20 heart diseases and their specific ECG findings with ECGs
Reading File
Finding Sources
Finding Sources
Searching the Web
20 heart diseases ECG findings electrocardiogram patterns
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
I now have excellent textbook content and ECG images from authoritative sources. Let me compile a comprehensive response covering 20 heart diseases with their specific ECG findings and images.
20 Heart Diseases and Their Specific ECG Findings
1. ST-Elevation Myocardial Infarction (STEMI) - Anterolateral
ECG Findings:
- ST elevation in V1-V4 (anterior leads) and I, aVL, V5, V6 (lateral leads)
- Reciprocal ST depression in leads III, aVF
- Development of Q waves in infarcted territory
- Hyperacute (peaked) T waves in early phase
- Proximal LAD occlusion with thrombus
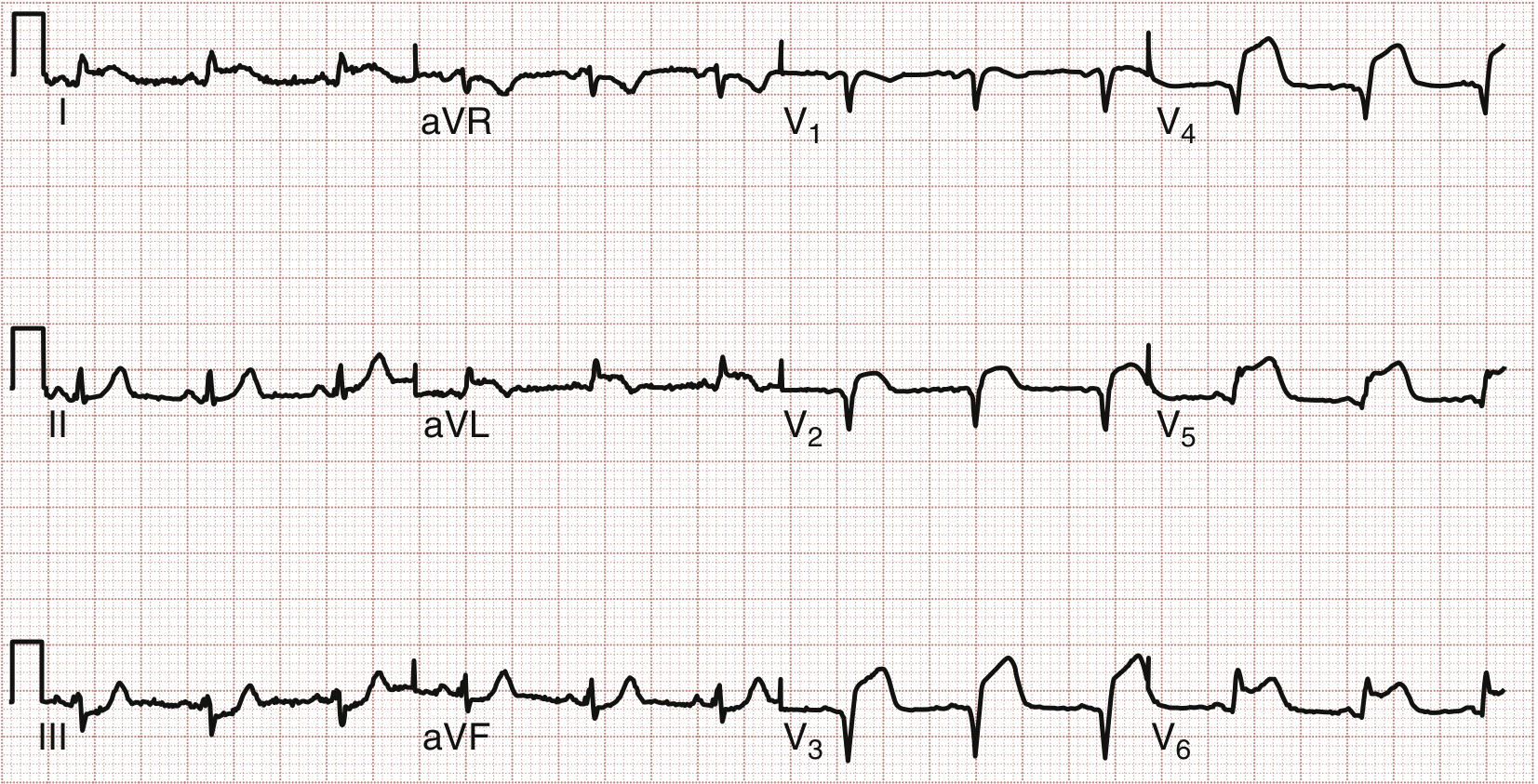
Anterolateral STEMI: ST elevation in V1-V4 (anterior) and I, aVL, V5, V6 (lateral). Proximal LAD lesion confirmed at emergent PCI. - Rosen's Emergency Medicine
2. Inferior STEMI
ECG Findings:
- ST elevation in II, III, aVF (inferior leads) - ≥2 contiguous inferior leads required
- Reciprocal ST depression in leads I and aVL
- ST elevation greater in III than II = 90% sensitive for RCA occlusion
- ST elevation in V1 with inferior STEMI suggests concomitant right ventricular infarction
- Left circumflex occlusion: III elevation NOT > II, aVL isoelectric or elevated
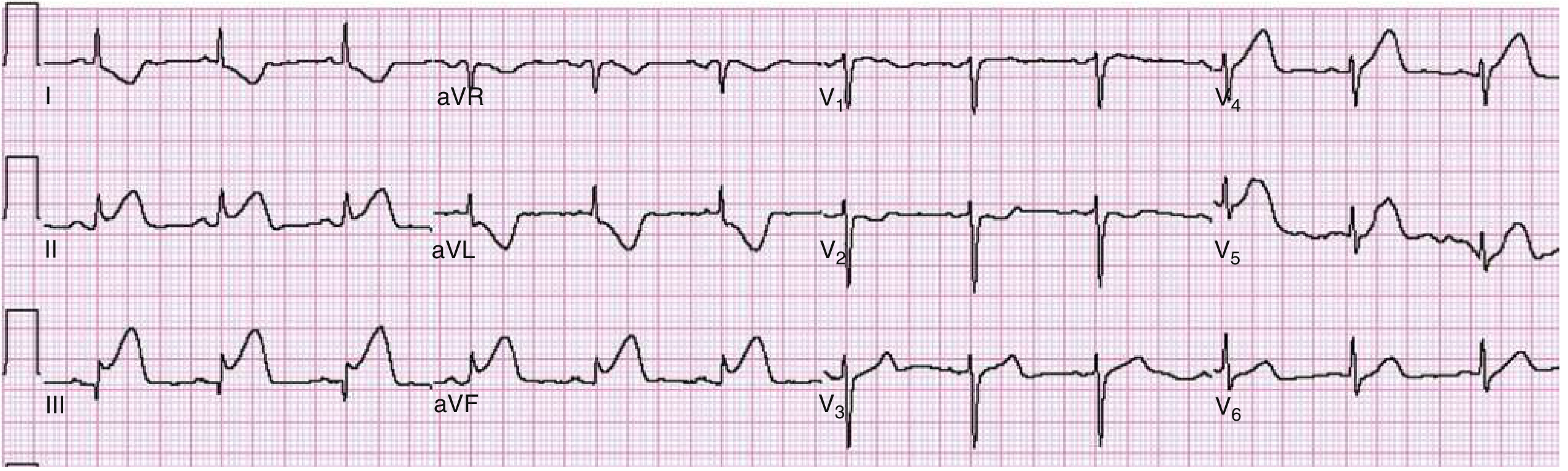
Inferior STEMI: Marked ST elevation inferiorly (II, III, aVF). Classic reciprocal ST depression in I and aVL. - Rosen's Emergency Medicine
3. Posterior Myocardial Infarction
ECG Findings:
- No direct ST elevation on standard 12-lead (no posterior electrodes)
- Reciprocal changes in V1-V3: horizontal ST depression + upright T wave
- Tall, wide R wave in V1-V2 (mirror image of posterior Q wave)
- R:S ratio >1 in V1-V2
- Posterior leads V8-V9: direct ST elevation (increases sensitivity)
- Occurs in ~15-20% of all AMIs, usually with inferior or inferolateral MI
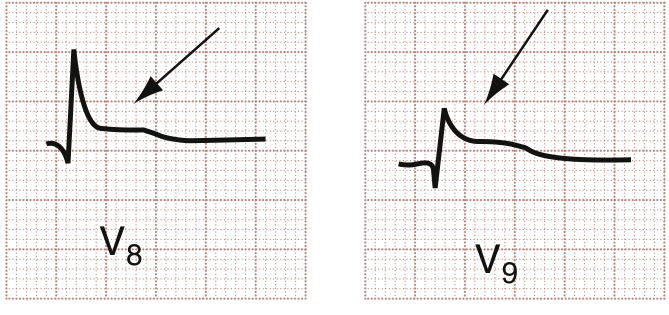
Posterior MI: V8 and V9 posterior leads showing subtle ST elevation (arrows), consistent with acute posterior wall MI. Horizontal ST depression and tall R waves in V1-V2 are the mirror-image findings. - Rosen's Emergency Medicine
4. de Winter Pattern (Proximal LAD Occlusion)
ECG Findings:
- J-point depression with upsloping ST depression in anterior leads (V1-V6)
- Prominent, hyperacute (tall, peaked) T waves in anterior leads
- ST elevation in aVR
- No classic ST elevation - this pattern is a "STEMI equivalent"
- Indicates proximal LAD obstruction
"The de Winter electrocardiographic finding, a pattern associated with proximal left anterior descending coronary artery obstruction. In the anterior leads, ST segment depression with depression of the J point is noted along with prominent, hyperacute T wave. In addition, ST segment elevation is also seen in lead aVR." - Rosen's Emergency Medicine
5. High Lateral STEMI
ECG Findings:
- ST elevation in leads I and aVL
- Reciprocal ST depression in III, aVF, and V1
- ST elevation in V2 may also be seen
- Indicates obstruction of left circumflex or first diagonal (D1) artery
6. Wolff-Parkinson-White (WPW) Syndrome
ECG Findings (classic triad during sinus rhythm):
- Short PR interval (<120 ms) - due to pre-excitation via accessory pathway
