Pulmonary thromboembolism
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is a thorough, well-structured overview of pulmonary thromboembolism:
Pulmonary Thromboembolism (PTE / PE)
Definition and Epidemiology
Pulmonary thromboembolism is the lodgment of thrombus (most commonly from deep venous thrombi) within the pulmonary arterial circulation. It is the third most common acute cardiovascular disease after coronary artery disease and stroke, with an annual clinically detected incidence of approximately 50 per 100,000. It causes roughly 100,000 deaths per year in the United States. Without anticoagulation treatment, mortality is approximately one-third of those diagnosed; with treatment, direct PE mortality falls to ~8%.
- Robbins & Kumar Basic Pathology, p. 93
- Grainger & Allison's Diagnostic Radiology, p. 381
Pathogenesis and Sources
Over 95% of venous emboli originate from deep vein thrombi in the leg veins proximal to the popliteal fossa, particularly the ilio-femoral system. They travel via the venous system through the right heart and lodge in the pulmonary vasculature.
Virchow's Triad governs VTE formation:
- Stasis (immobility, surgery, malignancy)
- Hypercoagulability (thrombophilia, pregnancy, OCP)
- Endothelial injury (trauma, catheters)
Anatomical distribution
| Location | Clinical implication |
|---|---|
| Main pulmonary artery or bifurcation ("saddle embolus") | Sudden death, massive PE |
| Medium-sized arteries | Obstruction without infarction (dual bronchial circulation) |
| Small end-arteriolar branches | Pulmonary infarction, hemorrhage |
Below is a gross pathology specimen showing a thrombus lodged in a pulmonary artery branch (derived from lower-extremity DVT):

Fig. 3.15 - Embolus derived from a lower-extremity DVT lodged in a pulmonary artery branch (Robbins & Kumar Basic Pathology)
Pathophysiology
- At least 30-50% of the pulmonary vascular bed must be obstructed to significantly raise pulmonary artery pressure (PAP).
- Humoral factors (serotonin, thromboxane A2) and reflex vasoconstriction also contribute.
- Abrupt rise in pulmonary vascular resistance → right ventricular (RV) dilatation → RV pressure overload → RV failure (primary cause of death in severe PE).
- Paradoxical embolism can occur when venous emboli cross an atrial or ventricular septal defect and enter systemic circulation.
Consequences by size:
- 60-80% of emboli: small, clinically silent; organize and incorporate into vascular wall (may leave fibrous webs).
- Large embolus occluding major pulmonary artery: sudden death.
- Medium-sized: ischemia without infarction (preserved bronchial artery flow); but if left-heart failure co-exists, infarction may occur.
- Recurrent emboli: progressive pulmonary hypertension → cor pulmonale.
Risk Factors
| Category | Examples |
|---|---|
| Age | Risk almost doubles each decade after age 40 |
| Previous VTE | Major predictor of recurrence |
| Malignancy | Active cancer (especially mucin-secreting) |
| Immobilization | Prolonged bed rest, long flights |
| Surgery | Especially orthopedic (hip/knee) |
| Hypercoagulable states | Factor V Leiden, protein C/S deficiency, antiphospholipid syndrome |
| Hormonal | OCP, HRT, pregnancy/postpartum (risk 2-4x higher) |
| Instrumentation | Indwelling venous catheters |
Clinical Presentation
Classical triad (present in minority): sudden chest pain + dyspnea + hemoptysis.
More common presentations:
- Pleuritic chest pain, tachypnea, dyspnea (most common)
- Cough, tachycardia (HR >100), fever
- Signs of DVT (leg swelling, tenderness)
- Syncope (suggests massive PE with hemodynamic compromise)
- Shock, hypotension, or cardiac arrest (severe/massive PE)
Classification by Severity
| Class | Definition | Key Features |
|---|---|---|
| Massive (High-Risk) | Sustained hypotension/shock (SBP <90 mmHg) | RV failure, high mortality |
| Submassive (Intermediate-Risk) | Normotensive + RV dysfunction or myocardial injury | Echo: RV strain; Troponin/BNP elevated |
| Low-Risk (Non-massive) | Normotensive, no RV dysfunction | Good prognosis with anticoagulation |
- Miller's Anesthesia, p. 5028
Diagnosis
Step 1: Pre-test Probability (Wells Score)
| Variable | Original | Simplified |
|---|---|---|
| Previous PE or DVT | 1.5 | 1 |
| Heart rate >100 bpm | 1.5 | 1 |
| Surgery or immobilization <4 weeks | 1.5 | 1 |
| Hemoptysis | 1 | 1 |
| Active cancer | 1 | 1 |
| Clinical signs of DVT | 1 | 1 |
| Alternative diagnosis less likely than PE | 3 | 1 |
| PE unlikely | ≤4 | ≤1 |
| PE likely | >4 | >1 |
- Grainger & Allison's Diagnostic Radiology, p. 381
Step 2: D-Dimer Testing
- Very high negative predictive value (NPV) - a negative D-dimer with low/intermediate pre-test probability safely excludes PE in up to 51% of outpatients.
