First second and third week of development embryology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have rich, comprehensive content from The Developing Human: Clinically Oriented Embryology. Let me compile the full, detailed answer.
Embryology: First, Second, and Third Weeks of Development
Source: The Developing Human: Clinically Oriented Embryology
WEEK 1 - Fertilization, Cleavage, and Early Implantation
Overview
Human development begins at fertilization when a sperm fuses with a secondary oocyte to form the zygote - a totipotent, diploid cell that is the biological beginning of a unique individual.
Gametogenesis (Background)
- Spermatogenesis: Occurs in the testes. One primary spermatocyte produces 4 functional sperms, each with 23 chromosomes (haploid).
- Oogenesis: Occurs in the ovaries. One primary oocyte produces 1 mature oocyte + 3 polar bodies (which degenerate). The oocyte conserves cytoplasm - hence it is a large cell.
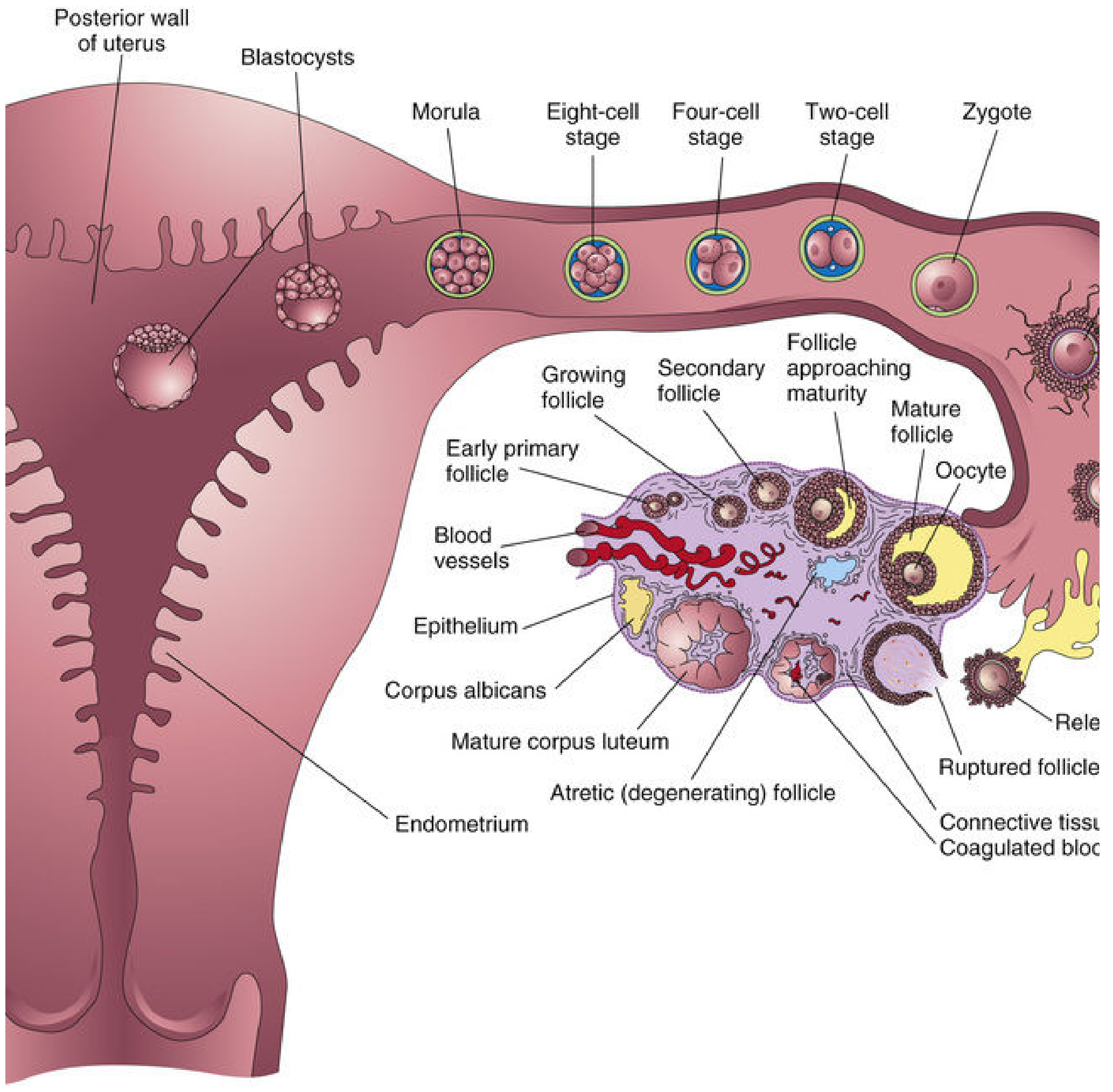
Ovulation
- One oocyte is expelled from the ovary at ovulation (secondary oocyte, arrested in metaphase II).
- The fimbriae of the uterine tube sweep the oocyte into the ampulla (the usual site of fertilization).
Fertilization (Day 0)
Occurs in the ampulla of the uterine tube. Steps:
- Hundreds of sperms reach the uterine tubes; capacitation occurs during transit (6-8 hours in female tract).
- Sperm penetrates the corona radiata and binds to the zona pellucida via the ZP3 glycoprotein receptor.
- The acrosome reaction releases enzymes (hyaluronidase, acrosin), allowing sperm to penetrate the zona.
- Sperm head fuses with the oocyte plasma membrane - this triggers:
- The cortical reaction (cortical granule release) - hardens zona pellucida to prevent polyspermy
- The oocyte completes meiosis II, forming the mature oocyte + second polar body
- The sperm head enlarges to form the male pronucleus; the oocyte nucleus becomes the female pronucleus.
