Patient has pain at anterior side of shoulder and on clavicle and on sternoclavicular joint
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Searching the Web
anterior shoulder pain sternoclavicular joint clavicle differential diagnosis 2025
I now have all the information needed for a comprehensive, well-cited answer. Here is a full clinical breakdown:
Pain at the Anterior Shoulder, Clavicle, and Sternoclavicular (SC) Joint
The combination of pain across these three anatomical zones - anterior shoulder, along the clavicle, and at the sternoclavicular (SC) joint - points to a cluster of diagnoses that must be worked through systematically. The SC joint is the only bony link connecting the upper limb to the axial skeleton, and it sits immediately anterior to critical mediastinal structures (great vessels, trachea, esophagus), making some of these diagnoses time-sensitive.
Differential Diagnosis
1. Sternoclavicular Joint Dislocation / Subluxation (Traumatic)
This is the most common traumatic diagnosis in this region. - Rosen's Emergency Medicine, p. 651
Mechanism: Indirect force on the posterolateral shoulder (e.g., motor vehicle collision, contact sports). Anterior dislocations are far more common.
Grading (Rosen's):
- Grade I - Mild sprain of SC and costoclavicular ligaments; joint stable
- Grade II - Subluxation due to SC ligament and capsule disruption
- Grade III - True dislocation; complete rupture of both SC and costoclavicular ligaments
Clinical features of anterior dislocation:
- Prominent, palpable medial end of clavicle displaced anteriorly
- Pain with any movement of the upper extremity
- Arm held in flexion at elbow, supported across trunk
- SC joint swollen and tender on palpation
- Crepitus may be present
Posterior dislocation (less common, more dangerous):
- More painful than anterior
- Red-flag signs: hoarseness, dysphagia, dyspnea, venous congestion of the neck, cyanosis, upper limb paresthesias
- Can compress or lacerate great vessels, trachea, esophagus
- 25% of posterior dislocations have life-threatening complications
Red Flag: In younger patients (<25 years), apparent SC "dislocation" is often a Salter-Harris type I/II physeal injury through the medial clavicular epiphysis (which does not fuse until age 23-25). - Rockwood and Green's Fractures, p. 1092
2. Medial Clavicle Fracture
A direct or indirect blow can fracture the medial third of the clavicle without SC joint involvement. Medial clavicle fractures are notoriously difficult to assess on plain radiographs; CT is the investigation of choice. - Rockwood and Green's Fractures in Adults 10th Ed
Differential for traumatic SC joint pain includes: medial clavicle fracture, rib fracture, costochondral injury, sternum fracture, SC dislocation, contusion, mediastinal injury, pneumothorax. - Rosen's Emergency Medicine
3. SC Joint Inflammatory Arthritis (Non-traumatic)
Inflammatory arthritis of the SC joint is associated with:
- Rheumatoid arthritis (RA)
- Psoriatic arthritis
- Ankylosing spondylitis
- Palmoplantar pustulosis (SAPHO syndrome)
- Septic arthritis (especially in IV drug users - Pseudomonas is common)
"The sternoclavicular joint should be considered a source of neck pain that is perceived anteriorly." - Rheumatology 2-Volume Set (Elsevier, 2022)
4. Septic Arthritis of the SC Joint
SC joint septic arthritis is seen especially in:
- IV drug users (Pseudomonas aeruginosa is common)
- Immunocompromised patients
- Patients with indwelling subclavian catheters
Ultrasound can detect joint effusion. This diagnosis must not be missed. - Firestein & Kelley's Textbook of Rheumatology
5. Condensing Osteitis of the Medial Clavicle
-
Most common in women of late childbearing age
-
Painful swelling over the medial one-third of the clavicle
-
Radiographs show sclerosis; similar to condensing osteitis of the ilium/pubis
-
Benign, idiopathic, self-limiting
-
Also called aseptic enlarging osteosclerosis of the clavicle
-
Firestein & Kelley's Textbook of Rheumatology; Rockwood and Green's Fractures
6. Friedrich's Disease (Osteonecrosis of the Medial Clavicle)
- Painful osteonecrosis of the sternal end of the clavicle
- Predominantly in women
- Rare but must be distinguished from infection and malignancy
