make notes on sciatica
Reading File
Finding Sources
Searching PubMed
sciatica lumbar radiculopathy
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
I now have rich content from multiple authoritative textbooks. Let me compile comprehensive notes.
Sciatica - Clinical Notes
Definition
Sciatica refers to pain that radiates along the distribution of the sciatic nerve, typically from the lower back through the buttock and down the posterior or lateral leg, often reaching the foot or ankle. It is a symptom, not a diagnosis - reflecting compression or irritation of one or more lumbosacral nerve roots (most commonly L4, L5, or S1).
- Symptom to Diagnosis, 4th Ed.
Epidemiology
-
Lifetime prevalence of true sciatica: 2-4% (contrast with low back pain: 60-80%)
-
90% of acute low back pain resolves within 6 weeks
-
70% of acute sciatica episodes resolve within 3 months
-
5-7% of the population aged 45-64 years report back problems as a chronic sickness
-
Bailey and Love's Short Practice of Surgery, 28th Ed.
Anatomy
The spinal canal houses the thecal sac containing the spinal cord (which terminates at L1) and the nerve roots in the lateral portions. The intervertebral foramen is bounded:
- Superiorly and inferiorly by pedicles
- Anteriorly by the disc
- Posteriorly by the facet joint
Degenerative changes in any of these structures can compress nerve roots. The sciatic nerve is the largest nerve in the body, formed from the lumbosacral plexus (L4-S3).
- Bailey and Love's; Adams and Victor's Principles of Neurology, 12th Ed.
Causes / Etiology
Most common: Herniated nucleus pulposus (disc herniation) - accounts for the vast majority
Other causes (differential diagnosis of lower limb pain suggestive of sciatica):
Neurogenic - within the spine (Spondylotic):
- Herniated nucleus pulposus
- Stenosis of central canal, lateral recess, or intervertebral foramen
- Synovial cyst (from degenerative facet joint disease)
- Arachnoid or perineural (Tarlov) cysts
- Sterile inflammatory arachnoiditis
- Tumor: primary (neurofibroma, ependymoma) or metastatic (bone/epidural/meningeal)
- Infection: disc, epidural, herpes zoster, Lyme disease
- Inflammatory radiculopathy (sarcoidosis, paraneoplastic)
Neurogenic - outside the spine:
- Lumbosacral plexus involvement
- Sciatic neuropathy
- Peripheral neuropathy
Non-neurogenic:
- Musculoskeletal (hip arthritis, trochanteric bursitis, sacroiliac joint disease, piriformis syndrome, iliotibial band syndrome, hamstring tendinitis)
- Peripheral vascular disease
Special/rare causes:
-
Piriformis syndrome - the sciatic nerve passes under (or occasionally through) the piriformis muscle; spasm or hypertrophy may compress it. Pain is elicited by hip flexion, adduction, and internal rotation.
-
Catamenial sciatica - temporally linked to the premenstrual period; almost always due to endometriosis at the sciatic notch.
-
Pregnancy-related sciatica - uterine traction on the nerve.
-
Cauda equina compression from epidural tumor (prostate/breast cancer, myeloma), lymphoma, or inflammatory conditions (CMV in AIDS, Lyme disease/Bannwarth syndrome, herpetic infection, neoplastic meningitis, Guillain-Barre).
-
Goldman-Cecil Medicine; Adams and Victor's; Tintinalli's Emergency Medicine
Disc Herniation - Key Points
- 95% of clinically important herniations occur at L4-L5 and L5-S1
- A smaller proportion (often elderly) occurs at L2-L3 and L3-L4
- Pain and paresthesias follow the dermatomal distribution of the affected root
- Radicular pain is typically described as sharp, shooting, burning, throbbing, or tingling
- Contact of the disc with a nerve root provokes inflammation - this (not just mechanical compression alone) drives symptoms
Nerve Root Levels - Clinical Findings
| Nerve Root | Distribution of Pain | Sensory Changes | Motor Weakness | Lost Reflex |
|---|---|---|---|---|
| L4 | Anteromedial thigh | Medial lower leg | Knee extension, hip adduction | Knee jerk |
| L5 | Lateral thigh, lateral lower leg, dorsum of foot | Lateral thigh, lateral lower leg, dorsum of foot | Foot dorsiflexion, foot eversion + inversion, hip abduction | None reliable |
| S1 | Posterior thigh, calf, heel | Sole, lateral foot + ankle, 4th and 5th toes | Foot plantar flexion, knee flexion, hip extension | Ankle jerk |
- Symptom to Diagnosis, 4th Ed.
