Make me understand Glycolysis for usmle step 1
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information to write a thorough USMLE Step 1-focused glycolysis guide. Let me compile the complete answer:
Glycolysis - USMLE Step 1 Master Guide
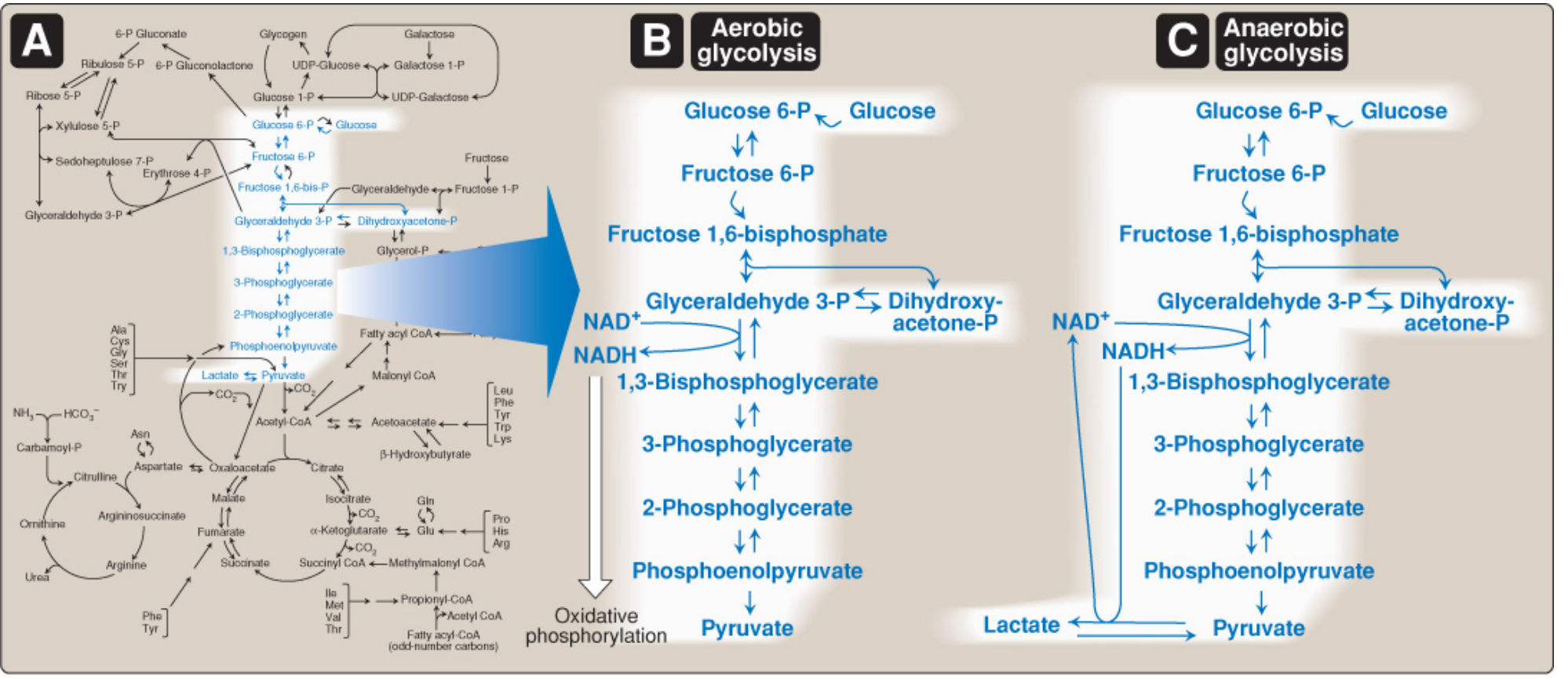
Figure: A) Glycolysis in the context of whole-cell metabolism. B) Aerobic glycolysis. C) Anaerobic glycolysis. (Lippincott Illustrated Reviews: Biochemistry, 8th ed.)