- Fertilization is complete when the two pronuclei unite (syngamy) and chromosomes intermingle during metaphase of the first mitotic division.
Results of fertilization:
- Restores diploid chromosome number (46)
- Determines biological sex (X or Y from sperm)
- Initiates cleavage
- Each individual becomes genetically unique
Cleavage (Days 2-3)
As the zygote travels through the uterine tube toward the uterus, it undergoes cleavage - rapid mitotic divisions into progressively smaller cells called blastomeres (no increase in total size, as cells are still enclosed by the zona pellucida).
| Stage | Timeline | Description |
|---|---|---|
| Zygote | Day 0 | Single totipotent cell |
| 2-cell stage | Day 1-2 | First cleavage |
| 4-cell stage | Day 2 | Second cleavage |
| 8-cell stage | Day 2-3 | Compaction begins (cells flatten, gap junctions form) |
| Morula | Day 3-4 | ~12-32 blastomeres, enters uterus |
| Blastocyst | Day 4-5 | Fluid accumulates, cavity forms |
Blastocyst Formation (Days 4-5)
A fluid-filled cavity (blastocystic cavity/blastocoele) forms within the morula, converting it into a blastocyst:
- Embryoblast (inner cell mass, ICM): cluster of cells at one pole - gives rise to the embryo proper and some extraembryonic membranes
- Trophoblast: outer cell layer - forms the placenta and extraembryonic structures
- Blastocystic cavity: fluid-filled space
At 4-5 days: the zona pellucida is shed (hatching). This allows the trophoblast to contact and attach to the endometrium.
Implantation Begins (Days 5-6)
- The blastocyst attaches to the posterior wall of the uterus (the usual site) via its embryonic pole.
- The trophoblast at the embryonic pole begins differentiating into two layers: cytotrophoblast (inner) and syncytiotrophoblast (outer).
- By end of week 1, implantation has just started.
WEEK 2 - Completion of Implantation, Bilaminar Disc
The second week is often called the "Week of 2s" - 2 trophoblast layers, 2 embryoblast layers (bilaminar disc), 2 cavities form.
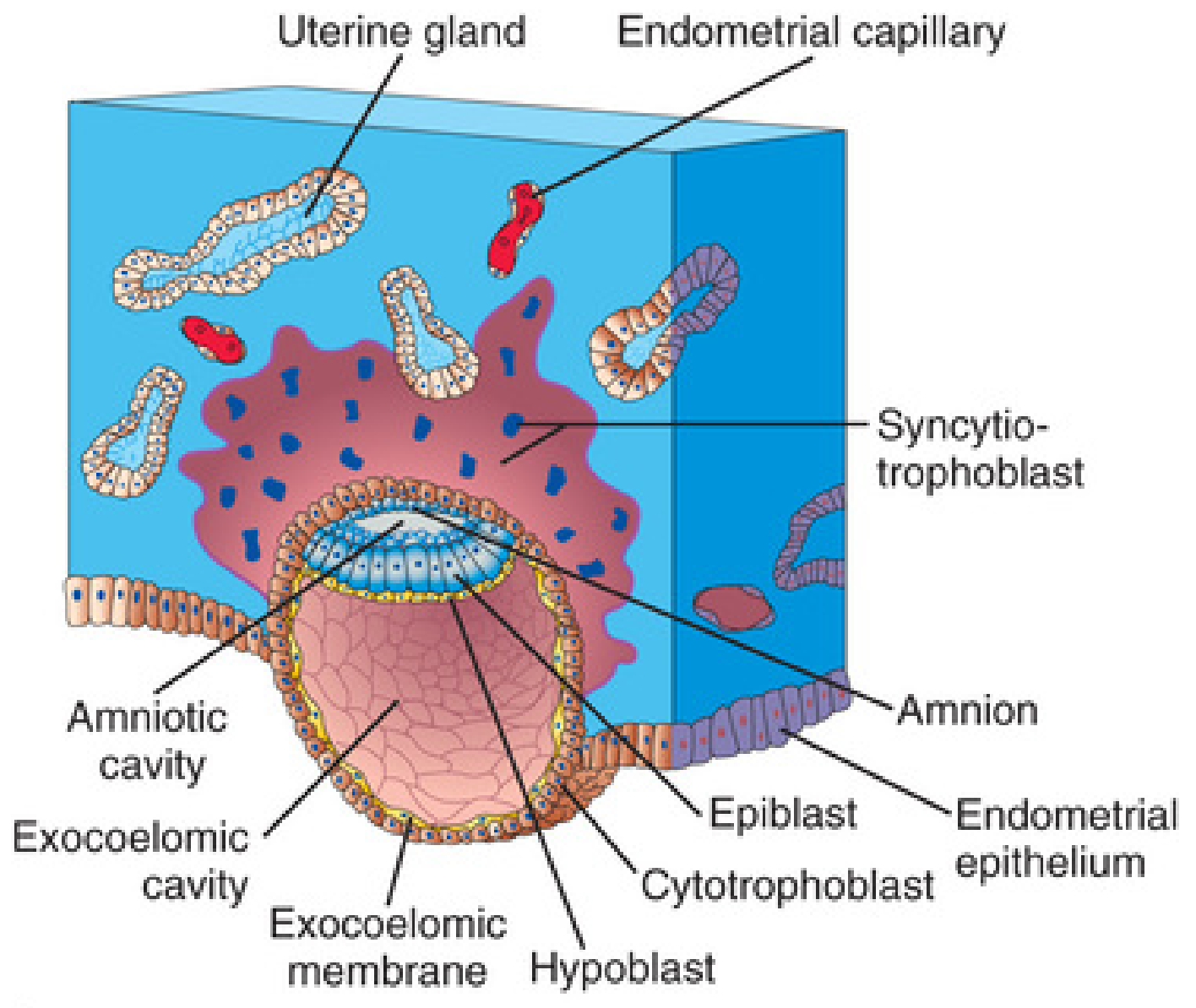
Completion of Implantation
- Implantation occurs 6-10 days after ovulation/fertilization.