Clinical Features
History:
- Pain radiating from the back down the buttock and leg, typically to the foot or ankle
- Associated numbness or paresthesias in a dermatomal distribution
- Pain classically worsened by coughing, sneezing, or sudden increases in intra-abdominal/intraspinal pressure (Naffziger sign)
- Radicular pain is a more prominent complaint than back pain in disc herniation
- Pain precipitated or worsened by forward bending, lifting
Examination signs:
- Antalgic posture (sciatic scoliosis) - reflex paraspinal muscle contraction; knee slightly flexed on affected side
- When disc herniates lateral to the nerve root: trunk bends toward side of lesion; medial to root: bends away
- Walking is cautious with brief weight bearing and a limp
- Knee slightly flexed to relax hamstrings
Straight Leg Raise (SLR) - Lasègue Sign
- Patient supine; examiner raises the straight leg
- Positive test: Reproduces sciatic pain (shooting down the leg) when the leg is elevated between 30-60 degrees
- Sensitivity: 72-97%, Specificity: 11-66%
- When sciatica is reproduced: Sensitivity 95%, Specificity 88%, LR+ 7.9, LR- 0.06
Crossed SLR (Fajersztajn Sign)
- Raising the contralateral straight leg reproduces pain on the affected side
- More specific but less sensitive for herniated disc than the ipsilateral SLR
- Sensitivity 25%, Specificity 90%
Other signs:
-
Bragard sign - dorsiflexion of the foot accentuates SLR pain
-
Sicard sign - dorsiflexion of the great toe accentuates pain
-
Neri sign (standing) - forward trunk bending causes knee flexion on the affected side
-
Valleix points - pressure along the sciatic nerve course (sciatic notch, retrotrochaneric gutter, posterior thigh, head of fibula) reproduces radiating pain
-
Adams and Victor's; Goldman-Cecil; Symptom to Diagnosis; Rosen's Emergency Medicine
Investigations
Imaging
- MRI is the preferred modality (gold standard for soft tissue/disc detail)
- Non-urgent MRI for most cases of suspected disc herniation
- Urgent/emergent MRI if suspected: epidural compression, cauda equina syndrome, rapid progressive neurologic deficit, or red-flag features
- Plain radiographs: useful if tumor, fracture, spondylolisthesis, or infection is suspected
- If symptoms are not severe or rapidly progressive, MRI can be ordered routinely rather than emergently
Electrodiagnostics (EMG/NCS)
-
Needle EMG is the most sensitive EDX tool in suspected lumbosacral radiculopathy
-
Fibrillation potentials are the most objective finding - confirm denervation in a segmental myotomal distribution with normal SNAP in the corresponding dermatome
-
EMG may be normal if only the dorsal root is compressed (pain/paresthesias only, no motor involvement)
-
EMG and imaging are complementary: EMG = nerve root function; imaging = anatomy
-
Bradley and Daroff's Neurology in Clinical Practice; Goldman-Cecil; Tintinalli's
Cauda Equina Syndrome - Red Flag
The most common cause is a very large L4-5 or L5-S1 disc herniation. Other causes: tumor, abscess, epidural hematoma, scarring.
Features:
- Low back pain
- Uni- or bilateral sciatica
- Saddle anaesthesia
- Motor weakness in the lower extremities
- Variable rectal and urinary symptoms
Unless onset is gradual, this requires emergent MRI and neurosurgical consultation.
- Goldman-Cecil; Bailey and Love's
Treatment
Conservative (first-line for most patients)
- Activity: Routine daily activity is as effective as 2 weeks of bed rest. Early mobilization accelerates recovery; prolonged immobilization is detrimental.
- Analgesics: NSAIDs are first-line (though less effective for disc herniation than non-specific back pain); limited opioids for severe pain
- Note: Most sufferers of acute sciatica recover within 6 weeks using simple nonoperative therapy
Medications with limited/no evidence:
- Oral corticosteroids - no lasting measurable benefit in sciatica
- Muscle relaxants - insufficient evidence
- Antiepileptics/anticonvulsants - insufficient evidence; pregabalin is not helpful for acute or chronic sciatica
- Antidepressants - studies find little benefit
Epidural Corticosteroid Injections (ESI)
- Provides a minor reduction in leg pain and sensory deficits vs. placebo at 2-6 weeks
- No significant functional benefit; does not reduce the need for surgery
- Not an emergency department procedure; option for moderately-to-severely symptomatic patients at follow-up
- No proven longer-lasting value beyond 6 weeks
Physical therapy / Spinal manipulation
- Spinal manipulative therapy results in a small decrease in pain up to 12 weeks
- Back-strengthening exercises help chronic cases
Surgery - Indications (all three criteria must be met):
- Definitive evidence of herniation on imaging
- Corresponding clinical picture and neurologic deficit
- Failure of adequate conservative therapy
Additional indications: Spinal instability, severe/progressive neurologic deficits, myelopathy, cauda equina syndrome, uncontrollable severe radicular pain with root compression evidence.
Surgical approach: Microsurgical discectomy with minimal laminectomy is most common for disc herniation. ~90% of patients report excellent relief of neuropathic pain post-operatively. Surgery is better than non-operative therapy at 2-3 months, but this advantage diminishes with longer follow-up.
Failed back surgery syndrome is a risk, especially when patients lack objective radiculopathy signs or corresponding neuroimaging.