Big Picture
Glycolysis is the universal 10-step cytosolic pathway that converts 1 glucose (6C) into 2 pyruvate (3C). It is the hub of carbohydrate metabolism - nearly every sugar in the body funnels through it. It generates ATP both with and without oxygen, making it the only energy source for certain tissues.
- Location: Cytosol (all 10 enzymes are cytosolic)
- Net yield per glucose: 2 ATP, 2 NADH, 2 pyruvate
- Oxygen requirement: NOT required (anaerobic glycolysis generates ATP without O2)
GLUT Transporters (High-Yield Table)
Glucose cannot diffuse into cells - it requires specific transporters.
| GLUT | Location | Key Feature | Km |
|---|---|---|---|
| GLUT-1 | Most tissues, RBCs, brain | Basal uptake | 1 mM |
| GLUT-2 | Liver, kidney, pancreatic β-cells | Bidirectional; glucose sensor | 15-20 mM (high) |
| GLUT-3 | Brain, neurons | High-affinity brain uptake | 1 mM |
| GLUT-4 | Muscle, adipose tissue | Insulin-dependent | 5 mM |
| GLUT-5 | Small intestine, testes | Fructose transporter | 10 mM |
USMLE pearl: GLUT-2 has a HIGH Km (low affinity) - it only activates in the liver/pancreas when glucose is truly abundant. This is how the pancreatic β-cell "senses" hyperglycemia.
The 10 Steps of Glycolysis
Phase 1: Investment Phase (Steps 1-5) - "Spend 2 ATP"
| Step | Reaction | Enzyme | Key Points |
|---|---|---|---|
| 1 | Glucose → Glucose-6-phosphate (G6P) | Hexokinase (most tissues) / Glucokinase (liver, β-cells) | Irreversible; traps glucose in cell; G6P is a major branch point |
| 2 | G6P → Fructose-6-phosphate (F6P) | Phosphoglucose isomerase | Reversible; aldose-ketose isomerization |
| 3 | F6P → Fructose-1,6-bisphosphate (F1,6BP) | Phosphofructokinase-1 (PFK-1) | Irreversible; RATE-LIMITING STEP; major regulatory point |
| 4 | F1,6BP → DHAP + Glyceraldehyde-3-P | Aldolase | Reversible; splits 6C into two 3C fragments |
| 5 | DHAP → Glyceraldehyde-3-P | Triose phosphate isomerase | Reversible; both fragments now enter ATP-generating phase |
Phase 2: Payoff Phase (Steps 6-10) - "Gain 4 ATP, 2 NADH" (x2, because 2 G3P)
| Step | Reaction | Enzyme | Key Points |
|---|---|---|---|
| 6 | G3P → 1,3-Bisphosphoglycerate | G3P dehydrogenase | Produces NADH; only oxidation step; inhibited by arsenate (uncouples phosphorylation) |
| 7 | 1,3-BPG → 3-Phosphoglycerate | Phosphoglycerate kinase | First ATP generated (substrate-level phosphorylation); can make 2,3-BPG instead (RBC shunt) |
| 8 | 3-PG → 2-Phosphoglycerate | Phosphoglycerate mutase | Reversible |
| 9 | 2-PG → Phosphoenolpyruvate (PEP) | Enolase | Produces high-energy bond; inhibited by fluoride (dental/lab use) |
| 10 | PEP → Pyruvate | Pyruvate kinase | Irreversible; last ATP generated; major regulatory point |
NET Yield Summary
| Per Glucose | |
|---|---|
| ATP used (investment) | 2 |
| ATP produced (payoff) | 4 |
| Net ATP | 2 |
| NADH produced | 2 |
| Pyruvate produced | 2 |
The 3 Irreversible "Key Enzymes" - Highest Yield
These are the enzymes tested most on USMLE because they are regulated, irreversible, and differ from gluconeogenesis.