- Age-adjusted D-dimer cut-off above age 50: age × 10 μg/L (instead of standard 500 μg/L) - improves specificity while maintaining sensitivity.
- Positive D-dimer is non-specific (elevated with inflammation, surgery, trauma, malignancy, pregnancy).
- A negative D-dimer does NOT have 100% NPV and cannot absolutely exclude PE.
Step 3: Imaging
CT Pulmonary Angiography (CTPA) - first-line imaging:
- Sensitivity: 83% (PIOPED II), Specificity: 96%
- Negative predictive value: 95-99%
- Requires adequate pulmonary arterial enhancement (≥300-350 HU)
- RV/LV ratio ≥1 on CTPA = independent predictor of adverse outcome
- Anticoagulation can be safely withheld with a negative CTPA (if concordant with clinical probability)
V/Q Scintigraphy:
- Most useful in outpatients without known cardiopulmonary disease with a normal CXR
- Preferred in young patients (less radiation), pregnant patients
- Normal perfusion scan effectively excludes PE
- High-probability scan is 97% specific (PIOPED I)
Compression Ultrasound (CUS):
- Proximal DVT on CUS is sufficient to initiate anticoagulation without further imaging
ECG & ABG:
- Not diagnostic; useful to exclude MI, arrhythmia
- ECG: sinus tachycardia most common; S1Q3T3, RBBB, RV strain in massive PE
- ABG: hypoxemia, reduced PaCO2, widened A-a gradient
Below is a coronal CT reconstruction showing coexisting acute (yellow arrow) and chronic pulmonary emboli (blue arrows):
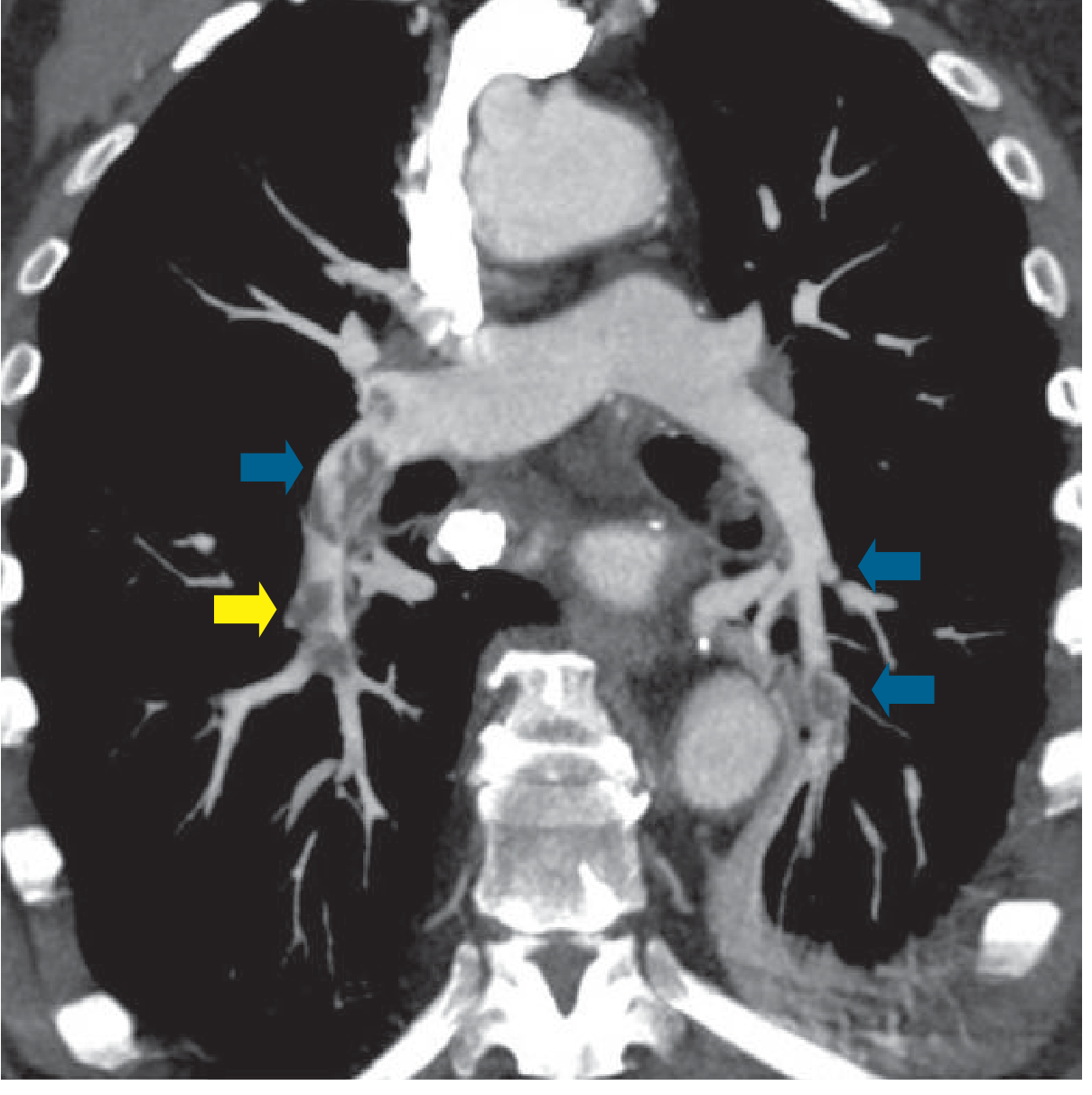
Fig. 16.36 - Coronal CT reconstruction showing both acute (yellow) and chronic (blue) pulmonary embolism (Grainger & Allison's Diagnostic Radiology)
Treatment
Initial Management
- Airway and oxygen support
- Hemodynamic resuscitation (vasopressors if shocked)
- Anticoagulation is the cornerstone of therapy in all risk groups
Anticoagulation Options
Initial phase (first 5-10 days):
- Low-molecular-weight heparin (LMWH) - preferred (e.g., enoxaparin 1 mg/kg SC q12h)
- Unfractionated heparin (UFH) - IV drip; preferred if renal failure, thrombolysis anticipated, or hemodynamically unstable
- Fondaparinux - subcutaneous, factor Xa inhibitor
Long-term phase:
- DOACs (rivaroxaban, apixaban, edoxaban, dabigatran) - now standard of care for most patients
- Warfarin with INR 2.0-3.0 (with bridging heparin)
- LMWH in pregnancy (does not cross placenta; warfarin is teratogenic)
Advanced Therapies (Massive and High-Risk Submassive PE)
| Therapy | Indication | Notes |
|---|---|---|
| Systemic thrombolysis (tPA, streptokinase) | Massive PE with shock/cardiac arrest | High bleeding risk; avoid if contraindicated |
| Catheter-directed thrombolysis (CDT) | Submassive PE; contraindication to systemic lysis | Lower dose thrombolytic via catheter |
| Mechanical thrombectomy | Massive PE; contraindication to thrombolysis | Emerging data vs. CDT (meta-analysis, 2025) |