- Tintinalli's; Bradley and Daroff's; Goldman-Cecil
Prognosis
- Most patients with herniated disc improve with nonsurgical therapy
- Over 50% recover in 6 weeks
- Workers off work for >6 months have a guarded prognosis for return to work
- Recurrent disc herniation or incomplete discectomy are common causes of poor post-operative outcomes
Recent Evidence (PubMed, 2024-2026)
- A 2024 systematic review of clinical practice guidelines (PMID: 38629664) synthesised medication recommendations for lumbosacral radiculopathy - useful for checking current drug guidance.
- A 2025 meta-analysis (PMID: 40488872) examined how symptom duration before lumbar discectomy affects outcomes - earlier surgery may yield better results.
- A 2024 systematic review (PMID: 38190195) assessed diffusion tensor MRI for lumbosacral nerve root evaluation - a potentially useful advanced imaging tool.
Sources: Tintinalli's Emergency Medicine; Adams and Victor's Principles of Neurology, 12th Ed.; Goldman-Cecil Medicine; Bailey and Love's Short Practice of Surgery, 28th Ed.; Bradley and Daroff's Neurology in Clinical Practice; Symptom to Diagnosis, 4th Ed.; Rosen's Emergency Medicine.
Search for clinical images showing disc herniation anatomy
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Excellent - I now have a comprehensive set of clinical images from multiple authoritative textbooks. Here is the full visual gallery with explanations:
Disc Herniation Anatomy - Clinical Images
1. Central vs. Posterolateral Disc Herniation (Axial Anatomy)
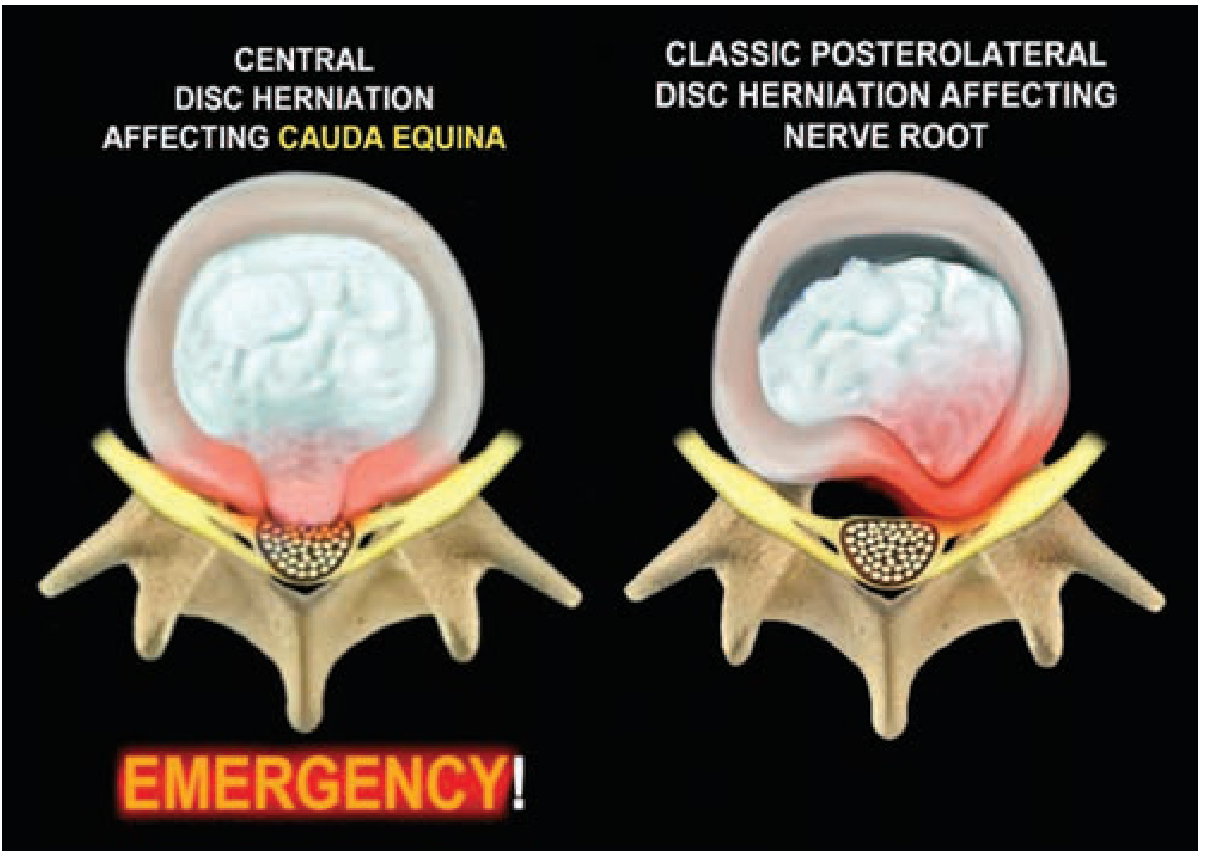
Fig. 43-33 (Schwartz's Principles of Surgery, 11th Ed.) - This is one of the most clinically important anatomical concepts. A central disc herniation (left) compresses the entire cauda equina - this is a surgical emergency. A posterolateral disc herniation (right) compresses a single nerve root and can often be managed conservatively initially.