1. Hexokinase vs. Glucokinase
| Hexokinase | Glucokinase | |
|---|---|---|
| Location | All tissues | Liver, pancreatic β-cells |
| Km | Low (~0.1 mM) - high affinity | High (~10 mM) - low affinity |
| Capacity (Vmax) | Low | High |
| Inhibited by | G6P (product inhibition) | NOT inhibited by G6P |
| Induced by | - | Insulin |
| Role | Constant glucose trapping | Acts only when glucose is HIGH |
USMLE pearl: Glucokinase is the "glucose sensor" of the pancreas. In MODY type 2 (glucokinase gene mutation), fasting hyperglycemia results because the β-cell cannot sense normal glucose levels.
2. Phosphofructokinase-1 (PFK-1) - THE Rate-Limiting Enzyme
PFK-1 is the most important control point of glycolysis.
Activators (stimulate glycolysis when energy is LOW):
- AMP, ADP (low energy signal)
- Fructose-2,6-bisphosphate (F2,6BP) - most potent activator; set by insulin
- Pi
Inhibitors (block glycolysis when energy is HIGH):
- ATP (high energy signal)
- Citrate (TCA cycle intermediate - signals "enough acetyl-CoA")
- Low pH (lactic acidosis acts as a brake)
Fructose-2,6-bisphosphate (F2,6BP) - the master regulator:
- Produced by PFK-2 (a bifunctional enzyme)
- Insulin → dephosphorylates PFK-2 → kinase domain active → more F2,6BP → activates PFK-1 → glycolysis ON
- Glucagon → phosphorylates PFK-2 via cAMP/PKA → phosphatase domain active → less F2,6BP → PFK-1 inhibited → glycolysis OFF, gluconeogenesis ON
- F2,6BP simultaneously inhibits fructose-1,6-bisphosphatase (gluconeogenesis enzyme) - prevents futile cycling
3. Pyruvate Kinase
Converts PEP → Pyruvate; the final step of glycolysis.
Activated by: F1,6BP (feedforward activation - the substrate of an earlier step activates the last step)
Inhibited by: ATP, alanine, acetyl-CoA (signals of energy abundance)
Inhibited by: Glucagon (via phosphorylation in liver)
USMLE pearl: Pyruvate kinase deficiency is the most common cause of hemolytic anemia due to an enzyme defect in glycolysis. RBCs depend entirely on glycolysis for ATP - without it, they cannot maintain membrane integrity and lyse.
Fates of Pyruvate
This is a critical branch point:
O2 available + mitochondria
Glucose → Pyruvate ─────────────────────────────→ Acetyl-CoA (→ TCA cycle)
No O2 / no mitochondria
─────────────────────────────→ Lactate (anaerobic glycolysis)
Aerobic Fate: Pyruvate → Acetyl-CoA
- Enzyme: Pyruvate dehydrogenase complex (PDC)
- Location: Mitochondria
- Cofactors: TPP (B1), Lipoic acid, FAD (B2), NAD+ (B3), CoA (B5) - mnemonic: "Tender Loving Care For Nothing" or TL CoFFee
Anaerobic Fate: Pyruvate → Lactate
- Enzyme: Lactate dehydrogenase (LDH)
- NADH is oxidized back to NAD+ in the process
- This regenerates NAD+ so glycolysis can continue WITHOUT mitochondria
- Net: Glucose → 2 lactate + 2 ATP + 2 H+
Net equation for anaerobic glycolysis:
Glucose + 2 ADP + 2 Pi → 2 Lactate + 2 ATP + 2 H2O + 2 H+
Tissues Dependent on Glycolysis/Anaerobic Glycolysis
| Tissue | Why | Notes |
|---|---|---|
| RBCs | No mitochondria | Entirely dependent; also use pentose phosphate pathway |
| Lens of eye | Few/no mitochondria | Cataracts if glycolysis impaired |
| Cornea | Poor O2 delivery | |
| Renal medulla | Hypoxic environment | |
| Leukocytes | High glycolytic demand during phagocytosis | |
| Brain | During hypoxia/ischemia | Usually uses aerobic glycolysis; switches to anaerobic under stress |
