Explain me about hysterectomy
Reading File
Finding Sources
Searching PubMed
hysterectomy indications outcomes
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Here is a thorough explanation of hysterectomy, drawn from Berek & Novak's Gynecology and Sabiston Textbook of Surgery.
Hysterectomy
Hysterectomy is the surgical removal of the uterus. It is the second most common major surgical procedure performed on women of reproductive age in the United States, surpassed only by cesarean section.
Definition
By definition, hysterectomy removes the uterine corpus. Depending on the extent of the operation and the surgical route, adjacent structures (cervix, fallopian tubes, ovaries) may also be removed at the same time.
Types of Hysterectomy
By Extent of Removal
| Type | What is Removed |
|---|---|
| Total hysterectomy | Uterine corpus + cervix |
| Subtotal (supracervical) hysterectomy | Uterine corpus only; cervix is left behind |
| Radical hysterectomy | Uterus + cervix + parametria + upper vaginal cuff (for malignancy) |
When the fallopian tubes and/or ovaries are also removed, the procedure is called:
- Salpingectomy - removal of fallopian tubes (now often done as "opportunistic salpingectomy" to reduce ovarian cancer risk)
- Oophorectomy - removal of ovaries
- Bilateral salpingo-oophorectomy (BSO) - both tubes and ovaries removed
By Surgical Route
1. Total Abdominal Hysterectomy (TAH)
- Performed through a low transverse (Pfannenstiel) or vertical midline incision
- Incision choice depends on indication, body habitus, surgical history, and size of pathology
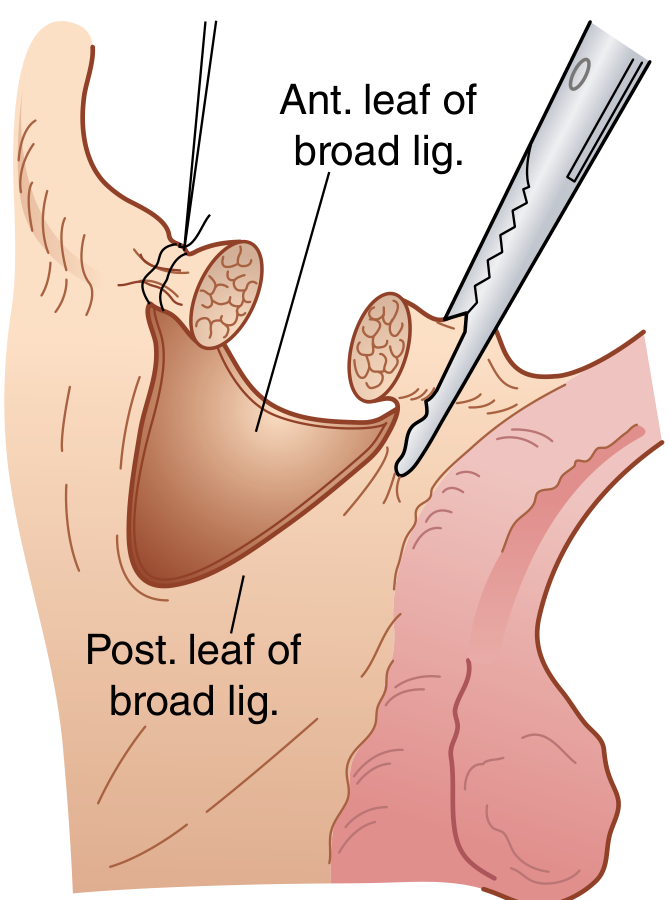
- The round ligaments are divided first, the anterior leaf of the broad ligament is incised, the bladder flap is developed, then the ovarian and uterine vessels are ligated before completing the cuff closure
2. Vaginal Hysterectomy (VH)
- Performed entirely through the vagina with no abdominal incision
- Associated with lower morbidity and shorter hospital stays than abdominal hysterectomy
- Preferred route when anatomy is favorable (uterine descent, adequate vaginal access, no large fibroids or expected adhesions)
3. Laparoscopic Hysterectomy (LH)
- Introduced in 1989; by 2006, accounted for ~15.5% of all hysterectomies
- Encompasses laparoscopic-assisted vaginal hysterectomy (LAVH), total laparoscopic hysterectomy, and supracervical hysterectomy
- Complication rates of LH and VH are now similar, both lower than abdominal hysterectomy
- Offers less postoperative pain, faster recovery, and lower hospital readmission rates compared to open surgery
- Procedural costs are higher, but reduced hospital stay and faster return to work partially offset this
- LH offers no advantage over VH when VH is technically feasible; LH's ideal role is as a replacement for laparotomy
4. Robotic Hysterectomy
- FDA approved in 2005; accounted for 8.2% of hysterectomies by 2010
- Compared to standard laparoscopy: reduced estimated blood loss, shorter hospital stay, and 4x lower conversion rate; surgical time is similar (~117 vs. 118 minutes)
- Cost is higher
Here is a surgical diagram showing incision of the broad ligament - a key step in hysterectomy:
Indications
Hysterectomy is performed for both benign and malignant conditions:
Benign Indications
- Uterine fibroids (leiomyomata) - the most common indication; causes heavy bleeding, bulk symptoms, pelvic pressure
- Adenomyosis - diffuse or focal invasion of endometrial glands into myometrium causing dysmenorrhea and menorrhagia
- Abnormal uterine bleeding unresponsive to medical or conservative surgical management
- Endometriosis with chronic pelvic pain, especially in women who have completed childbearing
- Uterine prolapse - often combined with pelvic floor repair
- Chronic pelvic pain (CPP) - only after at least 6 months of pain without correctable pathology (ACOG criteria); hysterectomy for central pelvic pain with dysmenorrhea and uterine tenderness provides relief in ~74-77% of women, but ~25% have persistent or worsened pain at 1 year
Malignant/Premalignant Indications
- Endometrial carcinoma - standard treatment
- Cervical carcinoma - radical hysterectomy for early-stage disease
- Cervical intraepithelial neoplasia (CIN) - hysterectomy is the treatment of last resort, appropriate for: microinvasion, histologically confirmed recurrent high-grade CIN, or co-existing gynecologic pathology requiring surgery