2. Sagittal MRI - Large Lumbar Disc Herniation

Fig. 369-8 (Goldman-Cecil Medicine) - Sagittal MRI showing a large lumbar disc herniation. The two arrows point to the herniated nucleus pulposus material bulging posteriorly into the spinal canal and compressing the thecal sac.
3. Disc Herniation Types - Protrusion vs. Extrusion (Axial Schematic)
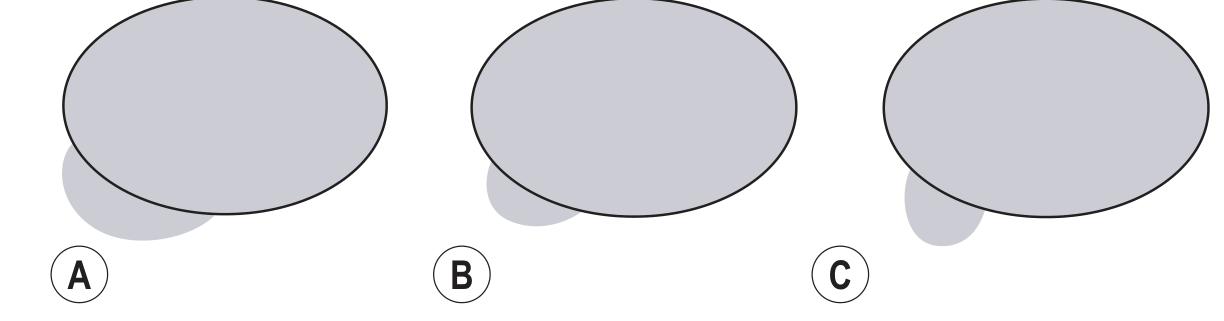
Fig. 48.8 (Grainger & Allison's Diagnostic Radiology) - Types of disc herniation in the axial plane:
- (A) Broad-based protrusion - base broader than apex, >25% of disc circumference involved
- (B) Focal protrusion - base broader than apex, <25% of disc circumference
- (C) Extrusion - base narrower than the apex ("toothpaste sign"); an extrusion is rarely seen in asymptomatic patients
