Thyroglossal cyst
Reading File
Finding Sources
Searching PubMed
thyroglossal duct cyst
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Thyroglossal Duct Cyst (TDC)
Embryology and Pathogenesis
The thyroid gland originates as a median endodermal thickening (thyroid diverticulum) at the foramen cecum at the base of the tongue. It descends through the neck to its definitive pretracheal position while remaining connected to the base of the tongue via the thyroglossal duct. The duct normally obliterates by the 8th-10th week of gestation.
As it descends, the duct is intimately related to the hyoid bone, which forms from the ventral cartilages of the 2nd and 3rd branchial arches at the 7th week of gestation. This anatomic relationship is the basis of the surgical procedure used for treatment.
When any portion of the duct persists and epithelial cells remain, secretions accumulate - forming a cyst anywhere along the duct's path from the foramen cecum to the lower anterior neck.
Epidemiology
- Most common congenital cystic neck mass in children
- Second most common benign neck mass overall, after benign lymphadenopathy
- Most often presents in the pediatric population, though can present at any age
Locations
| Location | Frequency |
|---|---|
| Infrahyoid (below hyoid bone) | ~65% |
| At the level of hyoid bone | ~15% |
| Suprahyoid / near tongue base | remaining |
| Midline | 75% |
| Up to 2 cm off midline | 25% |
Clinical Features
- Painless midline neck mass, most commonly at or just below the hyoid bone
- Pathognomonic sign: moves cranio-caudally with swallowing or tongue protrusion (due to attachment to the foramen cecum via the duct remnant)
- Usually smooth, soft, and fluctuant
- May become infected (from oral bacteria via the tongue) - presenting with pain, redness, and swelling
- Infected cysts may drain and form cutaneous fistulous sinuses
- Rarely causes dysphagia or airway obstruction
- "An upper midline cystic neck lesion in toddlers is a thyroglossal duct cyst until proven otherwise." - Sabiston
Pathology (Histology)
The cyst wall contains:
- Stratified squamous epithelium - near the tongue base
- Pseudostratified ciliated columnar epithelium - in lower locations
- Transitional patterns may also occur
- Fibrous cyst wall often includes lymphoid aggregates and thyroid tissue remnants
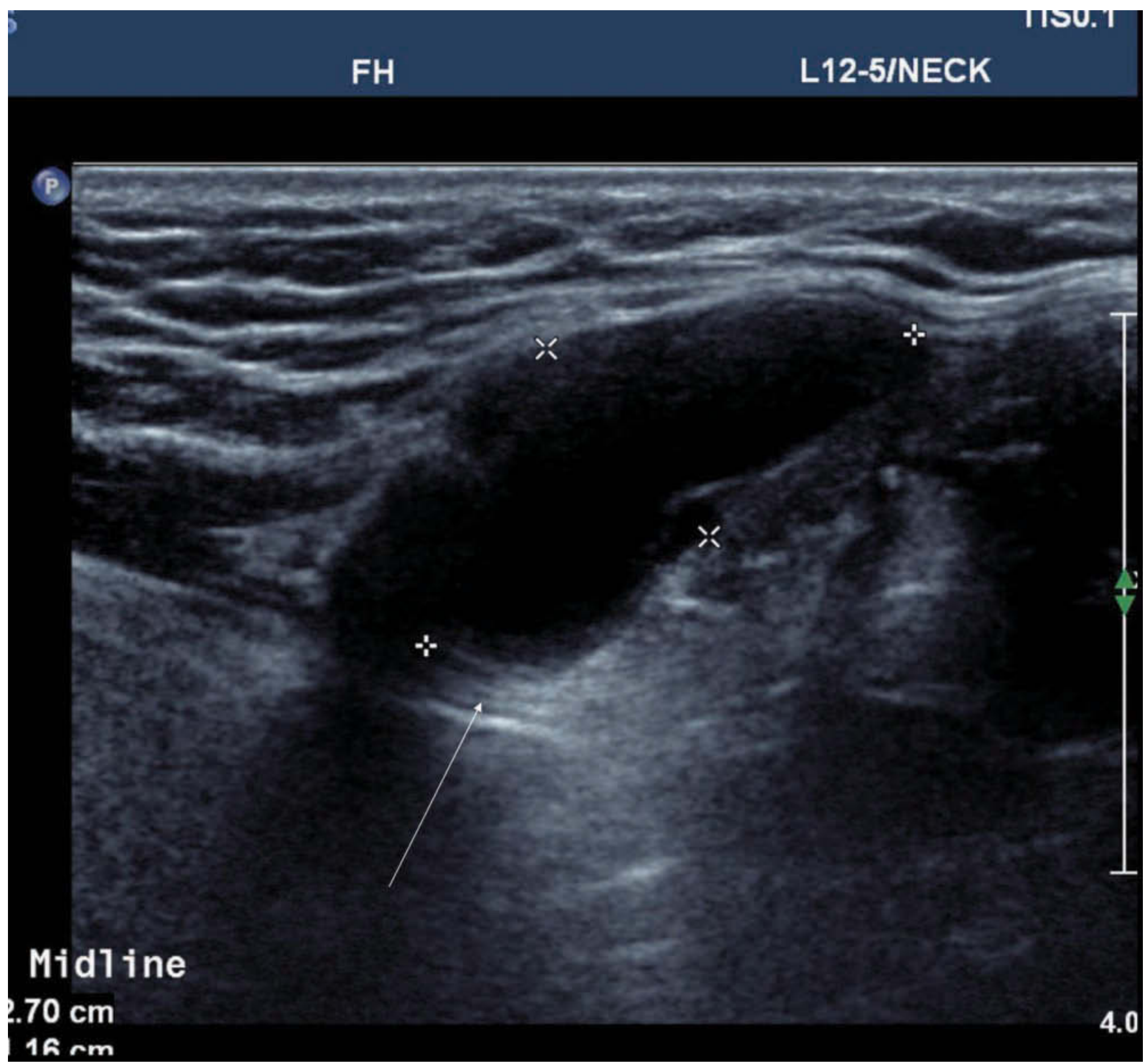
Imaging
Ultrasound (first-line)
Appearance varies:
- Homogeneous anechoic cystic mass with posterior wall enhancement (most classic)
- Pseudosolid mass - due to proteinaceous secretions
- Heterogeneous pattern - due to prior hemorrhage or infection
CT / MRI
- Appearance varies with cyst contents
- On MRI: invariably high T2 signal; T1 signal variable (depends on proteinaceous content)
Key Imaging Points
- Relationship of the TDC to the hyoid bone
