Ecg diagnosis common disease
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG diagnosis common diseases electrocardiogram patterns 2025
Finding Sources
Finding Sources
Searching Images
ECG patterns common diseases diagnosis electrocardiogram
Reading File
Reading File
Searching Images
STEMI myocardial infarction ECG ST elevation
Searching Images
atrial fibrillation ECG irregular rhythm no P waves
Searching Images
complete heart block third degree AV block ECG
Searching Images
ventricular tachycardia ECG wide complex tachycardia
Searching Images
pericarditis ECG diffuse ST elevation saddle shape
Searching Images
hyperkalemia ECG peaked T waves wide QRS sine wave
I now have rich image content and textbook data. Let me compile the comprehensive guide.
ECG Diagnosis of Common Diseases
A 12-lead ECG records the heart's electrical activity across 10 electrodes. Systematic interpretation covers: rate → rhythm → axis → intervals (PR, QRS, QT) → P waves → ST segments / T waves → pathological Q waves.
1. Acute Myocardial Infarction (STEMI)
Key ECG features:
- ST elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in ≥2 contiguous precordial leads
- Hyperacute T waves (tall, peaked) in the earliest phase
- Pathological Q waves (>40 ms wide, >25% of R wave amplitude) indicating transmural necrosis
- Reciprocal ST depression in leads facing away from the infarct zone
- New LBBB may be equivalent to STEMI in the right clinical context
Localisation by lead territory:
| Territory | Leads with STE | Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Anterolateral | V1–V6, I, aVL | Proximal LAD |
| Inferior | II, III, aVF | RCA (or LCx) |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | Tall R + ST depression V1–V3 | RCA/LCx |
Tombstone ST elevation (massive convex STE) signals proximal LAD/left main occlusion — immediate reperfusion required.

2. NSTEMI / Unstable Angina
Key ECG features:
- ST depression ≥0.5 mm (horizontal or downsloping) — most specific for subendocardial ischemia
- T-wave inversions — symmetric, deep inversions particularly ominous (Wellens' pattern in V2–V3 = LAD stenosis)
- Normal ECG does NOT exclude NSTEMI (1–6% of ED chest pain patients with normal ECG have NSTEMI)
- Dynamic ECG changes (resolution/worsening with symptoms) confirm ACS
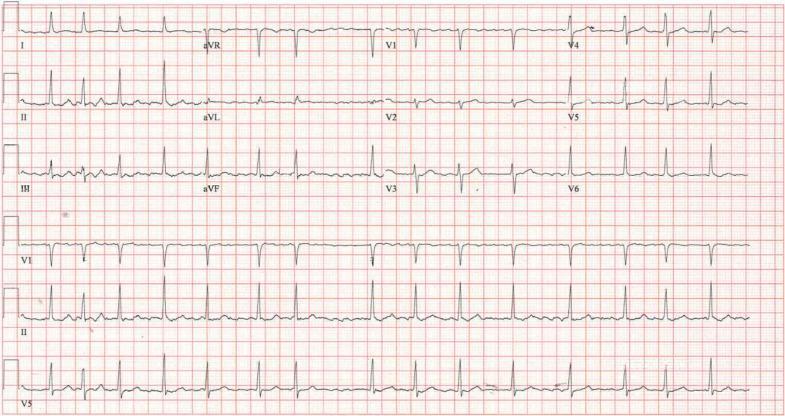
3. Atrial Fibrillation (AF)
Key ECG features:
- Irregularly irregular ventricular rhythm — no two R-R intervals are equal
- Absent P waves — replaced by fine fibrillatory (f) waves, best seen in V1 and lead II
- Narrow QRS (unless aberrant conduction/RBBB/WPW)
- Ventricular rate typically 110–160 bpm in uncontrolled AF
4. Atrial Flutter
Key ECG features:
- Sawtooth flutter waves at ~300 bpm (F waves), best seen in II, III, aVF, V1
- Regular or regularly irregular ventricular rate — most commonly 2:1 block (ventricular rate ~150 bpm)