4. Herniation Location Classification (Axial Plane)
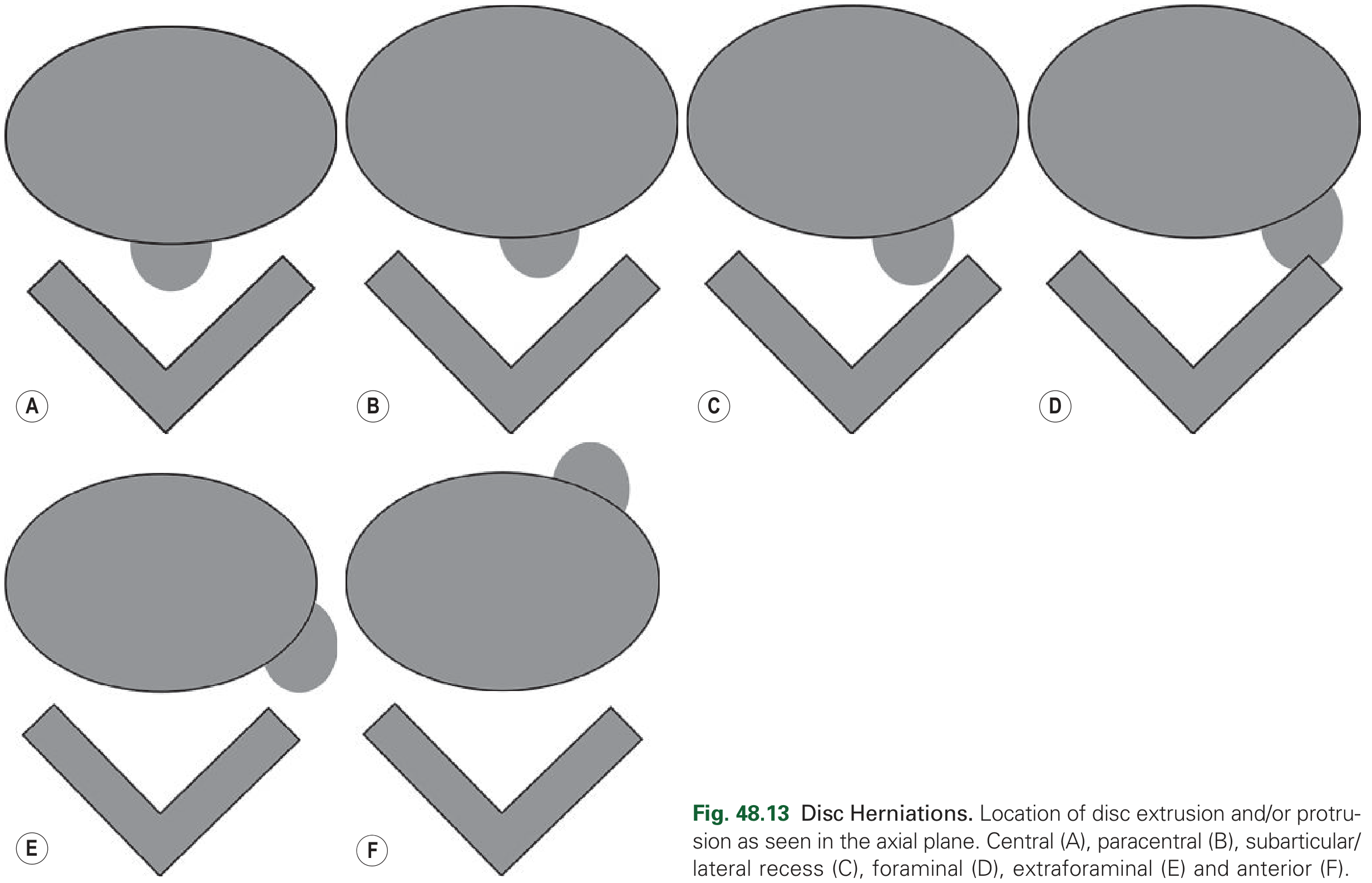
Fig. 48.13 (Grainger & Allison's Diagnostic Radiology) - The six anatomical zones of disc herniation in the axial plane:
- (A) Central - posterior midline; risks cauda equina syndrome
- (B) Paracentral - right or left of midline; most common cause of sciatica
- (C) Subarticular / lateral recess - compresses traversing nerve root in the lateral recess
- (D) Foraminal - within the neural foramen, compresses exiting nerve root
- (E) Extraforaminal - outside the neural foramen; far lateral, compresses the exiting nerve root one level higher than expected
- (F) Anterior - rare, usually asymptomatic
5. Massive Disc Extrusion - MRI (Sagittal + Axial T2)
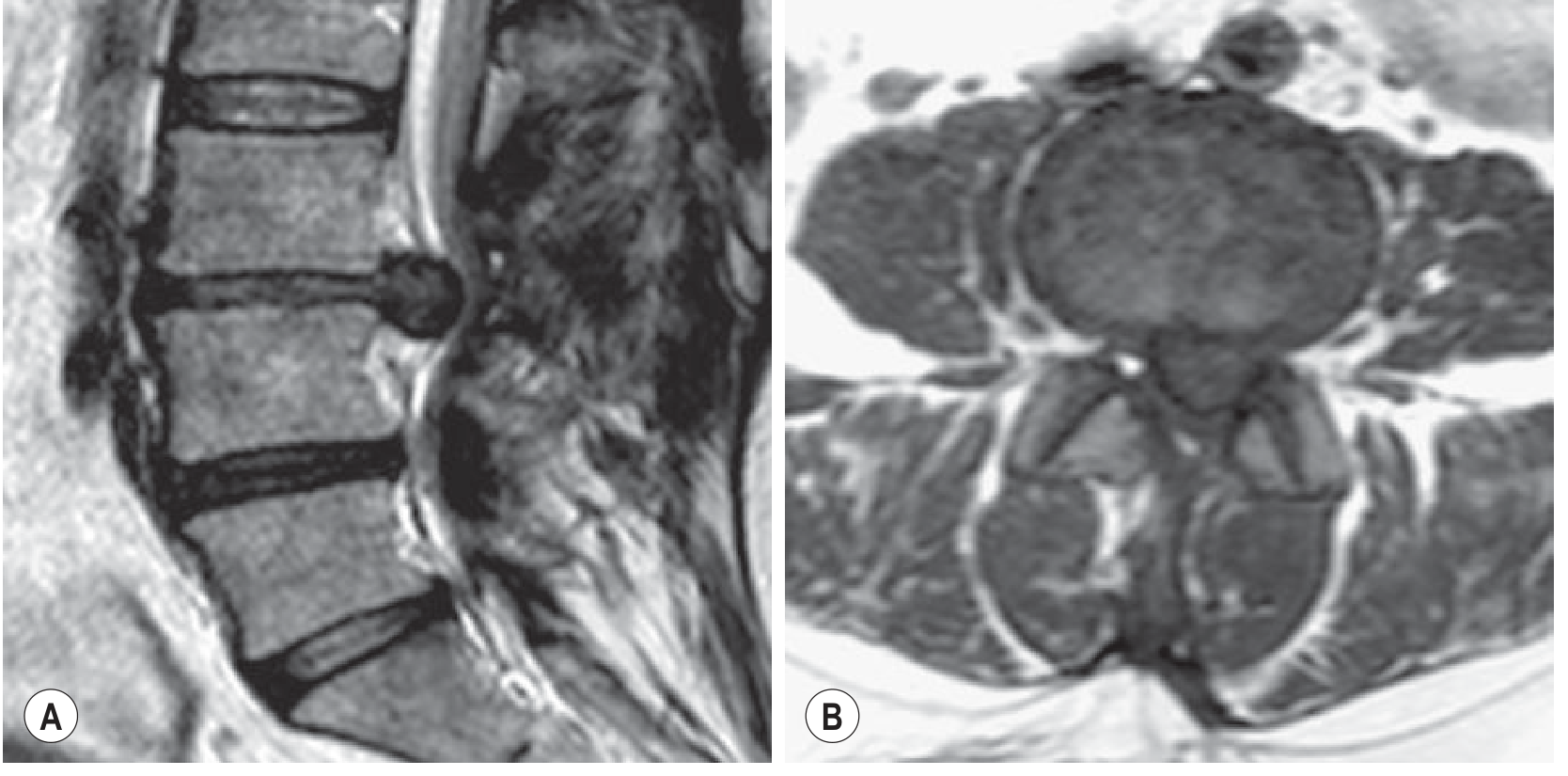