- Delta wave - slurred upstroke at the beginning of the QRS complex
- Widened QRS complex (>120 ms) - from ventricular pre-excitation
- Secondary ST/T wave changes (discordant to QRS)
- During tachycardia: narrow complex (orthodromic AVRT) or wide complex (antidromic AVRT)
- Associated with ventricular fibrillation if atrial fibrillation occurs through the accessory pathway
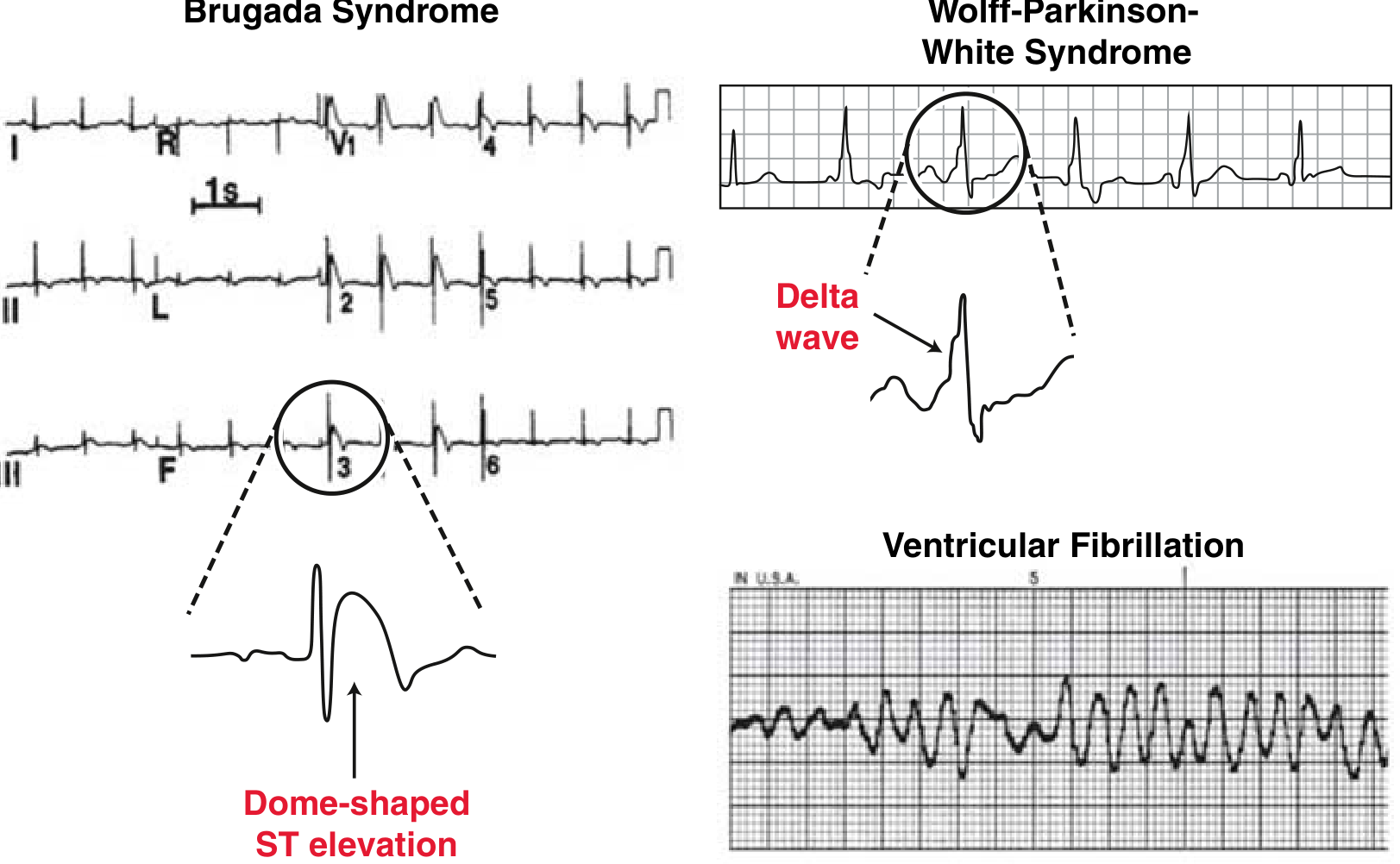
Top right: WPW - delta wave (slurred QRS upstroke) with short PR interval. Bottom left: Brugada - dome-shaped ST elevation in V1-V3. Bottom right: Ventricular fibrillation. - Miller's Review of Orthopaedics
7. Brugada Syndrome
ECG Findings (Type 1 - diagnostic):
- Coved-type (dome-shaped) ST elevation ≥2 mm in V1-V2 (sometimes V3), followed by a negative T wave
- Right bundle branch block (RBBB) pattern
- Type 2: "Saddle-back" ST elevation (≥2 mm J-wave, ≥1 mm ST elevation above baseline)
- Pattern may be dynamic - can appear normal between episodes
- Associated with syncope and sudden cardiac death from VF/VT
- Triggered/unmasked by fever, sodium channel blockers, vagotonic states
8. Long QT Syndrome (LQTS)
ECG Findings:
- Prolonged QT interval - corrected QTc >450 ms in males, >460 ms in females
- T wave morphology abnormalities: broad, notched, or biphasic T waves
- Predisposes to Torsades de Pointes (polymorphic VT)
- Associated with sudden cardiac death
- Each LQTS genetic subtype has characteristic T-wave morphology
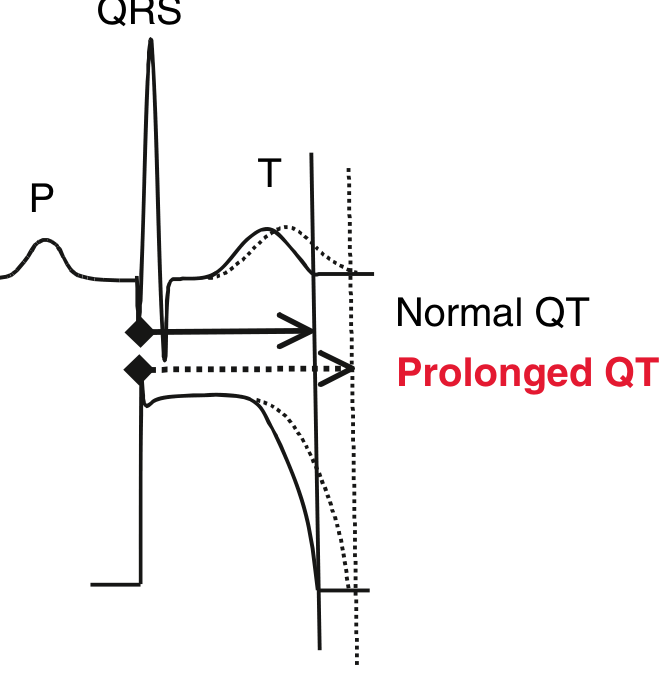
Long QT Syndrome: The dotted line shows prolonged QT interval extending beyond the normal QT endpoint. Prolonged QTc >450 ms is a risk factor for torsades de pointes and sudden cardiac death. - Miller's Review of Orthopaedics