- The trophoblast differentiates into:
- Cytotrophoblast (CTB): inner, mitotically active layer; mononuclear cells that migrate into syncytiotrophoblast
- Syncytiotrophoblast (STB): outer, rapidly expanding multinucleated mass with no cell boundaries; invasive, erodes endometrial stroma
- The syncytiotrophoblast invades the endometrial connective tissue, eroding maternal blood vessels - lacunae (small spaces) form within the STB and fill with maternal blood/secretions, establishing early uteroplacental circulation.
- Implantation is complete by day 10-12; the blastocyst is fully embedded in endometrium and the endometrial epithelium closes over it.
Bilaminar Embryonic Disc (Days 8-9)
Changes in the embryoblast produce a bilaminar embryonic disc composed of:
- Epiblast: thick layer of columnar cells adjacent to the amniotic cavity
- Hypoblast: thin layer of cuboidal cells adjacent to the exocoelomic cavity
Amniotic Cavity Formation (Day 8)
- A small space appears between the embryoblast and overlying cytotrophoblast - this is the amniotic cavity.
- Amnioblasts (derived from epiblast) line the cavity to form the amnion.
Exocoelomic (Primary Umbilical Vesicle / Yolk Sac) Formation (Day 8-9)
- Hypoblast cells migrate and line the blastocystic cavity to form the exocoelomic membrane (Heuser's membrane).
- Together with hypoblast, this forms the primary umbilical vesicle (exocoelomic cavity).
- A secondary umbilical vesicle (definitive yolk sac) forms later as the primary one largely disappears.
Extraembryonic Mesoderm and Coelom (Days 10-13)
- Extraembryonic mesoderm forms (from epiblast cells or hypoblast): fills space between trophoblast and amniotic/exocoelomic cavities.
- Spaces in it coalesce to form the extraembryonic coelom (chorionic cavity) - a large cavity surrounding the embryo except at the connecting stalk.
- The connecting stalk (future umbilical cord) attaches the embryo to the trophoblast.
Chorionic Sac
- The outer wall of the blastocyst (trophoblast + extraembryonic mesoderm) forms the chorion - the outermost fetal membrane.
- The embryo, amnion, and umbilical vesicle hang within the chorionic sac by the connecting stalk.
hCG Production
- The syncytiotrophoblast produces human chorionic gonadotropin (hCG) from day 8 onward.
- hCG maintains the corpus luteum (preventing luteal regression), which continues producing progesterone to maintain the endometrium.
- hCG is the basis of pregnancy tests - detectable in blood by day 8-10, in urine by day 14.
Summary Table - Week 2 ("Week of 2s")
| Structure | What forms |
|---|---|
| 2 trophoblast layers | Cytotrophoblast + Syncytiotrophoblast |
| 2 germ layers | Epiblast + Hypoblast (bilaminar disc) |
| 2 cavities | Amniotic cavity + Exocoelomic (yolk sac) cavity |
| 2 products | hCG secretion begins; Lacunae form |
WEEK 3 - Gastrulation, Notochord, Neurulation, and Early Organogenesis
The third week corresponds to 5 weeks after the last menstrual period (LMP) - the week after the first missed period. This is the most significant week of early development.
Key Events of Week 3:
- Gastrulation (primitive streak formation) - trilaminar disc
- Notochordal process and notochord
- Allantois formation
- Neurulation (neural plate and tube)
- Neural crest formation
- Somite development
- Intraembryonic coelom development
- Early cardiovascular system
1. Gastrulation and Primitive Streak (Day 15-16)
Gastrulation is the process by which the bilaminar disc is converted into a trilaminar embryonic disc with three germ layers: ectoderm, mesoderm, and endoderm.
- The primitive streak appears as a thickening of epiblast cells at the caudal end of the embryonic disc.
- It establishes the body axes: cranial-caudal, left-right, and dorsal-ventral.
- Epiblast cells migrate toward and through the primitive streak (invaginate/ingress):
- First wave: displaces hypoblast cells to form endoderm
- Second wave: migrates between epiblast and newly formed endoderm to form intraembryonic mesoderm
- Remaining epiblast cells become ectoderm
- The three primary germ layers are thus established:
| Germ Layer | Derivatives |
|---|---|
| Ectoderm | Skin, nervous system, sense organs, tooth enamel, lens, adrenal medulla |
| Mesoderm | Muscles, bones, connective tissue, cardiovascular system, kidneys, gonads, adrenal cortex |
| Endoderm | Epithelial lining of GI tract, respiratory tract, bladder, thyroid, parathyroid, liver, pancreas |
- The primitive node (Hensen's node) is the cranial end of the primitive streak - a circular elevation that controls body axis specification via signaling molecules (Nodal, FGF, BMP antagonists).
- Fate of the primitive streak: normally regresses and disappears by week 4. Persistence can cause a sacrococcygeal teratoma.
2. Notochordal Process and Notochord (Days 17-20)
- Cells from the primitive node migrate cranially to form the notochordal process (a hollow tube of cells).
- This develops into the notochord - a rod-like structure running the cranial-caudal axis under the neural plate.
