Autopeep for md Anaesthesia exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I have everything needed for a comprehensive exam-ready answer. Here it is:
Auto-PEEP (Intrinsic PEEP) — MD Anaesthesia Exam Notes
Definition
Auto-PEEP (also called intrinsic PEEP, iPEEP) is positive alveolar pressure present at end-exhalation above any externally applied PEEP, caused by incomplete lung emptying before the next breath begins.
"Intrinsic PEEP is any additional end-expiratory pressure beyond what is applied to the patient." — Barash Clinical Anaesthesia, 9e
Pathophysiology
Auto-PEEP arises when exhalation is not completed before the next inspiratory cycle. The key determinant is the expiratory time constant (τ):
τ = Resistance (R) × Compliance (C)
Three time constants are required for ~95% lung emptying. If the next breath interrupts exhalation before this, residual volume and pressure accumulate — dynamic hyperinflation.
Two mechanisms:
| Mechanism | Example |
|---|---|
| Increased expiratory time constant (high R or high C) | Asthma (↑R), COPD (↑C) |
| Expiratory flow limitation (airway collapse) | Obesity, mucous plugging |
Numerical example (Barash): If R = 10 cmH₂O/L/s and C = 0.05 L/cmH₂O → τ = 0.5 s → need ~1.5 s for full exhalation.
Causes / Risk Factors
| Category | Factors |
|---|---|
| Increased resistance | Asthma, bronchospasm, COPD, secretions, kinked or small ETT |
| Increased compliance | COPD emphysema |
| Ventilator settings | ↓Expiratory time (high RR, long I:E ratio), ↑Tidal volume |
| Active expiration | Persistent inspiratory muscle activity during exhalation |
| External resistance | HME filters, narrow tubing |
Detection / Measurement
1. Flow–Time Waveform (most practical)
The flow trace does not return to zero before the next breath — a non-zero end-expiratory flow indicates ongoing alveolar emptying (= auto-PEEP present).
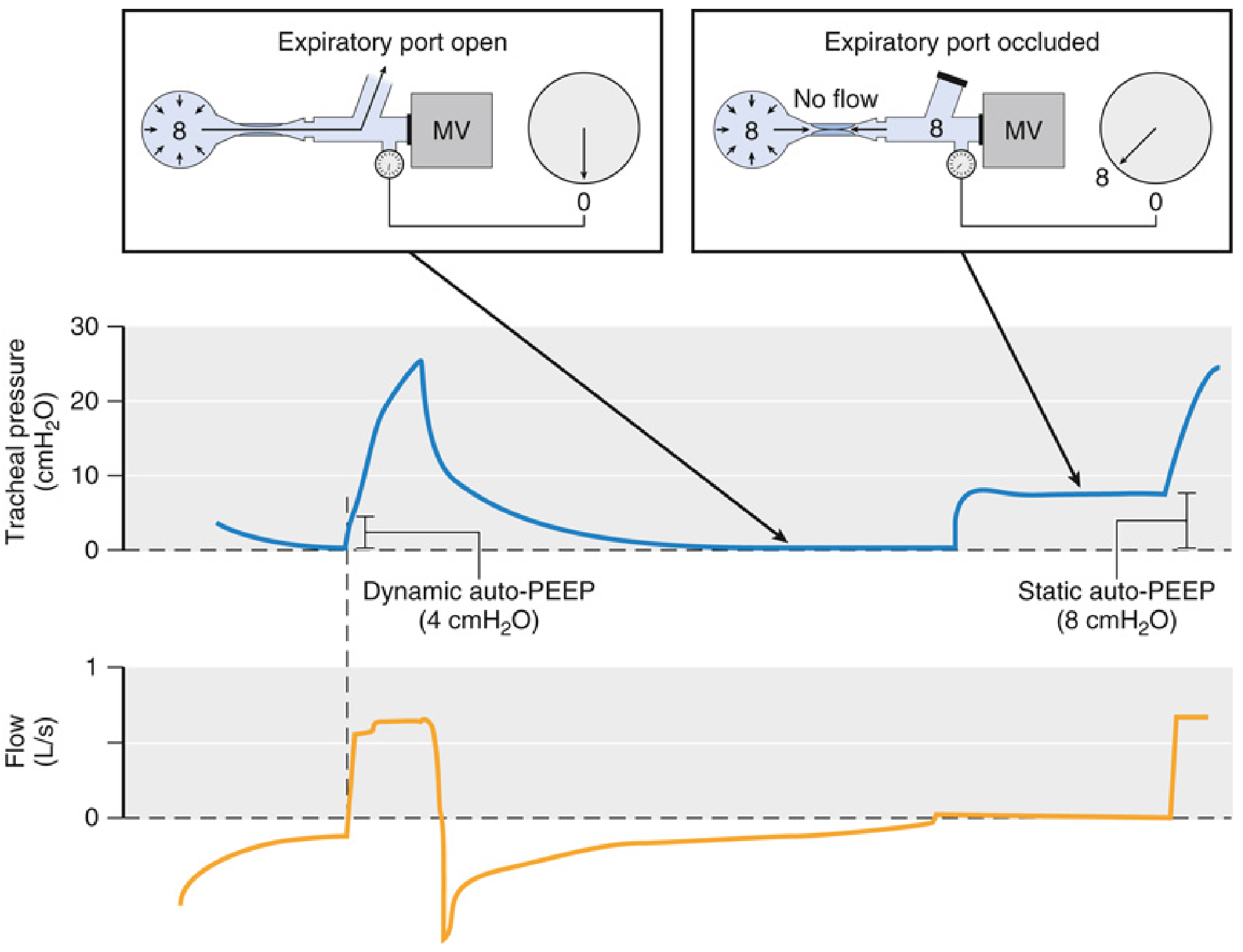
2. Dynamic Auto-PEEP
Tracheal pressure at the moment when the flow trace crosses zero during exhalation (expiratory port open). Underestimates true auto-PEEP in heterogeneous lungs (some alveoli are isolated by airway closure).