- Narrow QRS (unless aberrancy)
- Important: a regular tachycardia at exactly 150 bpm should always raise suspicion for flutter with 2:1 block
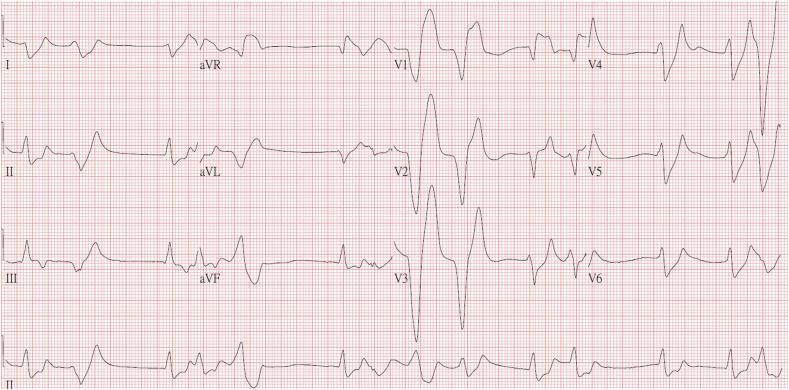
5. Ventricular Tachycardia (VT)
Key ECG features:
- Wide complex tachycardia (QRS >120 ms) at rate >100 bpm
- AV dissociation — independent P waves and QRS complexes (pathognomonic when present)
- Capture beats (narrow complex among wide complexes) and fusion beats
- Positive/negative concordance across all precordial leads
- Rate typically 140–200 bpm; monomorphic (structural disease) vs polymorphic
Brugada criteria favor VT: absence of RS in precordial leads; RS interval >100 ms; AV dissociation; specific morphology criteria.

6. Ventricular Fibrillation (VF)
Key ECG features:
- Chaotic, irregular waveforms with no recognizable QRS complexes or P waves
- Coarse VF (large amplitude) vs fine VF (small amplitude, harder to distinguish from asystole)
- Immediately life-threatening — requires immediate defibrillation
7. Complete (Third-Degree) AV Block
Key ECG features:
- Complete AV dissociation — P waves and QRS bear no relationship
- P rate > QRS rate (e.g., P at 80 bpm, QRS escape at 30–50 bpm)
- Escape rhythm: junctional escape = narrow QRS (40–60 bpm); ventricular escape = wide QRS (20–40 bpm)
- Wide QRS escape = infra-Hisian block = more serious, pacemaker urgently required
8. First- and Second-Degree AV Block
| Type | PR Interval | QRS after each P | Notes |
|---|---|---|---|
| First-degree | >200 ms (>5 small squares) | Yes, always | Benign; often vagal/digoxin |
| Mobitz I (Wenckebach) | Progressive lengthening | Dropped beat after longest PR | Usually nodal; benign |
| Mobitz II | Fixed, normal or prolonged | Suddenly dropped (no warning) | Infra-nodal; risk of CHB; pacemaker often needed |
| 2:1 block | — | Every other P blocked | Can be Mobitz I or II; check context |
9. Bundle Branch Blocks
Left Bundle Branch Block (LBBB)
- QRS ≥120 ms
- Broad monophasic R in I, aVL, V5–V6
- Deep S (or QS) in V1
- No septal Q in lateral leads
- ST/T changes secondary to conduction delay
Right Bundle Branch Block (RBBB)
- QRS ≥120 ms
- rSR' (rabbit ears) in V1–V2
- Wide slurred S in I, V6
- ST depression and T-wave inversion in V1–V3 (secondary changes)
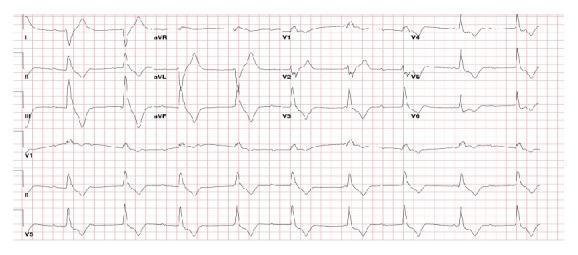
10. Pericarditis
Key ECG features (4 classic stages):
- Diffuse concave ("saddle-shaped") ST elevation in almost all leads EXCEPT aVR and V1 (which show ST depression)
- PR segment depression (most visible in lead II) — highly specific; aVR shows PR elevation
- ST returns to baseline, T waves flatten
- T-wave inversions (weeks later)
- Spodick's sign: downsloping TP segment
Differentiating from STEMI: pericarditis has diffuse distribution (not one coronary territory), concave (not convex) STE, and PR depression.