- Functions of the notochord:
- Defines the primitive axis of the embryo
- Induces the overlying ectoderm to form the neural plate (primary inducer of neurulation)
- Becomes the nucleus pulposus of intervertebral discs in the adult
- Produces Sonic Hedgehog (Shh) protein - key developmental signaling molecule
3. Allantois (Day 16)
- A small diverticulum from the caudal wall of the umbilical vesicle extends into the connecting stalk.
- Remains small in humans; blood formation occurs here in early development.
- Associated with urachus development; persistent allantois can lead to a urachal cyst or sinus.
4. Neurulation: Neural Plate and Neural Tube (Days 18-28)
- The notochord induces the overlying ectoderm to thicken into the neural plate (day 18).
- The neural plate folds: edges elevate as neural folds, the groove between them is the neural groove.
- Neural folds fuse dorsally (starting at the cervical level) to form the neural tube.
- Closure of neural tube is complete by day 28 (end of week 4).
- Failure to close: Neural tube defects (NTDs)
- Cranial end fails to close → Anencephaly
- Caudal end fails to close → Spina bifida
- Folic acid supplementation (400-800 mcg/day) significantly reduces NTD risk.
5. Neural Crest Formation
- As neural folds fuse, neural crest cells separate from the edges of the neural plate.
- These are highly migratory, pluripotent cells.
- Give rise to: peripheral and autonomic nervous system, melanocytes, facial bones/cartilage, adrenal medulla, Schwann cells, odontoblasts.
6. Somite Development (Days 20-30)
- Paraxial mesoderm on either side of the notochord and neural tube segments into paired somites (block-like structures).
- The first pair forms around day 20; new pairs form cranio-caudally at ~3 pairs/day.
- By end of week 3: approximately 4 pairs of somites
- By end of week 5: ~42-44 pairs total
- Somites differentiate into:
- Sclerotome → vertebrae, ribs, part of skull base
- Myotome → skeletal muscles of trunk and limbs
- Dermatome → dermis of back
7. Intraembryonic Coelom (Week 3)
- Spaces appear in the lateral plate mesoderm and coalesce to form the intraembryonic coelom (body cavity).
- Lateral plate mesoderm splits into:
- Somatic (parietal) layer - associated with overlying ectoderm → forms body wall
- Splanchnic (visceral) layer - associated with underlying endoderm → forms gut wall
- The intraembryonic coelom will later be partitioned into pericardial, pleural, and peritoneal cavities.
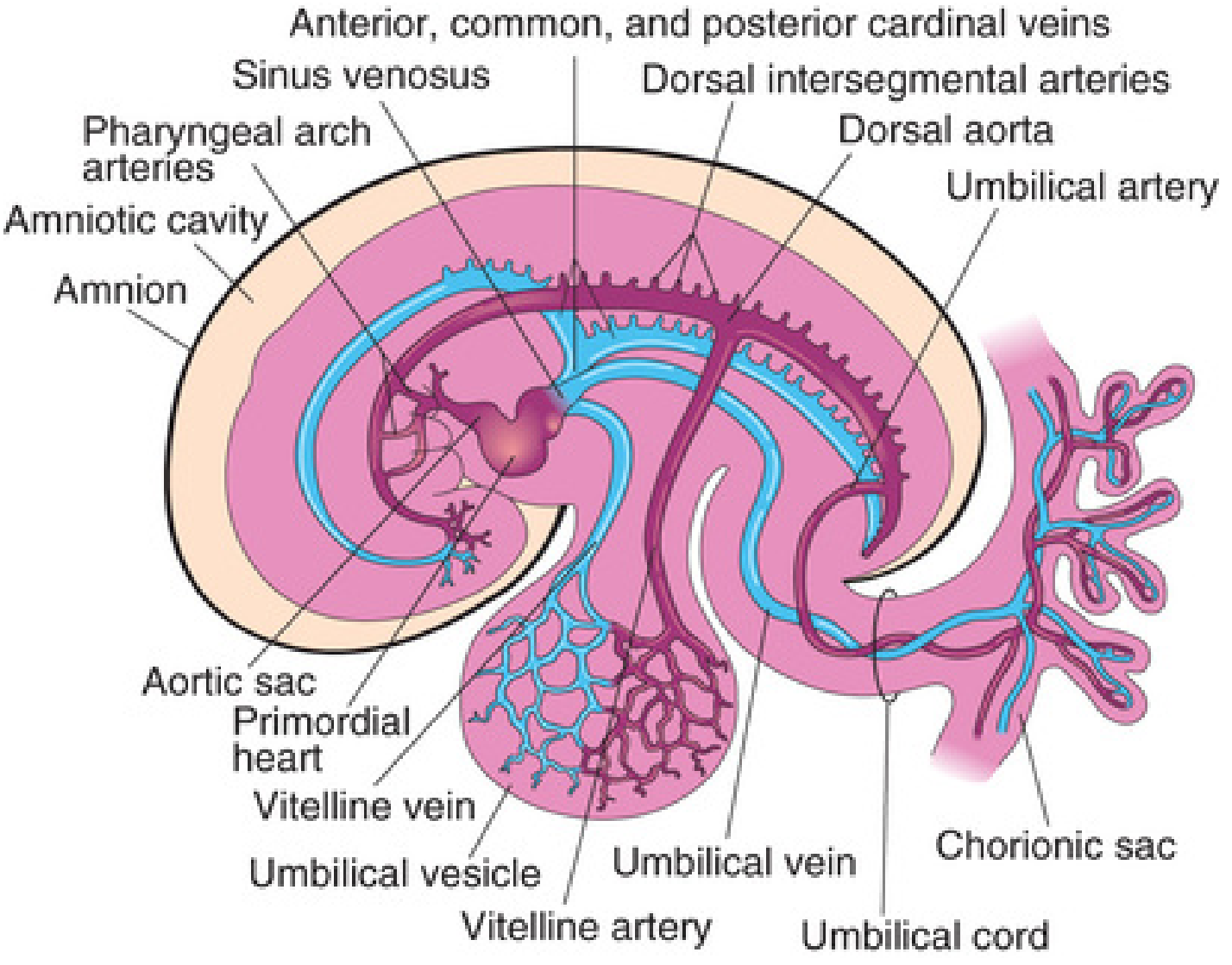
8. Early Cardiovascular System (Days 16-21)
- Vasculogenesis begins: angioblasts in the extraembryonic mesoderm and in the embryonic mesoderm aggregate to form blood islands.
