dyslipidemia, diabetes, smoking, obesity, family history
Types of MI
As described in the Sabiston Textbook of Surgery:
- Type 1 MI - atherosclerotic plaque rupture causing occlusion and ischemic infarction (the classic "heart attack")
- Type 2 MI - demand ischemia; mismatch between oxygen supply and demand without plaque rupture (e.g., tachyarrhythmia, severe anemia, hypotension)
Type 1 MI is further classified as:
- STEMI - ST elevation + biomarker elevation (complete occlusion)
- NSTEMI - biomarker elevation without ST elevation (partial/transient occlusion)
- Unstable angina - ischemic symptoms without biomarker elevation
Pathogenesis
Robbins & Kumar Basic Pathology describes the typical sequence:
- An atheromatous plaque is eroded or disrupted by endothelial injury, intraplaque hemorrhage, or mechanical forces, exposing subendothelial collagen and necrotic contents
- Platelets adhere, aggregate, and activate, releasing thromboxane A2, ADP, and serotonin - causing further aggregation and vasospasm
- Coagulation is activated by exposure of tissue factor, adding to the thrombus
- Within minutes, the enlarging thrombus fully occludes the coronary lumen
Angiography within 4 hours of MI onset shows coronary thrombosis in ~90% of cases. When performed at 12-24 hours, only 60% still show thrombus - indicating spontaneous thrombolysis occurs.
In 10% of cases, transmural MI occurs without occlusive atherosclerosis - due to vasospasm, embolism from mural thrombi (e.g., atrial fibrillation), or valve vegetations.