9. Ventricular Fibrillation (VF)
ECG Findings:
- Completely chaotic, irregular electrical activity
- No discernible P waves, QRS complexes, or T waves
- Irregular, rapid undulations of varying amplitude and frequency
- Rate: 300-600 "depolarizations" per minute
- Immediately life-threatening - no organized cardiac output
- Often preceded by VT or preceded by R-on-T phenomenon
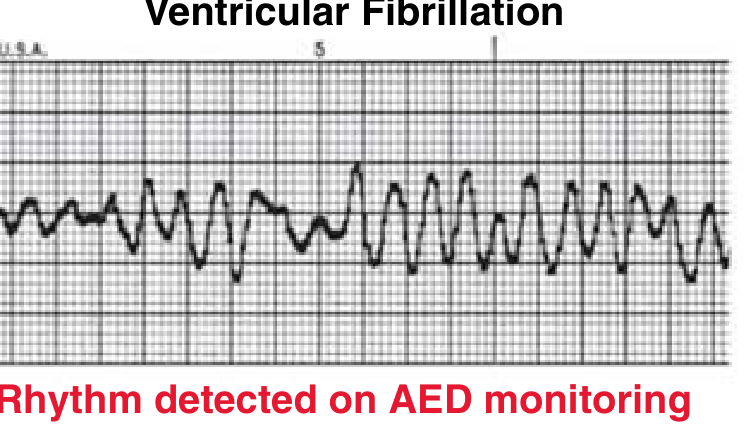
Ventricular fibrillation: Completely disorganized electrical activity with no identifiable waveforms. - Miller's Review of Orthopaedics
10. Hypertrophic Cardiomyopathy (HCM)
ECG Findings:
- Left ventricular hypertrophy (LVH) - deep S waves in V1-V3 (often >25-30 mm)
- Narrow septal Q waves in lateral leads (V5, V6, I, aVL) - from septal hypertrophy
- Upright T waves in leads with septal Q waves (V3, V6) - characteristic pattern
- Left atrial enlargement (broad, notched P waves)
- May show atrial fibrillation or atrial flutter
- Deep T-wave inversions in lateral leads if ischemic component
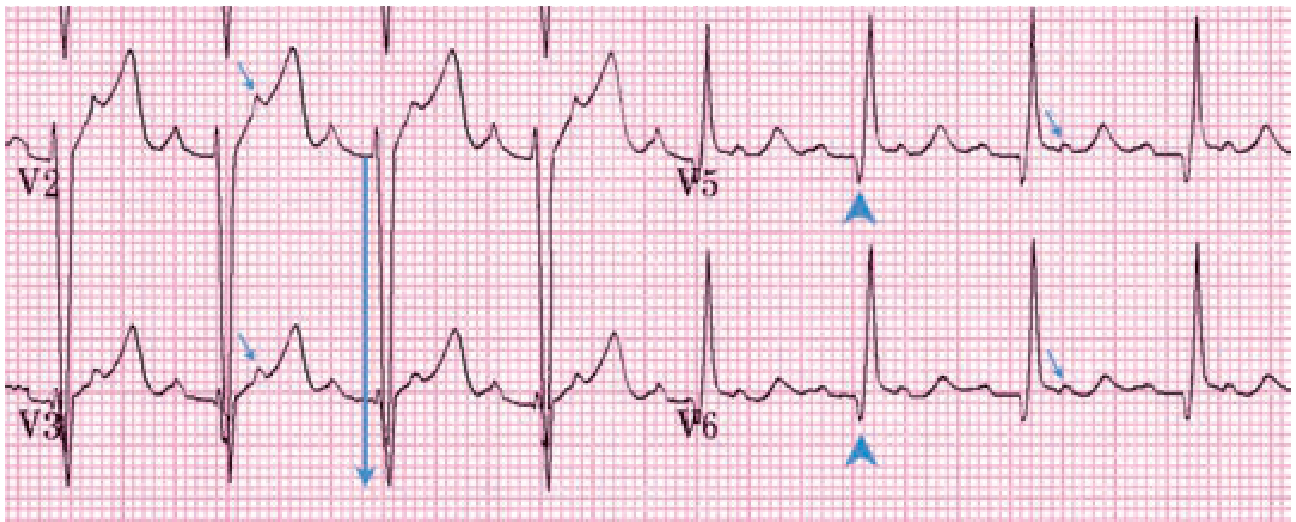
HCM: Deep S-wave (28 mm) in V3 (LVH, large arrow). Narrow septal Q waves in V5-V6 (arrowheads). Upright T waves in V3 and V6, typical of HCM. Atrial flutter with 2:1 block - extra P waves visible in ST segments (small arrows). - Tintinalli's Emergency Medicine
11. Acute Pericarditis
ECG Findings (4 phases):
- Phase 1 (days 1-2): Diffuse ST elevation (saddle-shaped, concave up) in most leads; PR depression in most leads (PR elevation in aVR); no Q waves; no reciprocal ST depression (key differentiator from STEMI)
- Phase 2 (days 3-7): ST returns to baseline; T-wave amplitude decreases and flattens