- The paired heart tubes form from cardiogenic mesoderm cranial to the neural plate.
- By day 21: the heart begins to beat - the earliest functioning system in the embryo.
- Primordial cardiovascular system is established including the heart, dorsal aortae, and umbilical vessels.
9. Chorionic Villi Development
- Primary chorionic villi form during week 2 (cytotrophoblast cores covered by syncytiotrophoblast).
- During week 3, extraembryonic mesoderm grows into the primary villi cores → secondary chorionic villi.
- Blood vessels develop within them → tertiary chorionic villi (by end of week 3).
- Tertiary villi are the functional villous units of the placenta.
Summary Table: Key Events by Week
| Feature | Week 1 | Week 2 | Week 3 |
|---|---|---|---|
| Main event | Fertilization, cleavage, blastocyst formation | Implantation complete, bilaminar disc | Gastrulation, trilaminar disc |
| Embryonic disc | - | Bilaminar (epiblast + hypoblast) | Trilaminar (ecto-, meso-, endoderm) |
| Trophoblast | CTB differentiates | CTB + STB; lacunae form | Chorionic villi (tertiary) |
| Key structures formed | Zygote → morula → blastocyst | Amnion, yolk sac, chorionic sac, connecting stalk | Primitive streak, notochord, neural plate, somites, heart |
| Hormonal signal | - | hCG produced (from day 8) | hCG peaks; progesterone maintained |
| Clinical landmark | Pregnancy begins | Pregnancy test positive | First missed period; morning sickness may begin |
Clinically Important Points
- Ectopic pregnancy: implantation outside the uterus (most commonly in the uterine tube ampulla) can occur if the blastocyst fails to reach the uterus.
- Twinning: Monozygotic (identical) twins arise from splitting of one embryo. Timing of splitting determines chorionicity - splitting before day 3 → dichorionic; days 4-8 → monochorionic diamniotic; days 8-12 → monochorionic monoamniotic; after day 13 → conjoined twins.
- hCG and pregnancy tests: Serum beta-hCG detectable from day 8-10; urinary tests from ~day 14.
- Neural tube defects: Folic acid 400 mcg daily periconceptionally reduces risk by ~70%.
- Sacrococcygeal teratoma: results from persistence of the primitive streak - most common tumor in neonates.
- Nucleus pulposus: the remnant of the notochord in adult intervertebral discs - relevant in disc herniation.
- Teratogens are most dangerous during week 3 onward, when organogenesis begins (organ-specific sensitive periods). Weeks 1-2 follow the "all or nothing" rule - severe damage kills the embryo; minor damage allows full recovery.
- The Developing Human: Clinically Oriented Embryology (Moore & Persaud)
Cardiovascular system embryology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive, detailed content from the textbook. Let me compile the full answer.
Cardiovascular System Embryology
Source: The Developing Human: Clinically Oriented Embryology (Moore & Persaud)
Overview
The cardiovascular system is the first major organ system to function in the embryo. It appears in the middle of the third week and the heart begins beating at day 22-23. This early development is driven by the urgent need for oxygen and nutrients - the rapidly growing embryo can no longer rely on diffusion alone from the beginning of week 3.
Critical period of heart development: Day 20 to Day 50 after fertilization.
1. Vasculogenesis and Angiogenesis (Week 3)
At the end of week 2, embryonic nutrition comes from diffusion across the extraembryonic coelom. By the start of week 3, this is no longer sufficient.
- Vasculogenesis: Formation of new blood vessels from de novo aggregation of angioblasts (mesenchymal precursor cells) into blood islands in the extraembryonic mesoderm of the umbilical vesicle, connecting stalk, and chorion.
- These blood islands canalize to form endothelial tubes - the first blood vessels.
- Angiogenesis: Sprouting and growth of new vessels from pre-existing ones - this is how the embryonic vascular network expands.
- By approximately day 20, embryonic blood vessel formation begins within the embryo itself (about 2 days after extraembryonic vessel formation).
2. Formation of the Primordial Heart Tube (Days 18-22)
- By day 18, bilateral mesoderm (splanchnopleure component) gives rise to paired endocardial progenitor cells that form two separate endocardial heart tubes on either side of the embryo.
- As lateral embryonic folding occurs (bringing the lateral body walls toward the midline), the two heart tubes are carried ventrally and toward each other.
- They fuse craniocaudally to form a single tubular heart - the primitive heart tube.
- The heart tube is composed of three layers (from inside out):
- Endocardium (inner endothelial lining)
- Cardiac jelly (gelatinous extracellular matrix between layers)
- Myocardium (from splanchnic mesoderm of the pericardial cavity)
- The epicardium develops later from the proepicardium (a cluster of cells near the sinus venosus).
- The heart tube is initially suspended in the pericardial cavity by the dorsal mesocardium, which degenerates to form the transverse pericardial sinus.
