Dysplastic hip in adults
Reading File
Finding Sources
Searching PubMed
"hip dysplasia" AND adults AND treatment
Searching the Web
adult hip dysplasia diagnosis management periacetabular osteotomy 2024
Reading File
Reading File
Reading File
Reading Article
PMID: 38919352
Reading Article
PMID: 37306161
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive content from Campbell's, Bailey & Love, and Rheumatology textbooks, plus current PubMed evidence. Let me compile the full answer.
Dysplastic Hip in Adults
Definition and Background
Hip dysplasia in adults describes inadequate coverage of the femoral head by the acetabulum - resulting from residual developmental dysplasia of the hip (DDH) or, less frequently, from Legg-Calvé-Perthes disease. Most patients become symptomatic between their second and fifth decades of life, though mild cases may not present until the teenage years or early adulthood. Hip dysplasia is now recognized as a cause of hip osteoarthritis (OA) in 20-40% of patients who eventually need total hip replacement. - Rheumatology 2-Volume Set (2022), p. 82.8
Pathomechanics
In a dysplastic hip, the acetabulum slopes excessively vertically (excessive valgus angulation), and the femoral neck usually has increased valgus and excessive anteversion. The femoral head sits laterally in a shallow socket, so the labrum becomes part of the weight-bearing surface. This creates:
- Increased contact pressures at the lateral acetabular rim
- Progressive labral tears (labral tears are a common feature in both subtle and severe dysplasia)
- Chondral delamination and ulceration
- Secondary osteoarthritis if untreated
A key study by Thomas et al. (20-year longitudinal) found that for each degree of reduction in the LCE angle below 28°, there was a 14% increase in risk of developing secondary OA. Murphy et al. found that contralateral hips with LCE <16° routinely developed significant OA by age 65. - Campbell's Operative Orthopaedics 15th Ed, p. 447
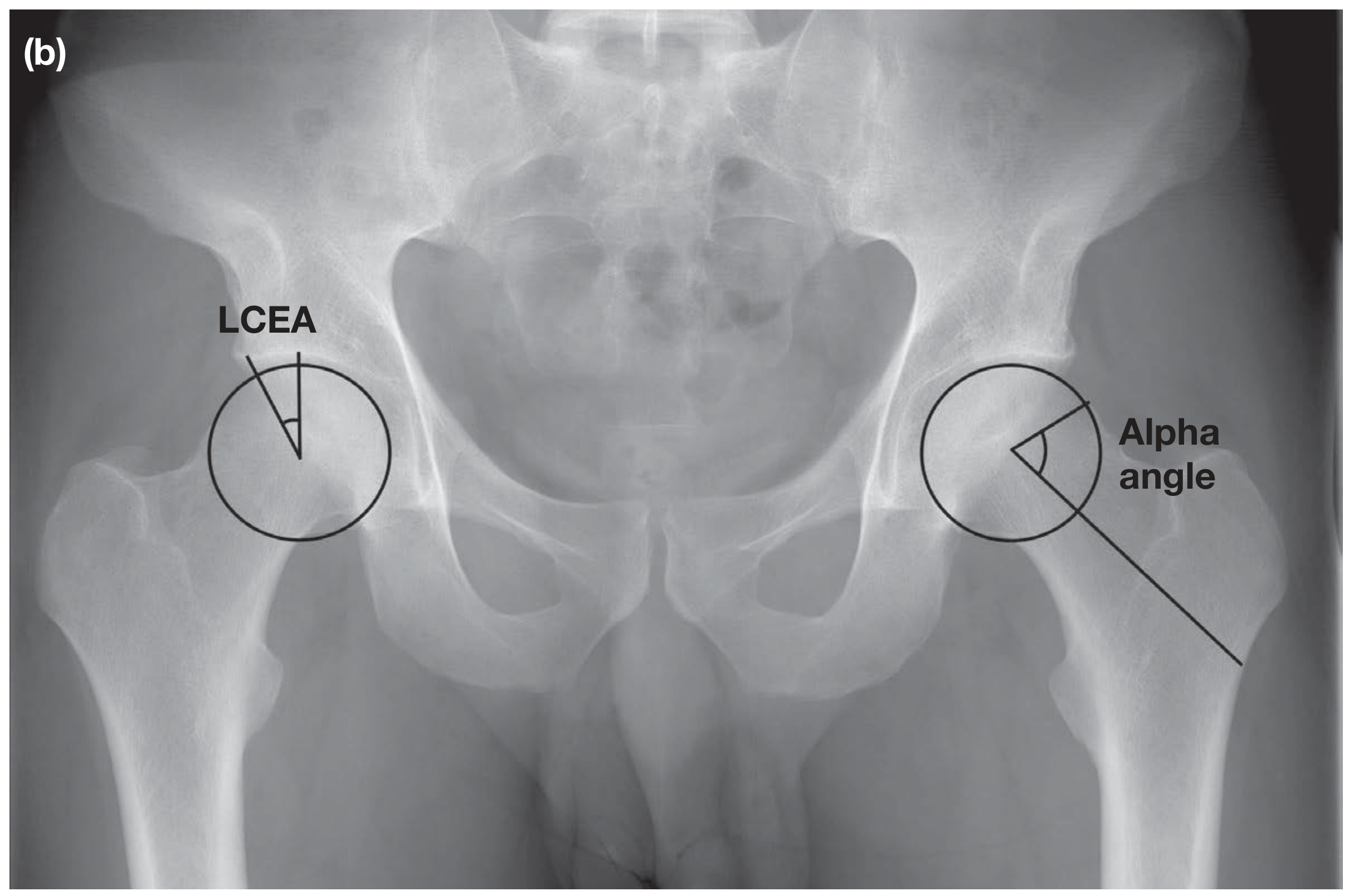
Radiographic Diagnosis
Standard AP pelvis radiograph is the primary screening tool.
Key radiographic measurements:
| Parameter | Normal | Borderline Dysplasia | Dysplasia |
|---|---|---|---|
| Lateral Center-Edge Angle (LCEA/LCE) of Wiberg | >25° | 20-25° | <20° |
| Tönnis angle (acetabular index) | <10° | - | >10° |
| Alpha angle | ≤55° | - | Often elevated (cam morphology in 10-40%) |
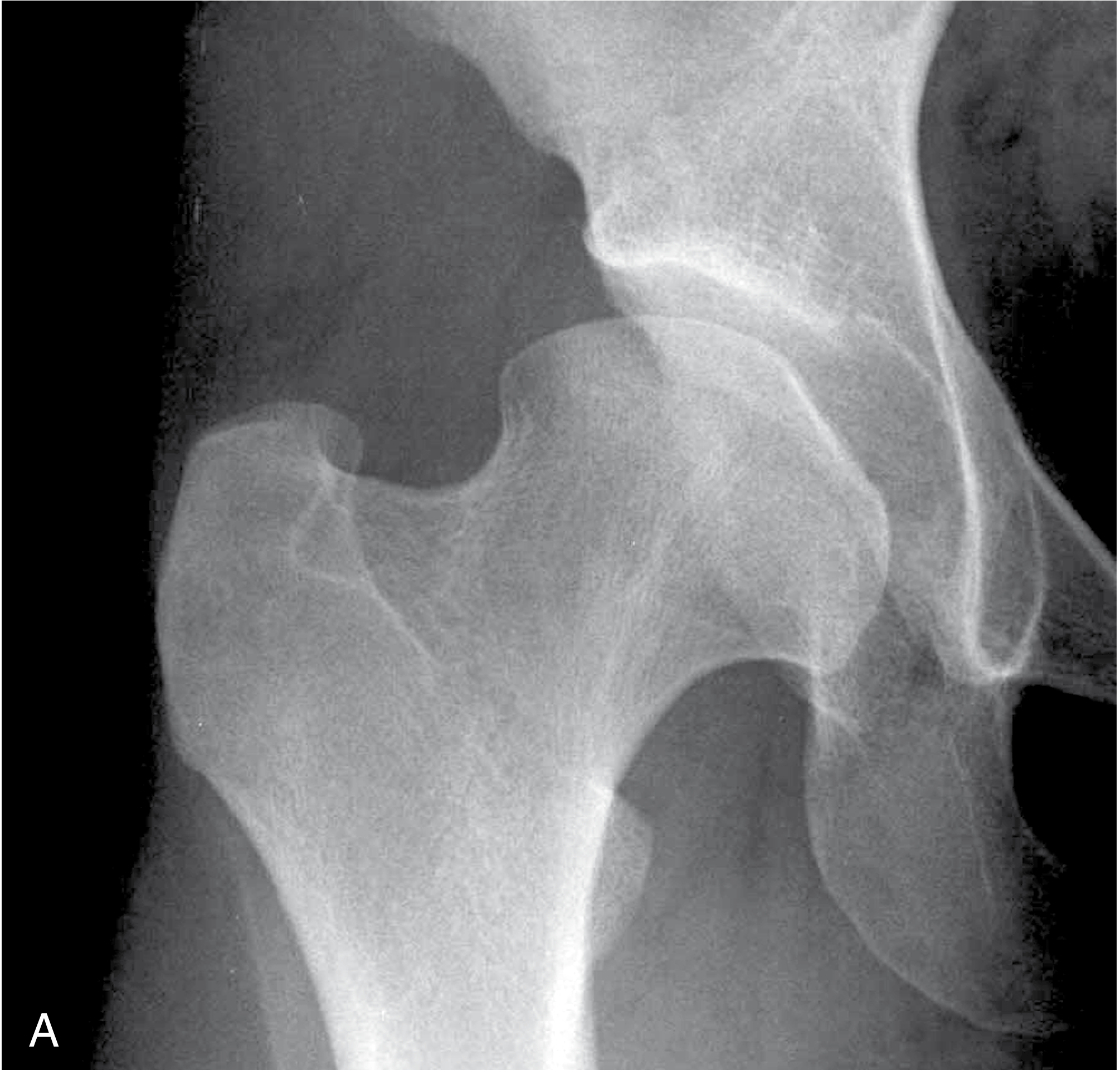
Additional radiographic findings:
- Increased Tönnis angle
- Lateralized hip center with broadened radiographic teardrop