| Skeletal muscle | During intense exercise | Warburg effect in tumors too |
The 2,3-BPG Shunt (High-Yield for RBCs)
In RBCs, some 1,3-BPG is diverted away from ATP production:
1,3-BPG → 2,3-Bisphosphoglycerate (2,3-BPG) → 3-Phosphoglycerate
- 2,3-BPG binds to deoxyhemoglobin and decreases O2 affinity (right-shifts the O2-Hb dissociation curve)
- This means tissues get MORE O2 when 2,3-BPG is high
- Increases with: altitude, anemia, hypoxia, acidosis (right shift)
- Stored blood (blood bank) has LOW 2,3-BPG → hemoglobin holds O2 tightly → less O2 delivery to tissues
Clinically Tested Glycolysis Associations
| Condition | Mechanism | Key Fact |
|---|---|---|
| Pyruvate kinase deficiency | No ATP in RBCs → hemolysis | Most common hereditary RBC enzyme deficiency; autosomal recessive |
| Hexokinase deficiency | Rare hemolytic anemia | Less common than PK deficiency |
| Lactic acidosis | Excess anaerobic glycolysis → excess H+ | Seen in: shock, metformin toxicity, thiamine deficiency, cyanide poisoning |
| Warburg effect | Tumors use aerobic glycolysis preferentially even with O2 | Basis of PET scans (FDG uptake); produces more biosynthetic precursors |
| Thiamine (B1) deficiency | Pyruvate cannot enter TCA (PDC requires TPP) → pyruvate backs up → converts to lactate | Wernicke's, beriberi; elevated pyruvate/lactate ratio |
| MODY type 2 | Glucokinase mutation → impaired glucose sensing | Mild persistent fasting hyperglycemia; treated with diet only |
| Arsenic poisoning | Arsenate replaces Pi in G3P dehydrogenase reaction → 1-arseno-3-PG spontaneously hydrolyzes → ATP not made | Uncouples substrate-level phosphorylation at step 6 |
Regulation Summary Table
| Enzyme | Activated by | Inhibited by |
|---|---|---|
| Hexokinase | - | G6P |
| Glucokinase | Insulin (induction) | - |
| PFK-1 | AMP, ADP, F2,6BP, Pi | ATP, citrate, low pH |
| Pyruvate kinase | F1,6BP | ATP, alanine, acetyl-CoA, glucagon |
High-Yield Mnemonics
10 Steps of Glycolysis (enzymes in order):
Happy People Always Think Positively, Giving People Enough Peace
- Hexokinase
- Phosphoglucose isomerase
- Phosphofructokinase-1
- Aldolase
- Triose phosphate isomerase
- Glyceraldehyde-3-phosphate dehydrogenase
- Phosphoglycerate kinase
- Phosphoglycerate mutase
- Enolase
- Pyruvate kinase
3 Irreversible Steps (Hexokinase, PFK-1, Pyruvate Kinase):
"Hexokinase Produces Pretty" (H-P-P) = Irreversible
Pyruvate dehydrogenase cofactors:
"The Lovely Factors Are Named" = TPP, Lipoic acid, FAD, Arsenic... no: NAD+, CoA Better mnemonic: "Tender Loving Care For Nerds" = TPP, Lipoic acid, CoA, FAD, NAD+
USMLE-Style Clinical Vignette
Vignette: A 2-year-old presents with jaundice, splenomegaly, and a hemolytic anemia. Osmotic fragility test is normal. Heinz bodies are absent. The blood smear shows no spherocytes. Enzyme assay shows decreased activity of the final enzyme of glycolysis.
Answer: Pyruvate kinase deficiency. No mitochondria in RBCs → glycolysis is the only ATP source → PK deficiency → ATP depletion → RBC membrane pump failure → hemolysis. Note: G6PD deficiency would show Heinz bodies and bite cells; spherocytes suggest hereditary spherocytosis.
Sources:
- Lippincott Illustrated Reviews: Biochemistry, 8th ed., Chapter 8 (p. 294-310)
- Basic Medical Biochemistry: A Clinical Approach, 6th ed., Chapter 22 (p. 791-810)
This is a shared conversation. Sign in to Orris to start your own chat.