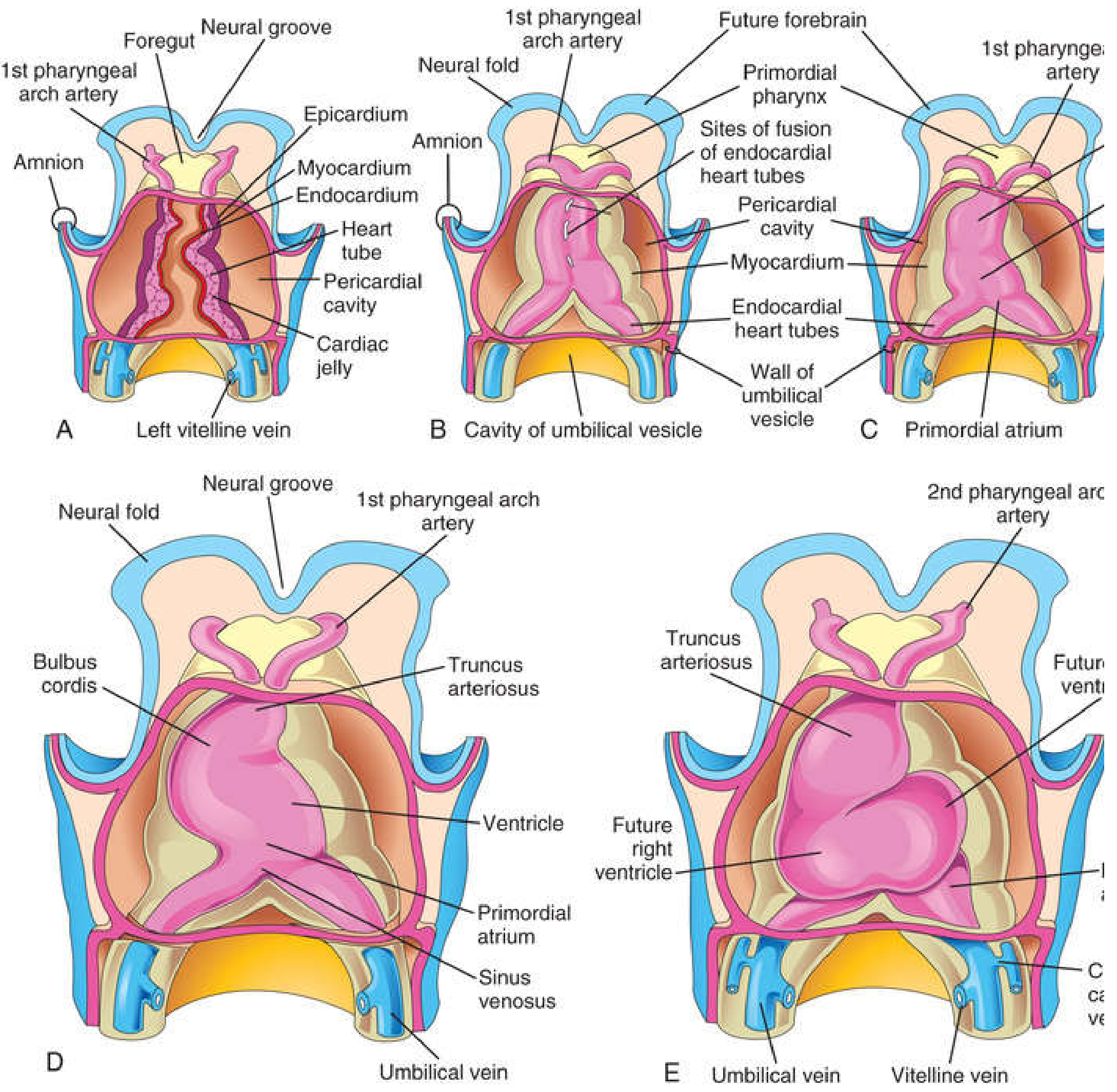
Regions of the Primitive Heart Tube (Craniocaudal)
| Region | Fate |
|---|---|
| Truncus arteriosus | Ascending aorta + pulmonary trunk |
| Bulbus cordis | Smooth part of right ventricle (conus arteriosus) + right ventricular outflow |
| Primordial ventricle | Left ventricle (trabeculated part) |
| Primordial atrium | Left and right atria (trabeculated parts) |
| Sinus venosus | SA node, coronary sinus, smooth wall of right atrium |
3. Cardiac Looping (Days 23-28)
- The heart tube elongates rapidly but is constrained within the pericardial cavity.
- It bends (loops) to the right - forming a D-loop (dextro loop), creating an S-shaped heart.
- This rightward looping is the first morphological evidence of left-right asymmetry in the embryo.
- Leftward looping (L-loop) results in situs inversus or dextrocardia.
- By day 28, the external heart resembles the adult configuration.
- Heart beat begins at day 22-23 - initially myogenic peristalsis-like contractions, progressing to unidirectional flow by end of week 4.
4. Partitioning of the Heart (Weeks 4-8)
Partitioning begins in the middle of week 4 and is complete by the end of week 8. All processes occur simultaneously.
A. Partitioning of the Atrioventricular (AV) Canal
- AV endocardial cushions (superior and inferior) form on the dorsal and ventral walls of the AV canal (end of week 4).
- These are composed of cardiac jelly + neural crest-derived mesenchymal cells.
- The cushions grow toward each other and fuse, dividing the AV canal into right and left AV canals.
- The cushions also form the AV valves (mitral and tricuspid).
- The mitral (bicuspid) valve has 2 leaflets; the tricuspid valve has 3.