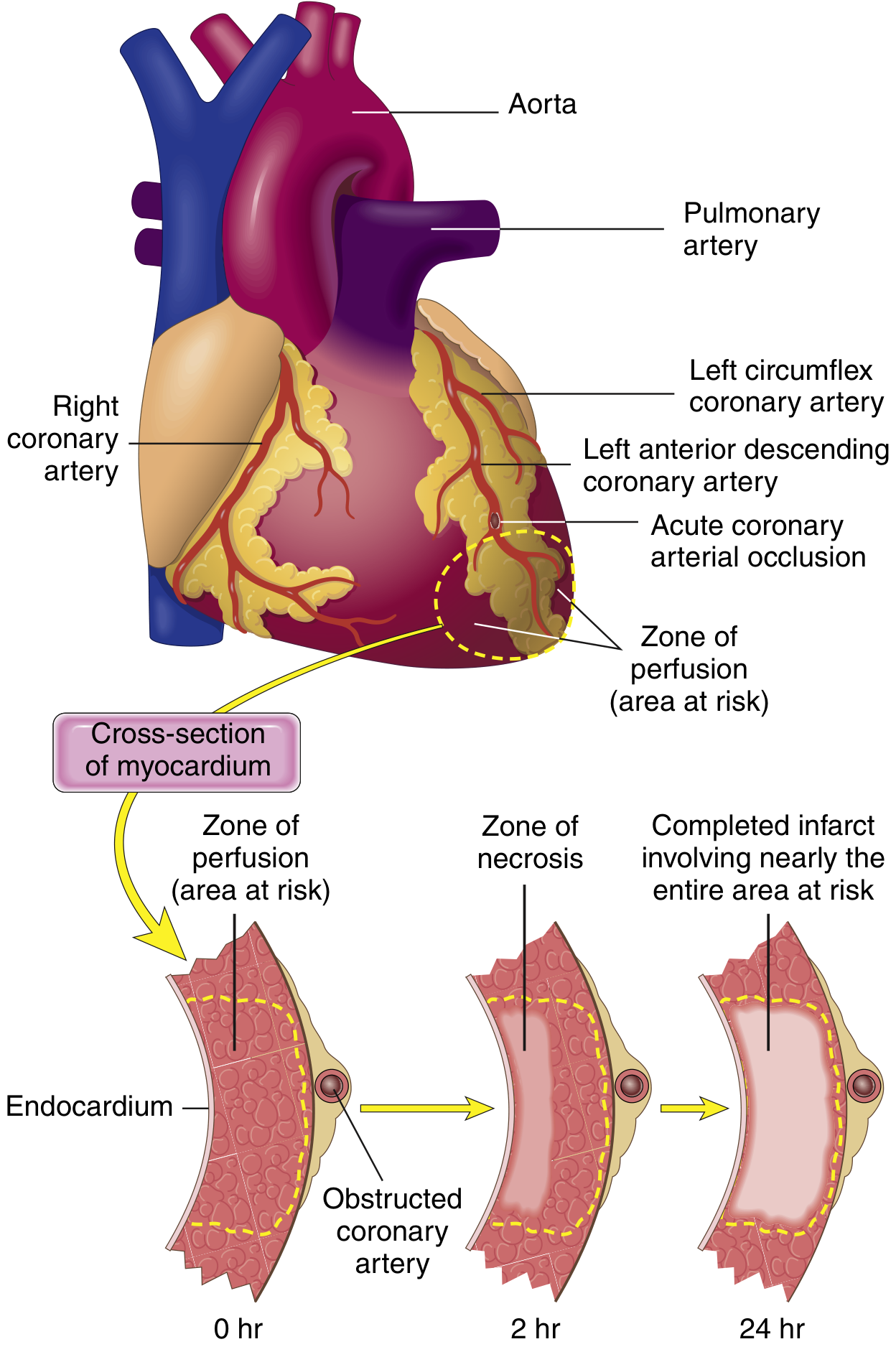
Myocardial Response to Ischemia
From Robbins & Kumar:
- Within seconds: aerobic metabolism ceases → ATP drops → lactic acid accumulates
- Within minutes: loss of contractility (reversible at this stage)
- 20-40 minutes of persistent ischemia: irreversible coagulative necrosis
- The subendocardial zone is most susceptible - it receives blood last from epicardial vessels and is compressed by high intramural pressures
Per Guyton and Hall Physiology: cardiac muscle requires ~1.3 mL O2/100g/min just to stay alive. Even 15-30% of normal resting coronary flow can prevent death of most cells - but the central core of a large infarct, with near-zero flow, dies.
A full-thickness infarct achieves its complete extent in 3 to 6 hours - the critical therapeutic window.
Coronary Artery Territories
| Artery | Territory | % of MIs |
|---|---|---|
| Left Anterior Descending (LAD) | Anterior LV wall, anterior 2/3 of septum, apex | 40-50% |
| Right Coronary Artery (RCA) | Most of RV, posterior LV (right-dominant) | 30-40% |
| Left Circumflex (LCX) | Lateral LV wall | 15-20% |
Morphological Evolution
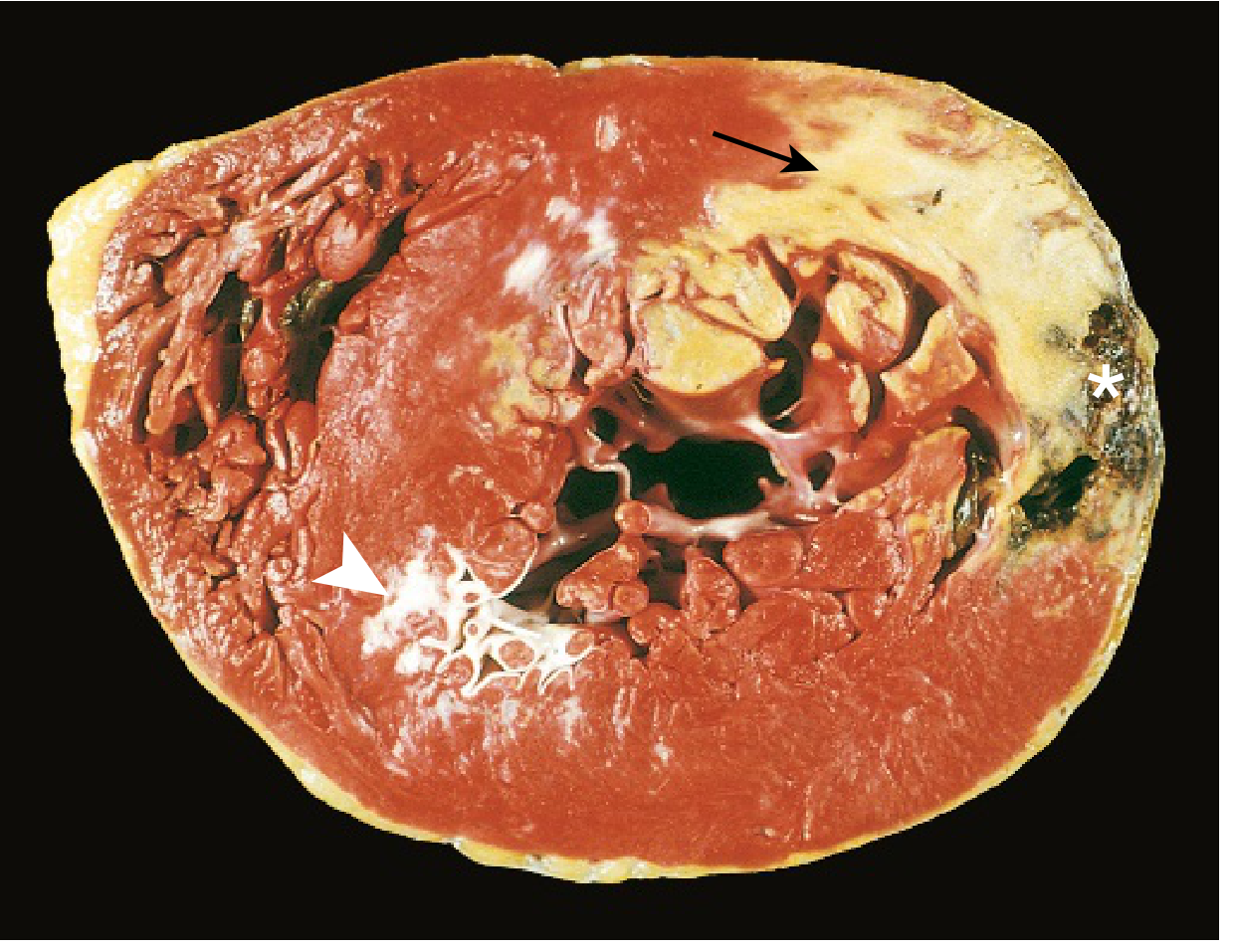
The table below is from Robbins & Kumar Basic Pathology:
| Time Frame | Gross Appearance | Light Microscopy |
|---|---|---|
| 0-½ hour | None | None |
| ½-4 hours | None | Wavy fibers at border; sarcolemmal disruption |
| 4-12 hours | Occasional dark mottling | Coagulation necrosis begins; edema; hemorrhage |