- Phase 3 (weeks 1-3): T-wave inversions; ST isoelectric
- Phase 4: Complete resolution
- Spitzberg sign: ST/T ratio >0.25 in V6
- Low voltage in all leads if large pericardial effusion present
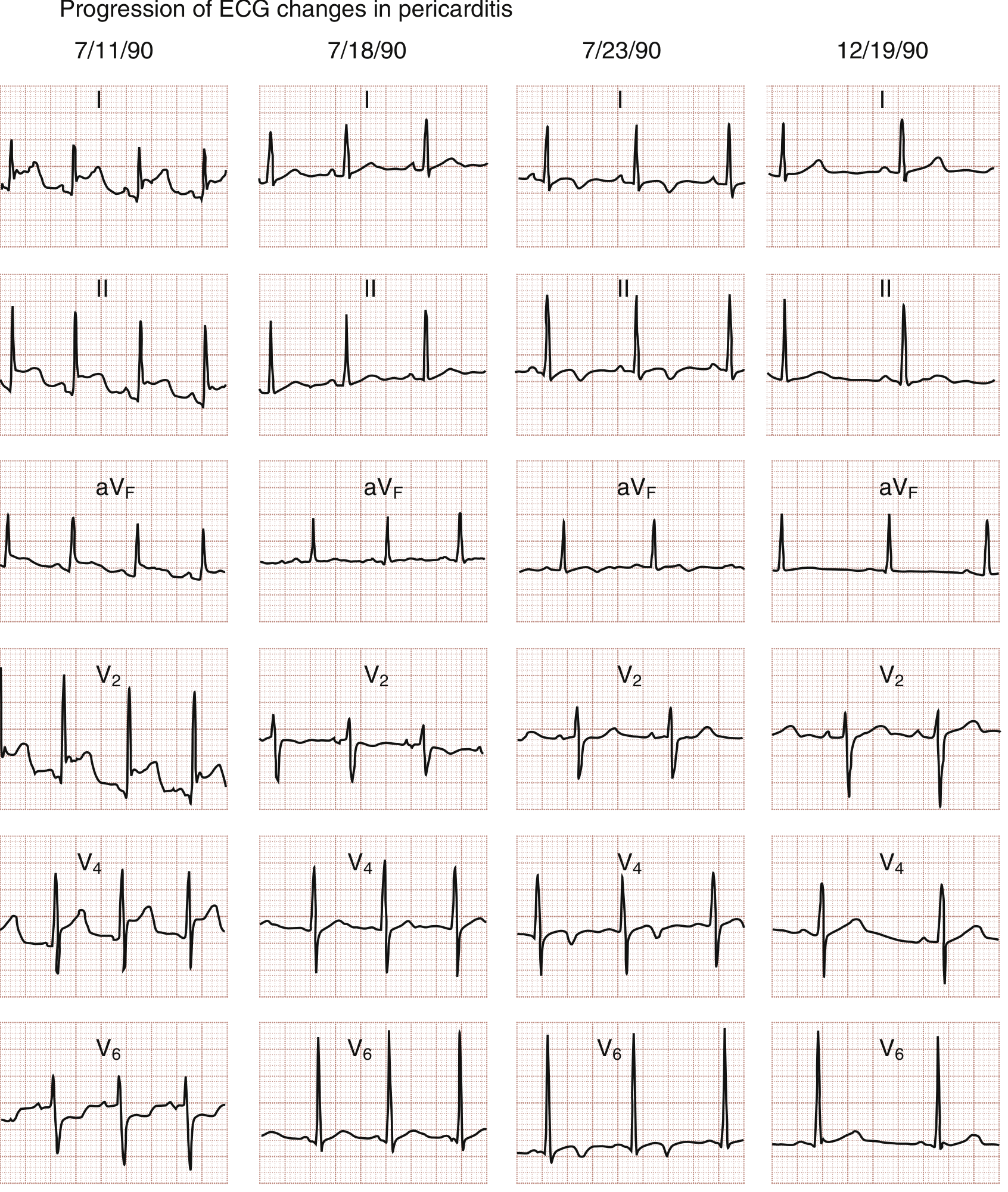
Classic pericarditis ECG progression: Phase 1 (7/11) - diffuse ST elevation. Phase 2 (7/18) - ST normalizes, T-wave flattening. Phase 3 (7/23) - T-wave inversions. Phase 4 (12/19) - complete resolution. - Rosen's Emergency Medicine
12. Atrial Fibrillation (AF)
ECG Findings:
- Absent P waves - replaced by fibrillatory (f) waves (irregular, chaotic baseline) at 350-600/min
- Irregularly irregular R-R intervals - hallmark finding
- Narrow QRS (unless pre-existing bundle branch block or aberrant conduction)
- Ventricular rate usually 100-180/min if untreated (AV node limits conduction)
- "Coarse AF" - prominent f waves; "Fine AF" - barely visible baseline oscillations
- WPW + AF = wide irregular tachycardia (dangerous - irregular pre-excited beats, can degenerate to VF)
13. Atrial Flutter
ECG Findings:
- Sawtooth flutter waves (F waves) at ~300/min in inferior leads (II, III, aVF)
- Regular atrial activity, usually with 2:1 AV block → ventricular rate ~150/min
- Flutter waves best seen in leads II, III, aVF (negative) and V1 (positive)
- Narrow QRS (unless aberrancy or pre-excitation)
- PR appears constant within a given conduction ratio
- QRS may obscure flutter waves - look carefully in II and V1
14. Complete (Third-Degree) Heart Block
ECG Findings:
- Complete AV dissociation - P waves and QRS complexes march independently
- P waves at a faster rate than QRS (e.g., P rate 80/min, QRS rate 30-45/min)