- Increased femoral neck-shaft angle with excessive anteversion
- Small femoral head with flattened lateral contour
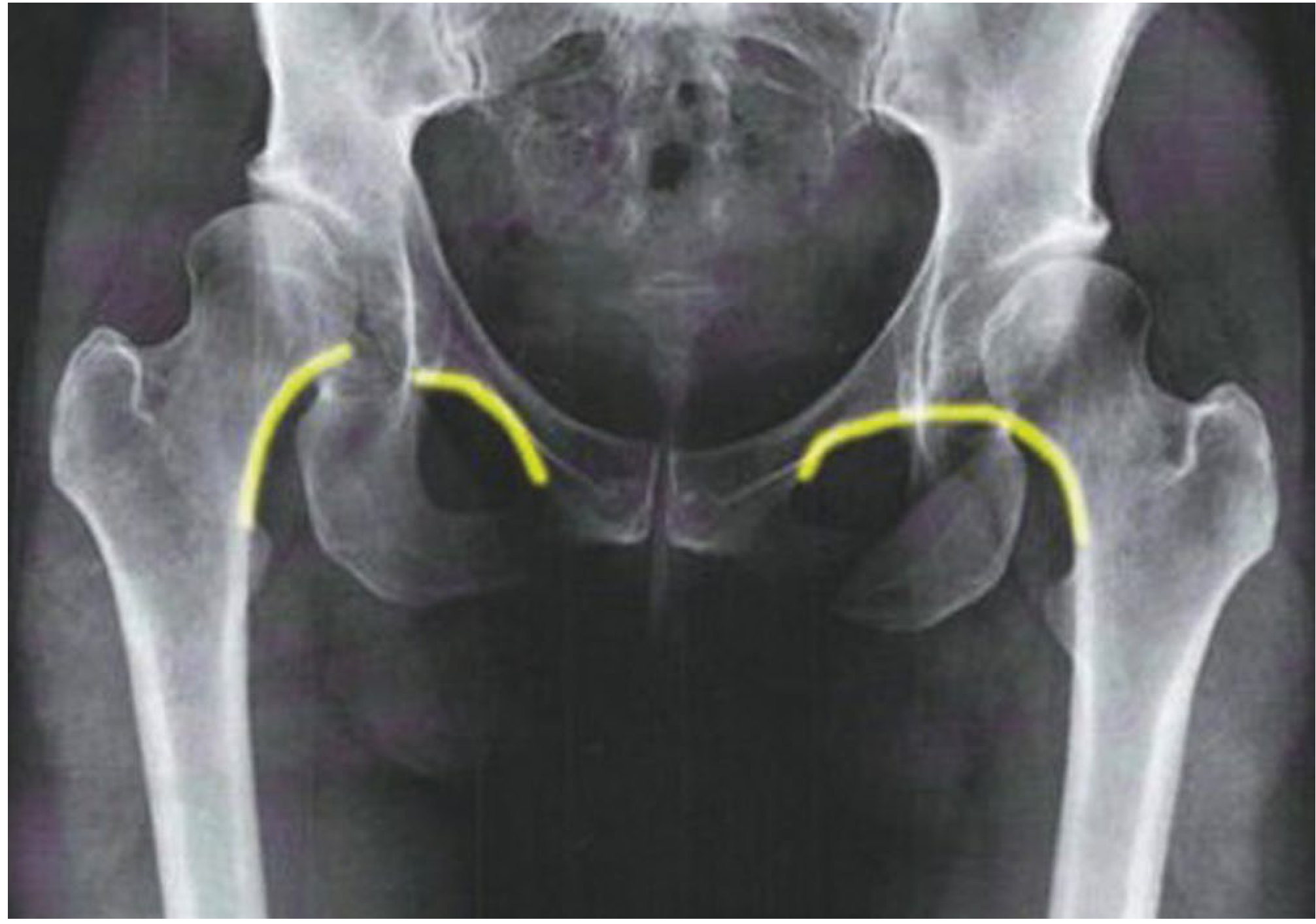
- Disruption of Shenton's line - indicates superior subluxation of the femoral head (more severe dysplasia)
False-profile view: Provides the vertical center-anterior (VCA) angle to assess anterior femoral head coverage and sagittal version.
Clinical Assessment
History: Groin pain worsened with activity, prolonged standing, pivoting sports. Initially only with high-stress activities.
Examination:
- FADIR test (Flexion, ADduction, Internal Rotation) - positive when labral injury present
- Apprehension test - positive with insufficient anterior coverage/anterior cartilage injury
- Trendelenburg gait in more severe cases
- Reduced internal rotation
Imaging Workup (Campbell's Protocol)
A structured pre-operative evaluation includes:
- AP pelvis + false-profile radiograph - assess LCEA, Tönnis angle, Shenton line, femoral head sphericity
- Abduction/flexion AP view - simulates the congruence that would be attained with PAO (helps decide if PAO is appropriate)
- MR arthrogram - gold standard for labral and articular cartilage status
- Low-dose CT pelvis (with knee slices) - assess acetabular version and femoral neck version
- 3D CT when complex deformity is present
Treatment Options
Treatment is tailored to the degree of dysplasia, severity of OA (Tönnis grade), patient age, femoral head sphericity, and functional status.
1. Non-operative Management
- Analgesia (NSAIDs, activity modification)
- Physiotherapy: core and hip strengthening, proprioception
- Intra-articular corticosteroid injection for symptom relief
- Reserved for those unwilling or unfit for surgery, or as a temporizing measure
2. Periacetabular Osteotomy (PAO) - The Bernese PAO
The primary surgical option for skeletally mature patients with symptomatic dysplasia and preserved or near-preserved articular cartilage (Tönnis grade 0-1).
Mechanism: A series of bony cuts around the acetabulum frees it as a fragment, which is then reoriented (laterally and anteriorly) to improve femoral head coverage, reducing joint contact pressure. The posterior column remains intact (ischium attached to axial skeleton), which:
- Preserves excellent rotational freedom
- Minimizes osteonecrosis risk of the acetabular segment
- Allows relatively rapid mobilization
- Does not compromise future THA (no acetabular bone stock loss)
Approach: Smith-Petersen (direct anterior); screw fixation of the repositioned fragment.