| 12-24 hours | Dark mottling | Coagulation necrosis; pyknotic nuclei; hypereosinophilic myocytes; early neutrophil infiltrate |
| 1-3 days | Mottling with yellow-tan center | Coagulation necrosis; increased neutrophils |
| 3-7 days | Hyperemic border; central yellow-tan softening | Neutrophil death; macrophages begin phagocytosis |
| 7-10 days | Maximally yellow-tan and soft; depressed red-tan margins | Well-developed macrophage phagocytosis; early granulation tissue |
| 10-14 days | Red-gray depressed borders | Established granulation tissue; new vessels; collagen deposition |
| 2-8 weeks | Gray-white scar (border to core) | Increasing collagen; decreasing cellularity |
| >2 months | Scarring complete | Dense collagenous scar |
Key point: Myocardial necrosis proceeds invariably to scar without regeneration.
ECG Changes
From Ganong's Review of Medical Physiology, three electrical defects occur in infarcted cells:
| Defect | Current Flow | ECG Change (leads over infarct) |
|---|---|---|
| Rapid repolarization | Out of infarct | ST elevation |
| Decreased resting membrane potential | Into infarct | TQ depression (recorded as ST elevation) |
| Delayed depolarization | Out of infarct | ST elevation |
Hallmark of acute MI: ST segment elevation in leads overlying the infarct; ST depression in reciprocal leads.
After days to weeks, the ST changes resolve. Dead tissue becomes electrically silent. The characteristic late change is the development of Q waves in leads overlying the infarct.