- Narrow QRS if junctional escape rhythm (40-60/min)
- Wide QRS if ventricular escape rhythm (20-40/min) - more dangerous
- Regular P-P and R-R intervals, but P-R intervals vary randomly
- Associated with syncope (Stokes-Adams attacks), hemodynamic compromise
15. First-Degree AV Block
ECG Findings:
- Prolonged PR interval >200 ms (one large box) - constant, every P conducts to QRS
- Normal P wave morphology
- Every P wave followed by a QRS (1:1 conduction maintained)
- QRS typically narrow
- Often benign; seen in athletes, elderly, inferior MI, digoxin toxicity, Lyme disease
16. Second-Degree AV Block - Mobitz Type II (Wenckebach)
ECG Findings:
- Progressive PR prolongation with each beat until a P wave is not conducted (dropped QRS)
- After the dropped beat, PR resets to shortest interval and cycle repeats
- RR intervals progressively shorten before the dropped beat
- Usually narrow QRS; block is at AV node level
- Grouped beating pattern (e.g., 3:2, 4:3 patterns)
17. Left Bundle Branch Block (LBBB)
ECG Findings:
- QRS duration ≥120 ms (wide, slurred)
- Broad, notched R wave in lateral leads (I, aVL, V5-V6) - "M-shaped" or "rabbit-ears"
- Deep S wave or QS pattern in V1 (rS or QS)
- ST and T waves discordant to QRS (ST depression and T inversion in leads with tall R)
- New LBBB in the right clinical context = STEMI equivalent
- Left axis deviation
18. Right Ventricular Hypertrophy / Cor Pulmonale
ECG Findings (Pulmonary Hypertension/Cor Pulmonale):
- Right axis deviation (axis >+100°)
- Dominant R wave in V1 (R/S > 1 in V1)
- S1Q3T3 pattern (in acute PE): S wave in lead I, Q wave in lead III, T-wave inversion in III