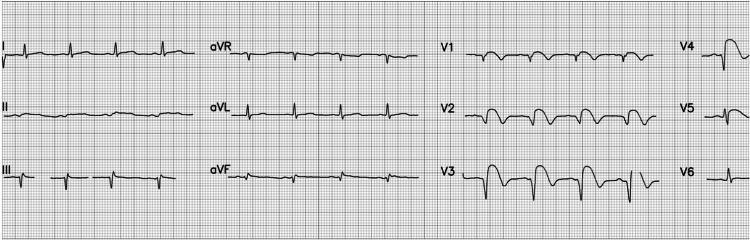
11. Hyperkalemia
Progressive ECG changes with rising K⁺:
| K⁺ Level | ECG Change |
|---|---|
| 5.5–6.5 | Tall peaked ("tented") T waves, narrow base |
| 6.5–7.5 | Prolonged PR, flattened/absent P waves |
| 7.5–8.0 | Widened QRS, left axis deviation |
| >8.0 | Sine-wave pattern, VF, asystole |
12. Pulmonary Embolism (PE)
Key ECG features (none are specific):
- Sinus tachycardia — most common finding
- S1Q3T3 pattern: deep S in I, Q wave and T-wave inversion in III
- Right axis deviation, new RBBB
- T-wave inversions in V1–V4 (right heart strain pattern)
- Sinus tachycardia + right heart strain in clinical context = presumptive PE until proven otherwise
13. WPW (Wolff–Parkinson–White) Syndrome
Key ECG features:
- Short PR interval (<120 ms)
- Delta wave — slurred upstroke of QRS
- Wide QRS (>120 ms)
- Secondary ST/T changes
- Risk of AF conducting rapidly via accessory pathway → can precipitate VF
14. Long QT Syndrome
Key ECG features:
- QTc >440 ms (men) or >460 ms (women) (Bazett's formula: QT ÷ √RR)
- Morphological T-wave changes (notched T, biphasic T)
- Risk of torsades de pointes (TdP) — a polymorphic VT that can degenerate to VF
- Causes: congenital channelopathies, drugs (antiarrhythmics, antibiotics, antipsychotics), hypokalemia, hypomagnesemia
15. Brugada Syndrome
Key ECG features:
- Type 1 (diagnostic): Coved-type ST elevation ≥2 mm with descending ST → negative T wave, in V1–V2 (or high precordial placement)
- Type 2: Saddleback morphology — not diagnostic without provocative test (ajmaline/flecainide)
- Risk of polymorphic VT/VF and sudden cardiac death, typically in young males at night/rest
- ICD is definitive treatment for symptomatic patients
Quick Reference Summary
| Condition | Most Characteristic Feature |
|---|---|
| STEMI | Convex STE in contiguous leads + reciprocal changes |
| AF | Irregularly irregular, absent P waves |
| VT | Wide complex tachycardia + AV dissociation |
| CHB | Independent P & QRS, bradycardia |
| Pericarditis | Diffuse concave STE + PR depression |
| LBBB | Wide QRS, monophasic R in V5–V6 |
| RBBB | Wide QRS, rSR' in V1, slurred S in V6 |
| Hyperkalemia | Peaked T waves → sine wave |
| PE | Sinus tach + S1Q3T3 + right heart strain |
| WPW | Short PR + delta wave |
| Long QT | QTc >440–460 ms |
| Brugada | Coved STE V1–V2, no ischemia |
Sources: Tintinalli's Emergency Medicine (9e), Braunwald's Heart Disease (15e), Rosen's Emergency Medicine — via the medical textbook library.
This is a shared conversation. Sign in to Orris to start your own chat.