| Surgical embolectomy | Central PE, failed thrombolysis | Open surgery, cardiopulmonary bypass |
| VA-ECMO | Refractory cardiogenic shock | Bridge to definitive therapy |
| IVC filter | Anticoagulation contraindicated/recurrent PE | Retrievable filters preferred; rare indications |
PE Response Teams (PERT): Multidisciplinary teams (pulmonology, interventional cardiology, cardiac surgery, IR) assessing optimal management strategy in real-time - particularly for submassive PE.
Duration of Anticoagulation
| Scenario | Duration |
|---|---|
| Provoked PE (transient risk factor) | 3 months |
| Unprovoked PE, first episode | At least 3-6 months; consider extended therapy |
| Recurrent unprovoked PE | Indefinite |
| Active malignancy | Indefinite or until cancer resolved (LMWH/DOAC) |
Complications
Pulmonary Infarction
- Occurs when dual circulation is overwhelmed (usually with pre-existing cardiopulmonary disease)
- Hampton's hump on CXR (wedge-shaped pleural-based opacity)
Chronic Thromboembolic Pulmonary Hypertension (CTEPH)
- Occurs in up to 4% of patients with acute PE (typically within 2 years)
- Paradoxically, ~50% of CTEPH patients have no clinical history of acute PE
- Presents with progressive dyspnea, RV failure
- Diagnosis: V/Q scintigraphy (screening) → CTPA/conventional pulmonary angiography confirms
Treatment of CTEPH:
-
Pulmonary thromboendarterectomy (PTE surgery) - treatment of choice for surgically accessible (proximal) disease
-
Balloon pulmonary angioplasty (BPA) - for inoperable or distal disease
-
Medical therapy (riociguat, macitentan) for inoperable/residual CTEPH
-
Grainger & Allison's Diagnostic Radiology, p. 388
Key Summary Points
-
95% of PEs originate from DVT in proximal leg veins - they share the same risk factors and pathophysiology (VTE spectrum).
- 60-80% of emboli are clinically silent; massive PE causes sudden death.
- Low/intermediate Wells score + negative D-dimer safely rules out PE.
- CTPA is the gold-standard first imaging test; V/Q scan is preferred in pregnancy and young patients.
- Anticoagulation is universal; choice of agent depends on severity, renal function, pregnancy, and bleeding risk.
- Systemic thrombolysis is reserved for massive PE; CDT/mechanical thrombectomy for selected submassive cases.
- CTEPH is a serious delayed complication requiring long-term follow-up after acute PE.
Recent evidence note: A 2024 meta-analysis (PMID 39267429) confirmed that anticoagulation is comparable to thrombolytic therapy in overall outcomes for most PE patients, supporting current guidelines favoring anticoagulation first. A July 2025 meta-analysis (PMID 40269600) compared mechanical thrombectomy vs. catheter-directed thrombolysis in PE, showing similar outcomes - evidence informing evolving interventional strategies.
This is a shared conversation. Sign in to Orris to start your own chat.