- ST depressions in V1-V3 (right ventricular strain)
- Sinus tachycardia
- P-pulmonale (tall peaked P waves in II, III, aVF >2.5 mm)
- Right bundle branch block (RBBB) pattern may develop
19. Mitral Stenosis
ECG Findings:
- P-mitrale (bifid P waves in II, III; duration >120 ms) - left atrial enlargement
- Broad, notched P waves (lead II) and biphasic P waves in V1 (negative terminal component)
- Right axis deviation (from RV pressure overload)
- RVH patterns if pulmonary hypertension develops
- Atrial fibrillation - very common complication (dilated LA becomes arrhythmogenic)
"Abnormalities in the ECG may include atrial fibrillation, left atrial enlargement, or right axis deviation." - Schwartz's Principles of Surgery
20. Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC)
ECG Findings:
- Epsilon wave - small positive deflection at the end of the QRS in V1-V3 (pathognomonic)
- T-wave inversions in right precordial leads V1-V3 (most common finding; present in >85%)
- Right bundle branch block (RBBB) - complete or incomplete
- Prolonged S-wave upstroke in V1-V3 (≥55 ms)
- QRS duration in V1-V3 ≥110 ms
- Ventricular tachycardia with LBBB morphology (origin in RV)
- Right precordial late potentials on signal-averaged ECG
Summary Table
| # | Disease | Key ECG Finding | Leads Affected |
|---|---|---|---|
| 1 | Anterolateral STEMI | ST elevation + Q waves | V1-V6, I, aVL |
| 2 | Inferior STEMI | ST elevation + reciprocal depression | II, III, aVF; reciprocal I, aVL |
| 3 | Posterior MI | Tall R, ST depression (mirror image) | V1-V3 (reciprocal); V8-V9 direct |
| 4 | de Winter Pattern | J-point depression, hyperacute T | V1-V6, ST elevation aVR |