Indications:
- LCEA <20° (definite dysplasia) with symptoms and no/mild OA
- Selected patients with borderline dysplasia (LCEA 20-24°) + labral pathology
- Age typically <40, but evidence supports use in selected patients >40 with Tönnis 0-1
Simultaneous procedures:
- Arthroscopic labral repair/central compartment management
- Femoral osteochondroplasty (if cam morphology creates risk of post-PAO FAI)
- Intertrochanteric varus-derotational osteotomy (for severe valgus/anteversion of the proximal femur)
2024 Systematic Review (O'Connor et al., PMID 38919352): 335 hips in patients >40 years (mean age 43.5-47.2 years). PAO survivorship ranged from 67-100%. Complications in 2-36% with no lasting effects. Conclusion: PAO should be considered for patients >40 without hip arthritis, but with very selective indications. - Iowa Orthopaedic Journal 2024
2024 Meta-analysis (O'Brien et al., PMID 37306161): 62 studies, 5017 participants. PAO produces significant improvements in pain (SPD 1.35 at 1 year), function (SPD 1.22 at 1 year), and QOL (SPD 1.36 at 1 year). Outcomes do not fully normalize to healthy controls but improve substantially. - Hip International 2024
3. Hip Arthroscopy
- For borderline dysplasia (LCEA 20-24°) when FAI coexists and instability concerns are absent
- Labral repair, chondral debridement, cam resection
- Predictors of poor outcome: severe acetabular chondral damage, labral damage, femoral head cartilage damage
- Caution: arthroscopy alone in true dysplasia (LCEA <20°) can worsen instability
4. Total Hip Arthroplasty (THA)
- For advanced OA (Tönnis grade 2-3), usually in patients >50 or when PAO is contraindicated
- Technical challenges: shallow acetabulum (poor cup fixation), deficient bone stock, excessive anteversion, horizontal/oblique acetabular orientation
- Prior PAO does not worsen THA outcomes - retrospective multicenter data showed no significant differences in complications, revision rates, or Harris Hip Scores between THA performed after prior PAO vs. THA without prior PAO
- THA after PAO should use the same Smith-Petersen approach to avoid biomechanical compromise
Tönnis Grading of OA (guides surgical decision-making)
| Grade | Radiographic Features |
|---|---|
| 0 | No signs of OA |
| 1 | Increased sclerosis, slight joint space narrowing, small osteophytes |
| 2 | Small cysts, moderate joint space narrowing, moderate head deformity |
| 3 | Large cysts, severe narrowing or obliteration, severe head deformity |
PAO is generally indicated for Tönnis 0-1. Grade 2 is a relative contraindication; Grade 3 is an indication for THA.
Natural History if Untreated
- LCE angle <16°: routinely develops significant OA by age 65
- Each 1° reduction below 28° = 14% increased OA risk
- The labrum hypertrophies as a compensatory mechanism but eventually tears under overload
- Untreated dysplasia accounts for up to 40% of all hip OA cases
Summary Algorithm
Adult hip pain + shallow acetabulum (LCEA <25°)
↓
Full imaging workup (X-ray, false-profile, MRA, CT)
↓
Assess Tönnis grade + femoral head sphericity + age
↓
Tönnis 0-1, age <50, spherical head → PAO ± arthroscopy
Tönnis 0-1, borderline (LCEA 20-24°) + FAI → Arthroscopy
Tönnis 2-3, age >50, advanced OA → THA
Non-operative → physiotherapy, NSAIDs (any grade, temporizing)
Sources
- Campbell's Operative Orthopaedics 15th Ed (2026), Chapter 7 (Hip Dysplasia in Young Adults), pp. 445-455
- Bailey and Love's Short Practice of Surgery 28th Ed, Chapter 39 (Hip dysplasia in young adults), p. 575
- Rheumatology 2-Volume Set (2022, Elsevier), Chapter 82, p. 82.8
- O'Connor KP et al. "Hip Dysplasia Treated With Periacetabular Osteotomy in Patients Over 40 Years Old." Iowa Orthop J 2024. PMID 38919352
- O'Brien MJ et al. "Pain, function and quality of life are impaired in adults undergoing PAO for hip dysplasia: a systematic review and meta-analysis." Hip Int 2024. PMID 37306161
- O'Connor KP et al. "Prevalence of Radiographic Hip Dysplasia in the General Adult Population." Iowa Orthop J 2024. PMID 38919354
This is a shared conversation. Sign in to Orris to start your own chat.