Fig. 48.9 (Grainger & Allison's Diagnostic Radiology) - 45-year-old woman. Sagittal (A) and axial (B) T2-weighted images show a massive lumbar disc extrusion at L3-L4 with:
- Displacement of nerve roots
- Obliteration of the left lateral recess
- Loss of disc height at L3-L4
- Decreased disc signal at L4-L5 (early degenerative change)
6. Foraminal Disc Protrusion - CT (Sagittal + Axial, Bone and Soft Tissue Windows)
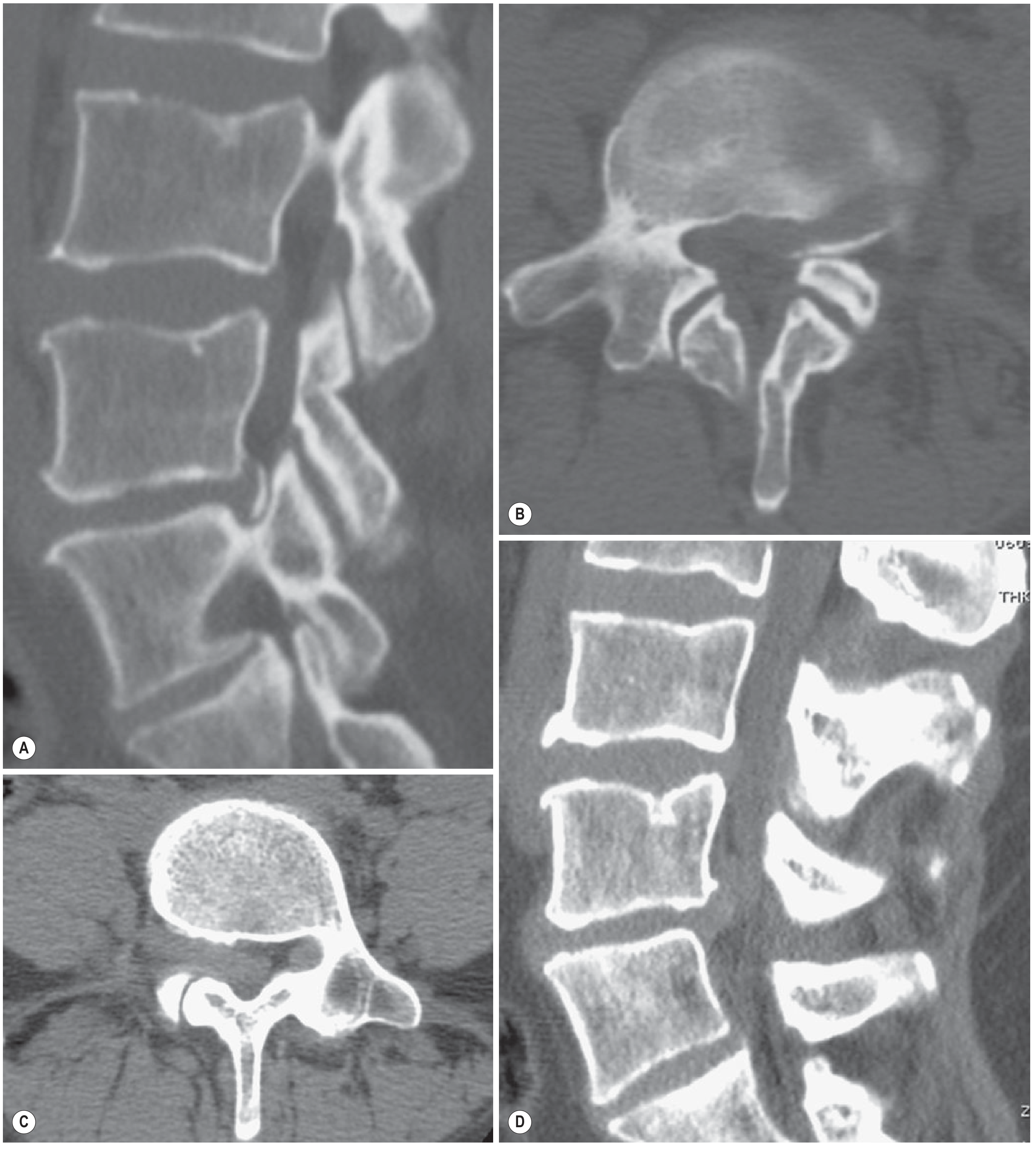
Fig. 48.10 (Grainger & Allison's Diagnostic Radiology) - Reformatted CT images showing:
- (A, B) Broad-based foraminal disc protrusion on the left at L4-L5 with a calcified outer rim (bone window)
- (C, D) Broad-based disc protrusion on the right at L5-S1 (soft-tissue window) This demonstrates how CT can identify calcified fragments and foraminal compromise.