| 5 | High Lateral STEMI | ST elevation I, aVL | I, aVL; reciprocal III, aVF, V1 |
| 6 | WPW | Short PR + delta wave + wide QRS | All leads |
| 7 | Brugada | Coved ST elevation, RBBB pattern | V1-V3 |
| 8 | Long QT Syndrome | Prolonged QTc | All leads |
| 9 | Ventricular Fibrillation | Chaotic, no organized complexes | All leads |
| 10 | HCM | LVH voltage + narrow septal Q waves | V2-V6, I, aVL |
| 11 | Acute Pericarditis | Diffuse ST elevation + PR depression | All leads except aVR, V1 |
| 12 | Atrial Fibrillation | Absent P waves, irregular RR | All leads |
| 13 | Atrial Flutter | Sawtooth flutter waves 300/min | II, III, aVF, V1 |
| 14 | Complete Heart Block | AV dissociation, escape rhythm | All leads |
| 15 | First-Degree AVB | PR >200 ms | All leads |
| 16 | Mobitz I (Wenckebach) | Progressive PR prolongation, dropped QRS | All leads |
| 17 | LBBB | Wide QRS, broad R in lateral leads | I, aVL, V5-V6; QS in V1 |
| 18 | Cor Pulmonale/RVH | Right axis deviation, dominant R in V1 | V1, I, III |
| 19 | Mitral Stenosis | P-mitrale, right axis deviation, AF | II, V1 |
| 20 | ARVC | Epsilon wave, T inversions V1-V3 | V1-V3 |
Sources:
- Rosen's Emergency Medicine, 10e (Coronary artery disease ECG atlas)
- Tintinalli's Emergency Medicine, 9e (HCM, WPW, AV blocks, ARVC)
- Fuster and Hurst's The Heart, 15e (Arrhythmias, channelopathies)
- Miller's Review of Orthopaedics, 9e (WPW, Brugada, Long QT, VF - sudden death in athletes)
- Goldman-Cecil Medicine (VT, LBBB, AV blocks)
- Braunwald's Heart Disease, 2 Vol Set (VT, inherited cardiomyopathies)
- Schwartz's Principles of Surgery, 11e (Valvular disease ECG)
This is a shared conversation. Sign in to Orris to start your own chat.