3. Static Auto-PEEP (Gold Standard)
Expiratory hold / occlusion manoeuvre: Occlude the expiratory port at end-exhalation for ≤4 seconds and observe the pressure rise to a plateau. Auto-PEEP = plateau pressure − applied PEEP.
Requires passive patient (no spontaneous effort). Active breathing invalidates this measurement. Oesophageal balloon manometry can assess auto-PEEP in spontaneously breathing patients.
4. Other signs
- Unexpected ↑ peak airway pressure and plateau pressure
- Apparent ↓ respiratory system compliance
- Haemodynamic compromise (hypotension, ↓ cardiac output)
- Ventilator dyssynchrony / "missed" trigger attempts
Haemodynamic Consequences
Auto-PEEP → ↑ intrathoracic pressure → ↓ venous return → ↓ preload → ↓ cardiac output and hypotension. This is especially dangerous at induction in asthmatics/COPD patients.
"With severe intrinsic PEEP, increased intra-thoracic pressure reduces venous return and lowers cardiac output." — Murray & Nadel's Respiratory Medicine
Management
A. Address the Ventilator Settings (first-line)
| Strategy | Rationale |
|---|---|
| ↓ Respiratory rate | ↑ Expiratory time |
| ↑ Inspiratory flow rate | Shortens inspiration → more time for expiration |
| ↓ I:E ratio (e.g., 1:3 or 1:4) | Lengthens expiratory phase |
| ↓ Tidal volume | Less volume to exhale |
| Permissive hypercapnia | Accept ↑ PaCO₂ to allow adequate expiratory time |
B. Treat the Underlying Cause
- Bronchodilators (β₂-agonists, anticholinergics) for bronchospasm
- Suction / physiotherapy to clear secretions
- Treat bronchospasm: in mechanically ventilated asthmatics → ketamine (bronchodilation + sedation) is preferred
C. Applied (Extrinsic) PEEP to Counter-Balance iPEEP
In spontaneously breathing patients on assisted modes (e.g., PSV), patients must generate effort equal to auto-PEEP before the ventilator triggers — causing increased work of breathing and missed triggers.
Applying extrinsic PEEP up to ~80% of intrinsic PEEP reduces triggering effort without increasing end-expiratory lung volume (EELV), because EELV only rises when extrinsic PEEP exceeds intrinsic PEEP. — Miller's Anaesthesia 10e
⚠️ In passive/controlled ventilation, adding extrinsic PEEP does NOT reduce auto-PEEP and will worsen hyperinflation — avoid this approach.
D. Emergency — Acute Haemodynamic Collapse
Disconnect the patient from the ventilator and allow passive exhalation ("the ventilator disconnect test"). This immediately relieves hyperinflation and restores venous return.
Auto-PEEP in Specific Anaesthesia Scenarios
| Scenario | Key Point |
|---|---|
| Status asthmaticus on MV | Reduce RR, accept hypercapnia; ketamine for sedation; extrinsic PEEP below iPEEP |
| COPD | High compliance + dynamic airway collapse = major risk; use expiratory hold to quantify |
| Induction of anaesthesia | May cause sudden hypotension at initiation of IPPV in obstructed patients — disconnect if BP collapses |
| One-lung ventilation | Isolated lung with dependent position and reduced expiratory time — high risk |
| Dynamic parameters (SVV/PPV) | Auto-PEEP >15 cmH₂O invalidates SVV/PPV as predictors of fluid responsiveness |
Exam Summary Box
| Definition | End-expiratory alveolar pressure > applied PEEP |
| Mechanism | Incomplete exhalation due to ↑τ or flow limitation |
| At-risk | Asthma, COPD, high RR, ↑VT, ↓I:E |
| Detect | Non-zero end-expiratory flow; expiratory hold |
| Consequences | ↑Paw, ↓compliance, ↓CO, hypotension, barotrauma |
| Fix (ventilator) | ↓RR, ↑flow rate, ↓VT, ↑I:E ratio |
| Fix (spontaneous) | Extrinsic PEEP < iPEEP to ease triggering |
| Emergency | Disconnect ventilator |
Sources: Barash Clinical Anaesthesia 9e; Miller's Anaesthesia 10e; Murray & Nadel's Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.