7. Sequestrated Disc Fragment with Gadolinium Enhancement - MRI
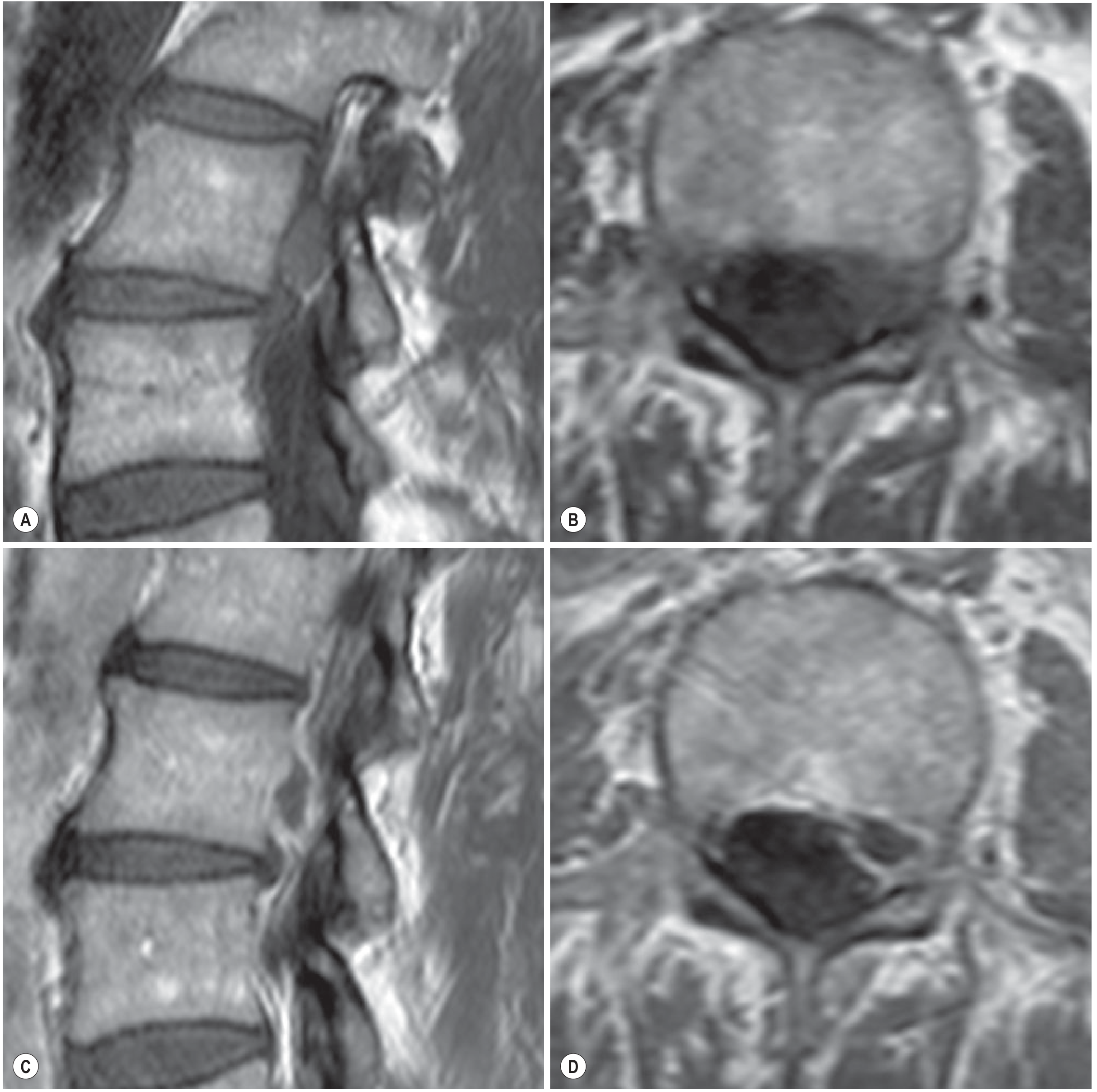
Fig. 48.11 (Grainger & Allison's Diagnostic Radiology) - Pre- and post-gadolinium T1-weighted images of a sequestrated (free) disc fragment posterior to L2:
- (A, B) Precontrast sagittal and axial T1
- (C, D) Post-gadolinium: peripheral rim enhancement around the fragment
- Clinical pearl: Peripheral contrast enhancement is associated with a high probability of spontaneous regression - an important prognostic indicator
8. CT Myelography of Lumbar Disc Herniation at L4-5 (Multiple Views)
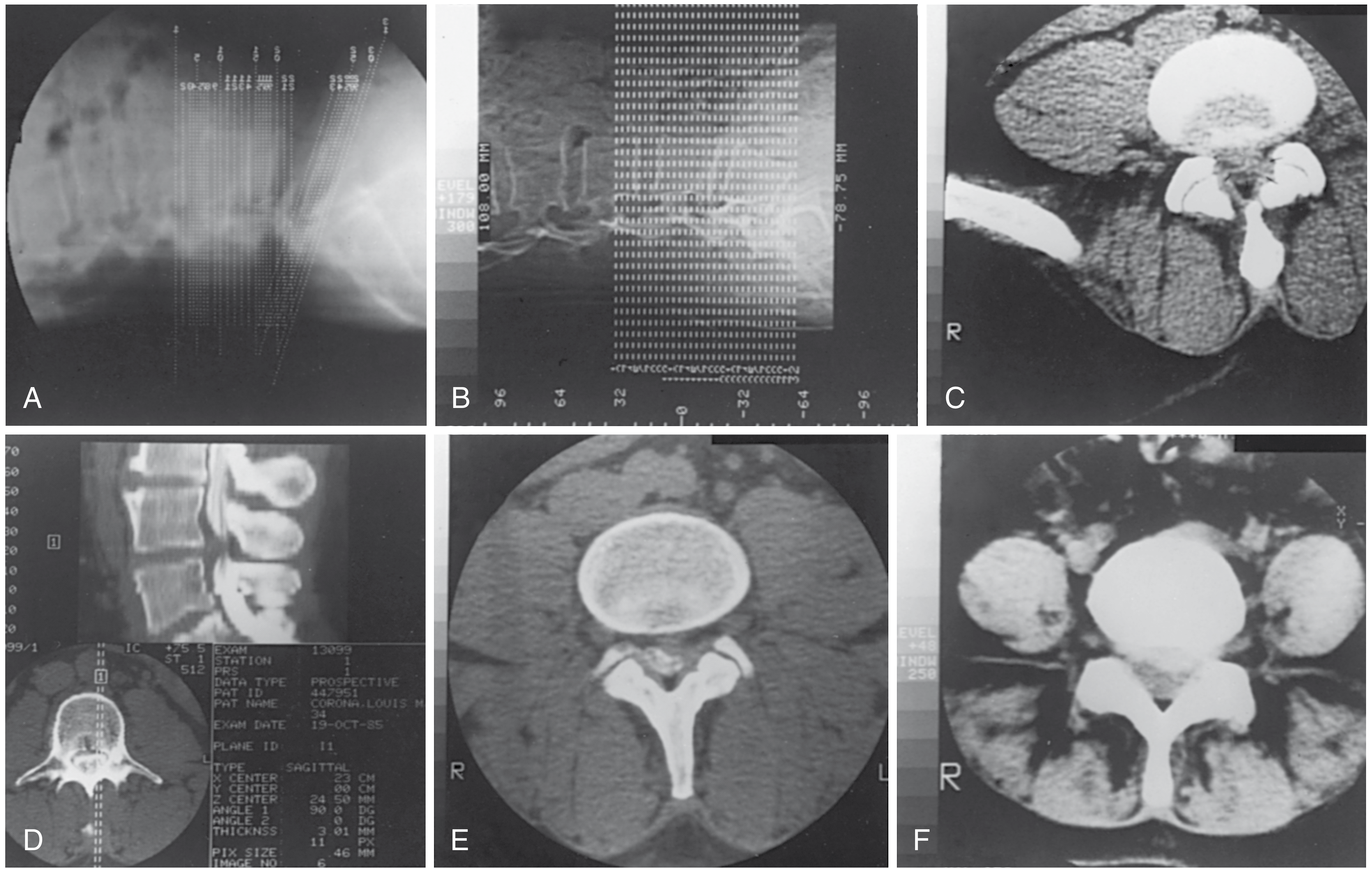
Fig. 46.2 (Campbell's Operative Orthopaedics, 15th Ed., 2026) - CT series of L4-5 disc herniation:
- (A) Scout view (angled gantry technique)
- (B) Scout view (straight gantry)
- (C) Cross-sectional axial CT at L4-5 disc level - normal soft tissue anatomy
- (D) Sagittal and coronal reformats (computerized reformatted technique)
- (E) Axial CT 2 hours after metrizamide myelography - contrast outlines the thecal sac, clearly delineating the herniation
- (F) Axial CT after IV contrast injection for greater soft-tissue differentiation
Key Anatomical Points Illustrated
| Concept | Image |
|---|---|
| Central vs. posterolateral herniation | Image 1 (Schwartz's) |
| Sagittal MRI appearance | Image 2 (Goldman-Cecil) |
| Protrusion vs. extrusion distinction | Image 3 (Grainger & Allison) |
| Six zones of herniation location | Image 4 (Grainger & Allison) |
| Massive extrusion with nerve displacement | Image 5 (Grainger & Allison) |
| Foraminal herniation on CT | Image 6 (Grainger & Allison) |
| Sequestration + contrast enhancement | Image 7 (Grainger & Allison) |
| CT myelography technique | Image 8 (Campbell's Operative) |
Sources: Schwartz's Principles of Surgery 11th Ed.; Goldman-Cecil Medicine; Grainger & Allison's Diagnostic Radiology; Campbell's Operative Orthopaedics 15th Ed. (2026)
make script for reel
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.