- Presence/absence of normal thyroid tissue in the neck (to rule out ectopic/only thyroid tissue in the cyst)
- Any solid component within the cyst - ~1% incidence of carcinoma (classically papillary thyroid carcinoma, PTC)
Diagnosis
- Primarily clinical: characteristic midline mass + history
- Ultrasound confirms the diagnosis and assesses size/location
- CT scan when anatomy is complex or infection is present
- Imaging must confirm the existence of normal orthotopic thyroid tissue before surgery - the TDC may contain the patient's only functional thyroid tissue
- FNA may be performed to exclude other diagnoses or malignancy
Complications
| Complication | Notes |
|---|---|
| Infection/abscess | From oral bacteria; can lead to cutaneous fistula |
| Cutaneous fistula | Post-infection or spontaneous rupture |
| Malignant transformation | ~1% incidence; most commonly papillary thyroid carcinoma |
| Recurrence post-surgery | Up to 40-50% if incompletely excised |
Treatment: The Sistrunk Procedure
The definitive treatment is surgical excision via the Sistrunk procedure (first described in 1920/1928).
Components of the Sistrunk operation:
- Complete excision of the cyst
- Excision of the entire thyroglossal duct tract
- Resection of the central portion of the hyoid bone (the tract passes through it)
- Excision of the tract from hyoid bone to the base of the tongue (toward the foramen cecum)
Resection of a small portion of the tongue base is no longer considered necessary in the majority of cases.
Why the hyoid must be removed: The intimate anatomic relationship of the duct remnant with the central hyoid means incomplete excision leads to recurrence rates of 40-50%. Removing the central hyoid ensures the entire tract is eliminated.
If the cyst is acutely infected, surgery is typically deferred until after a course of antibiotics.
Malignancy in TDC
A recent systematic review (Thimsen et al., 2025 - PMID: 40347268) reviewed TDC carcinomas. The Cummings Otolaryngology textbook highlights well-differentiated thyroid carcinoma (especially PTC) as the classic malignancy arising within TDC. Solid components on imaging warrant FNA or frozen section during surgery.
Differential Diagnosis of Midline Neck Mass
| Diagnosis | Distinguishing Feature |
|---|---|
| Thyroglossal duct cyst | Moves with tongue protrusion; at/below hyoid |
| Dermoid/epidermoid cyst | Does NOT move with tongue protrusion |
| Lingual thyroid | At base of tongue; only thyroid tissue present |
| Submental lymphadenopathy | Reactive; not cystic |
| Thyroid nodule/goiter | Lower in neck; moves with swallowing but not tongue |
| Lipoma | Soft, subcutaneous; not midline-fixed |
Sources: Sabiston Textbook of Surgery; Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Robbins, Cotran & Kumar Pathologic Basis of Disease; Cummings Otolaryngology Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.