- Ovarian carcinoma - as part of cytoreductive surgery
- Gestational trophoblastic disease
Surgical Steps (Total Abdominal Hysterectomy)
The key anatomical steps (as illustrated in Sabiston Surgery, Figure 120.12):
- Transection of the round ligaments bilaterally
- Incision of the anterior and posterior broad ligament
- Development of the bladder flap - dissecting the bladder off the lower uterine segment/cervix
- Division of the ovarian/infundibulopelvic vessels (if BSO is planned) after identifying ureters
- Removal of fallopian tubes (if opportunistic salpingectomy is performed)
- Transection of the utero-ovarian vessels (if ovaries are preserved)
- Division of the uterine vessels, cardinal ligaments, and uterosacral ligaments
- Incision of the vagina and excision of the specimen
- Closure of the vaginal cuff - with delayed absorbable sutures
Route Selection - Clinical Decision-Making
The surgical approach should be chosen based on:
- Uterine size and anatomy
- Underlying disease/indication
- Extent of expected adhesions
- Patient's wishes
- Surgeon's training and experience
ACOG/current guidance hierarchy:
- Vaginal hysterectomy - preferred when feasible (lowest morbidity)
- Laparoscopic hysterectomy - preferred over open when VH is not feasible
- Abdominal hysterectomy - reserved for cases where minimally invasive approaches are inappropriate
Remaining indications for open (laparotomy-based) hysterectomy include:
- Severe cardiopulmonary disease contraindicating general anesthesia or pneumoperitoneum
- Known or suspected uterine malignancy where morcellation would be required (contraindicated in malignancy)
- Severely distorted anatomy where minimally invasive approaches are deemed unsafe by experienced surgeons
- No access to surgeons/facilities for minimally invasive approaches
Complications
| Category | Specific Complications |
|---|---|
| Intraoperative | Hemorrhage, bladder injury, ureteral injury, bowel injury |
| Postoperative | Infection (wound, pelvic), VTE, vault hematoma, vaginal cuff dehiscence |
| Long-term | Vesicovaginal fistula (1 in 540 for abdominal, 1 in 896 for vaginal hysterectomy), pelvic floor disorders, sexual dysfunction, premature menopause (if oophorectomy) |
A 2025 meta-analysis (Chang OH et al., PMID 40120730) found associations between hysterectomy and pelvic floor disorders, reinforcing the importance of counseling patients about long-term pelvic floor consequences.
Concomitant Procedures
Opportunistic salpingectomy - removal of the fallopian tubes at the time of hysterectomy is now widely recommended (when oophorectomy is not planned) because high-grade serous ovarian carcinoma is thought to originate from the fimbriated end of the fallopian tube. Removing the tubes reduces future ovarian cancer risk without the premature menopausal effects of oophorectomy.
Special Considerations
- PREPARE mnemonic (Berek & Novak's): Before recommending hysterectomy for pain, discuss the Procedure, Reason/indication, Expectation, Preoperative workup, Alternatives (nonsurgical and surgical), Risks, and Expense with the patient
- Hysterectomy for CPP: ACOG requires at least 6 months of pelvic pain without correctable pathology before proceeding; a multidisciplinary approach (gynecologist + physical therapist + psychologist) reduced the frequency of hysterectomy from 16.3% to 5.8% in one study
- Cervical retention (subtotal hysterectomy): Leaves the cervix; proponents cite preserved sexual function and pelvic floor support, but evidence from prospective studies shows no statistically significant difference in urinary or sexual outcomes vs. total hysterectomy at 6 months
Key Evidence Updates (2024-2025)
- A 2024 systematic review (Mamik et al., PMID 38743951) reviewed hysterectomy techniques and outcomes specifically for benign large uteri, relevant when deciding between routes for bulky fibroids
- A 2025 meta-analysis (Chang et al., PMID 40120730) confirmed associations between hysterectomy and pelvic floor disorders - important for preoperative counseling
Sources: Berek & Novak's Gynecology (9th ed.); Sabiston Textbook of Surgery (21st ed.)
This is a shared conversation. Sign in to Orris to start your own chat.