Localizing MI by ECG leads:
- Anterior (LAD): V1-V4
- Lateral (LCX): I, aVL, V5-V6
- Inferior (RCA): II, III, aVF
- Posterior (RCA/LCX): tall R in V1-V2 (reciprocal)
Cardiac Biomarkers
- Troponin I and T - most sensitive and specific; rise 3-6 hours post-MI, peak at 24-48h, remain elevated 7-10 days (troponin T) or 5-7 days (troponin I)
- CK-MB - rises in 4-6h, peaks at 24h, returns to normal in 48-72h; used to detect re-infarction
- Myoglobin - earliest to rise (1-3h) but not cardiac-specific
Clinical Presentation
Typical:
- Severe, crushing/pressure chest pain - often radiating to the left arm, jaw, or back
- Duration >20 minutes (differentiates from stable angina)
- Diaphoresis, nausea, vomiting
- Dyspnea
Atypical (especially women, elderly, diabetics):
- Epigastric pain, fatigue, jaw pain, or no pain at all ("silent MI")
Management
Acute STEMI - "Time is muscle"
-
Immediate reperfusion (within 90 min "door-to-balloon"):
- Primary PCI (preferred if available within 90 min)
- Thrombolysis (if PCI unavailable within 120 min)
-
Antiplatelet therapy:
- Aspirin 300 mg loading
- P2Y12 inhibitor (ticagrelor or clopidogrel)
-
Anticoagulation: heparin (UFH or LMWH)
-
Supplemental O2 if SpO2 <94%
-
Nitrates: sublingual/IV for chest pain and hypertension (avoid in RV infarction - can cause catastrophic preload reduction)
-
Beta-blockers: cardioprotective; start if no cardiogenic shock, bradycardia, or low EF
-
Morphine: for pain unrelieved by nitrates
NSTEMI / Unstable Angina
- Risk-stratify (TIMI/GRACE score)
- High-risk: early invasive strategy (angiography within 24-72h)
- Medical therapy: antiplatelet + anticoagulation + statin
Secondary Prevention
- Aspirin lifelong
- Statin (high-intensity, e.g., atorvastatin 40-80 mg)
- ACE inhibitor / ARB - especially if EF reduced or anterior MI; prevents remodeling
- Beta-blocker - reduces sudden cardiac death
- Aldosterone antagonist (eplerenone) if EF <40% and no renal failure
Recent meta-analysis (Chi et al., 2025) found beta-blockers for secondary prevention post-MI may not reduce mortality in patients without reduced ejection fraction or heart failure - an evolving evidence area.
Complications
From Guyton and Hall and Robbins:
Early (within days)
- Arrhythmias - most common cause of death; ventricular fibrillation accounts for 80-90% of ischemic cardiac deaths
- Cardiogenic shock - pump failure; mortality ~80% without intervention
- Acute heart failure - pulmonary edema from LV dysfunction
- Systolic stretch - non-contractile infarcted segment bulges outward during systole, worsening effective output
Mechanical complications (days 1-14, highest risk 3-7 days)
- Free wall rupture - leads to hemopericardium and tamponade; usually fatal
- Interventricular septal rupture - new harsh pansystolic murmur; requires surgical repair
- Papillary muscle rupture - acute severe mitral regurgitation; cardiogenic shock
Late complications
- Ventricular aneurysm - fibrotic bulge of infarcted wall; risk of mural thrombus, arrhythmia, and persistent heart failure
- Dressler syndrome (post-MI pericarditis) - autoimmune pericarditis 2-10 weeks post-MI; fever, pleuritic chest pain, elevated ESR; treated with NSAIDs/aspirin
- Chronic heart failure - progressive LV remodeling
- Sudden cardiac death - Peek et al., 2024 found in a meta-analysis of pooled cohorts that sudden cardiac death risk remains significantly elevated for years after MI
Key Pearls
- Irreversible injury begins at 20-40 minutes of ischemia
- Full infarct develops in 3-6 hours - the reperfusion window
- LAD occlusion = most common (40-50%); often fatal if proximal
- Subendocardium is always more vulnerable than epicardium
- ECG: ST elevation = acute injury; Q waves = established necrosis
- Right-sided MI: avoid nitrates and diuretics; maintain preload
- Cardiac troponin is the gold standard biomarker
- After MI, healing produces only scar - no myocardial regeneration
Sources: Robbins & Kumar Basic Pathology; Ganong's Review of Medical Physiology, 26th Ed; Guyton and Hall Textbook of Medical Physiology; Sabiston Textbook of Surgery; Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.