B. Partitioning of the Primordial Atrium (Atrial Septal Formation)
Two septa form sequentially:
Septum Primum:
- Grows caudally from the roof of the atrium toward the AV endocardial cushions.
- The gap between its free edge and the cushions = ostium primum (foramen primum) - allows right-to-left blood flow initially.
- Before ostium primum closes, perforations appear in the upper part of septum primum (due to programmed cell death), forming the ostium secundum (foramen secundum) - maintains right-to-left shunt.
- Septum primum ultimately becomes the valve of the foramen ovale.
Septum Secundum:
- A thick, muscular septum grows caudally on the right side of septum primum.
- It is incomplete - its free lower edge forms a curved oval opening: the foramen ovale.
- The foramen ovale is covered on the left side by the valve-like septum primum.
- In fetal life, blood flows from right atrium → foramen ovale → left atrium (right-to-left shunt, normal in the fetus).
- At birth, rising left atrial pressure pushes the septum primum against septum secundum, functionally closing the foramen ovale.
- Anatomic closure within a few months forms the fossa ovalis and its annulus.
- Patent Foramen Ovale (PFO): failure of anatomic closure (probe-patent in ~25% of adults).
C. Partitioning of the Ventricles (Interventricular Septum)
- The muscular interventricular (IV) septum grows superiorly from the floor of the ventricle.
- The IV foramen (gap between muscular septum and AV cushions) normally closes by the end of week 7.
- Closure occurs via:
- Growth of the muscular IV septum
- Downgrowth of the aorticopulmonary septum (conotruncal ridges)
- Tissue from the AV endocardial cushions
- Together, these form the membranous part of the IV septum.
- Ventricular Septal Defect (VSD): most common congenital heart defect (25-30% of all CHDs); most commonly involves the membranous part.
D. Partitioning of the Outflow Tract (Truncus Arteriosus and Bulbus Cordis)
- Neural crest cells migrate into the outflow tract and form conotruncal ridges within the truncus arteriosus and conus cordis (bulbus cordis).
- These ridges spiral around each other (in an approximately 180° spiral), then fuse to form the aorticopulmonary septum.
- This divides the truncus arteriosus into the:
- Ascending aorta - connected to the left ventricle
- Pulmonary trunk - connected to the right ventricle
- The spiral arrangement of the septum gives the great vessels their characteristic helical relationship.
- Disruption of neural crest cell migration → conotruncal defects:
- Transposition of the Great Arteries (TGA): aorticopulmonary septum fails to spiral
- Tetralogy of Fallot (ToF): unequal division of truncus arteriosus (pulmonary stenosis, large VSD, overriding aorta, RV hypertrophy)
- Persistent Truncus Arteriosus: failure of septum formation
5. Sinus Venosus and Changes (Week 5-8)
The sinus venosus initially has right and left horns, draining the common cardinal, umbilical, and vitelline veins.
- The right sinus venosus horn enlarges to become the smooth-walled part of the right atrium (sinus venarum).
- The left horn shrinks and becomes the coronary sinus.
- The right horn is incorporated into the right atrium, bringing the SA node (located in the right wall of the sinus venosus) to the right atrium near the SVC entry.
6. Conducting System of the Heart
| Structure | Origin | Adult Location |
|---|---|---|
| SA node | Right wall of sinus venosus | Right atrium, near SVC - the pacemaker |
| AV node | Left wall of sinus venosus + AV region cells | Base of interatrial septum |
| Bundle of His (AV bundle) | AV region | Interventricular septum |
| Bundle branches | AV bundle | Right and left ventricles |
| Purkinje fibers | Bundle branches | Ventricular myocardium |
- Conducting system is well developed before nerve supply reaches the heart.
- Parasympathetic innervation of the heart (vagal) is derived from neural crest cells.
- The chambers are electrically isolated by a fibrous skeleton (connective tissue from epicardium) - only the AV node and bundle bridge atria and ventricles.
7. Development of the Veins
Three pairs of veins drain the primordial heart:
| Vein System | Fate |
|---|---|
| Vitelline veins (from umbilical vesicle) | Become hepatic portal system, hepatic veins, most of IVC |
| Umbilical veins | Right involutes; left → ductus venosus → ligamentum venosum after birth |
| Cardinal veins (anterior + posterior → common cardinal) | Form the caval system (SVC, IVC, azygos vein) |
8. Pharyngeal Arch Arteries (Aortic Arches)
During weeks 4-5, six pairs of pharyngeal arch arteries arise from the aortic sac and enter the pharyngeal arches. By weeks 6-8, they are remodeled:
| Arch | Fate |
|---|---|
| 1st arch artery | Largely disappears; contributes to maxillary artery |
| 2nd arch artery | Largely disappears; hyoid and stapedial arteries |
| 3rd arch artery | Common carotid arteries; proximal internal carotid arteries |
| 4th arch artery | Left: aortic arch (between left common carotid and left subclavian); Right: proximal right subclavian artery |
| 5th arch artery | Rudimentary; disappears |
| 6th arch artery | Left: left pulmonary artery + ductus arteriosus (becomes ligamentum arteriosum); Right: right pulmonary artery (distal part disappears) |
Pharyngeal Arch Artery Defects
- Coarctation of the aorta: narrowing at the aortic isthmus (near ductus arteriosus). Postductal (most common) - develops collateral circulation. Preductal - ductus arteriosus keeps lower body perfused; closure at birth is critical. Associated with Turner syndrome.
- Double aortic arch: failure of right dorsal aorta to disappear → vascular ring compresses trachea and esophagus (stridor, dysphagia).
- Right arch of aorta: entire right dorsal aorta persists.
- Aberrant right subclavian artery: right subclavian crosses behind esophagus → dysphagia lusoria.
9. Fetal Circulation
The fetal lungs are nonfunctional, so the circulation bypasses them via three special structures:
Fetal Shunts
| Shunt | Route | Purpose |
|---|---|---|
| Ductus venosus | Umbilical vein → bypasses liver → IVC | Carries oxygenated blood from placenta directly to heart |
| Foramen ovale | Right atrium → left atrium | Bypasses pulmonary circulation |
| Ductus arteriosus | Pulmonary trunk → descending aorta | Bypasses lungs |
Flow of Oxygenated Blood in the Fetus
- Oxygenated blood from placenta travels via the umbilical vein (the only vessel carrying oxygenated blood in the fetus)
- ~50% bypasses the liver via the ductus venosus → enters IVC → right atrium
- Most IVC blood is directed by the crista dividens (inferior border of septum secundum) through the foramen ovale → left atrium → left ventricle → ascending aorta → coronary arteries and head/neck (best-oxygenated blood goes to brain and heart)
- SVC blood (deoxygenated from head) → right atrium → right ventricle → pulmonary trunk
- Because pulmonary resistance is high, most blood flows via ductus arteriosus → descending aorta → body → umbilical arteries → placenta for reoxygenation
- The pulmonary arteries receive only ~10% of cardiac output in fetal life
10. Circulatory Changes at Birth
At birth, three critical changes occur simultaneously:
| Event | Mechanism | Result |
|---|---|---|
| Lungs expand | First breath, decreased pulmonary resistance | Increased pulmonary blood flow |
| Umbilical cord clamped | Umbilical arteries constrict, vein collapses | Loss of placental circulation, increased systemic resistance |
| Foramen ovale closes | Left atrial pressure > right atrial pressure | Functional closure (flap valve mechanism) |
| Ductus arteriosus closes | Rising pO2 → smooth muscle contraction; bradykinin released by lungs; reduced prostaglandin E2 | Closes functionally within 24-96 hours; anatomical closure by week 1-3 |
| Ductus venosus closes | Loss of umbilical vein flow | Becomes ligamentum venosum |
Timeline of Ductus Arteriosus Closure
- 24 hours: 20% closed
- 48 hours: ~80% closed
- 96 hours: 100% closed (term neonates)
- In premature infants: closure may be delayed due to hypoxia and elevated prostaglandins
- Indomethacin (prostaglandin synthesis inhibitor) can close a patent DA in premature neonates
- PGE2 (prostaglandin) is used to keep the DA open in duct-dependent congenital heart lesions (e.g., TGA, pulmonary atresia) until surgery
Adult Derivatives of Fetal Structures
| Fetal Structure | Adult Derivative |
|---|---|
| Ductus arteriosus | Ligamentum arteriosum |
| Foramen ovale | Fossa ovalis |
| Ductus venosus | Ligamentum venosum |
| Umbilical vein | Ligamentum teres hepatis (round ligament of liver) |
| Umbilical arteries | Medial umbilical ligaments (distal parts); proximal parts → superior vesical arteries |
11. Congenital Heart Defects (CHDs)
Frequency: 6-8 per 1000 live births. Most are multifactorial.
| Defect | Mechanism | Key Features |
|---|---|---|
| VSD | Failure of membranous IV septum closure | Most common CHD (~25-30%); L→R shunt |
| ASD (Ostium secundum) | Excessive resorption of septum primum or inadequate septum secundum | L→R shunt; "fixed split S2" |
| Patent Foramen Ovale (PFO) | Failure of anatomic septum fusion | ~25% of adults; usually asymptomatic |
| Tetralogy of Fallot | Unequal division of truncus/conus | PS + VSD + overriding aorta + RVH; most common cyanotic CHD |
| TGA | Failure of aorticopulmonary septum to spiral | Aorta from RV, PA from LV; incompatible with life unless shunt present |
| PDA | Failure of ductus arteriosus to close | L→R shunt; "machinery murmur"; treated with indomethacin or surgical ligation |
| Coarctation of aorta | Abnormal aortic narrowing near DA | Rib notching; upper limb HTN; associated with Turner syndrome |
| Persistent truncus arteriosus | Failure of aorticopulmonary septum formation | Always has a large VSD; single vessel from both ventricles |
| Hypoplastic left heart syndrome | Underdevelopment of left heart structures | Duct-dependent systemic circulation |
| Dextrocardia | Abnormal cardiac looping (L-loop) | Mirror-image heart; if isolated, usually asymptomatic |
| Ebstein anomaly | Displacement of tricuspid valve into RV | Associated with maternal lithium use |
Summary Timeline
| Time | Event |
|---|---|
| Day 18-20 | Blood islands form; vasculogenesis begins |
| Day 20-22 | Paired heart tubes fuse into single tube |
| Day 22-23 | Heart begins to beat (first functioning organ) |
| Day 23-28 | Cardiac looping (D-loop) |
| Day 28 | Neural tube closes; heart resembles adult external shape |
| Week 4-5 | Endocardial cushion formation; atrial/ventricular septation begins |
| Week 5-6 | Aorticopulmonary septum forms (spiraling); pharyngeal arch arteries remodel |
| Week 5-6 | Conducting system develops |
| Week 8 | Partitioning complete; four-chambered heart |
| Birth | Foramen ovale closes; ductus arteriosus constricts |
| Week 1-3 postnatal | Anatomic closure of foramen ovale and ductus arteriosus |
- The Developing Human: Clinically Oriented Embryology (Moore & Persaud)
This is a shared conversation. Sign in to Orris to start your own chat.