7. Tietze's Syndrome
- Painful, non-suppurative swelling of the SC joint and adjacent sternochondral junctions
- Presents with localized tenderness and swelling at the SC joint / medial clavicle area
- Self-limiting
8. SC Hyperostosis (SAPHO Syndrome)
- Inflammatory condition causing new bone formation and potential ankylosis of the SC joint and medial ribs
- Associated with Japanese ethnicity and dermatologic lesions (palmoplantar pustulosis)
- Also classified under SAPHO (Synovitis, Acne, Pustulosis, Hyperostosis, Osteitis)
9. Referred Pain / Cervical Spine Pathology
-
About 5% of patients presenting with shoulder pain have an isolated cervical spine disorder as the cause
-
The SC joint can refer pain to the neck and anterior chest
-
Always examine the cervical spine in any shoulder pain patient
-
Campbell's Operative Orthopaedics 15th Ed 2026
Physical Examination Approach
Per Campbell's Operative Orthopaedics (15th Ed, 2026):
- Inspection: Compare both shoulders - look for asymmetry, swelling, deformity, ecchymosis
- Palpation: Systematically palpate the SC joint, clavicle, AC joint, and acromion - tenderness localizes the pathology
- Range of motion: Active and passive; note painful arcs
- Neurovascular exam: Both upper extremities - assess for brachial plexus or vascular compromise
- Cervical spine: Examine to rule out referred pain
- Airway/breathing assessment: If SC involvement - check for jugular venous distension, hoarseness, dyspnea (posterior dislocation warning signs)
Investigations
| Test | Indication |
|---|---|
| AP chest X-ray + clavicle views + serendipity view (40° cephalic tilt) | First-line imaging for SC region |
| CT scan | Investigation of choice - best for SC dislocation, medial clavicle fracture, physeal injury |
| MRI | Soft tissue assessment, osteonecrosis (Friedrich's), stress edema |
| Ultrasound | Effusion detection (septic arthritis) |
| Blood cultures / joint aspiration | Suspected septic arthritis |
| CRP, ESR, RF, HLA-B27 | Inflammatory arthritis workup |
Summary Table
| Diagnosis | Key Feature |
|---|---|
| SC dislocation (anterior) | Trauma; prominent medial clavicle; crepitus |
| SC dislocation (posterior) | Trauma; hoarseness, dyspnea - emergency |
| Medial clavicle fracture | Direct trauma; needs CT |
| Septic arthritis SC joint | IV drug use, immunosuppression; fever |
| Condensing osteitis | Middle-aged women; sclerosis on X-ray |
| Friedrich's disease | Osteonecrosis medial clavicle; women |
| Tietze's syndrome | Non-suppurative swelling; SC + sternochondral |
| Inflammatory arthritis (RA/PsA/AS) | Bilateral, systemic features |
| SAPHO/SC hyperostosis | Pustulosis; ankylosis; Asian ethnicity |
| Cervical spine referred pain | Neck movement reproduces symptoms |
Clinical bottom line: In a trauma setting, rule out posterior SC dislocation first (life-threatening). In a non-traumatic setting, the combination of anterior shoulder + clavicle + SC joint pain most commonly points to SC joint subluxation/ligament injury, inflammatory arthritis, or one of the medial clavicle-specific conditions (condensing osteitis, Friedrich's). CT scan of the SC region is the most informative single investigation. - Rockwood and Green's Fractures in Adults 10th Ed 2025; Campbell's Operative Orthopaedics 15th Ed 2026; Firestein & Kelley's Textbook of Rheumatology
Patient has sitting job like sewing on table
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
I have all the key information. Here is the updated, integrated clinical analysis:
Updated Clinical Picture: Occupational Context - Sedentary Sewing Job
The occupational history of prolonged sitting + fine repetitive upper limb work at a table (like sewing) dramatically shifts the diagnostic thinking. This pattern causes:
- Sustained forward head posture + protracted shoulders
- Chronic muscle overload of the neck, shoulder girdle, and pectoral muscles
- Narrowing of the costoclavicular and thoracic outlet spaces
- Microtrauma to SC joint ligaments from repetitive arm/shoulder cycling
This means the pain triad (anterior shoulder + clavicle + SC joint) in this patient is most likely postural/overuse in origin, not traumatic.
Top Diagnoses in This Occupational Context
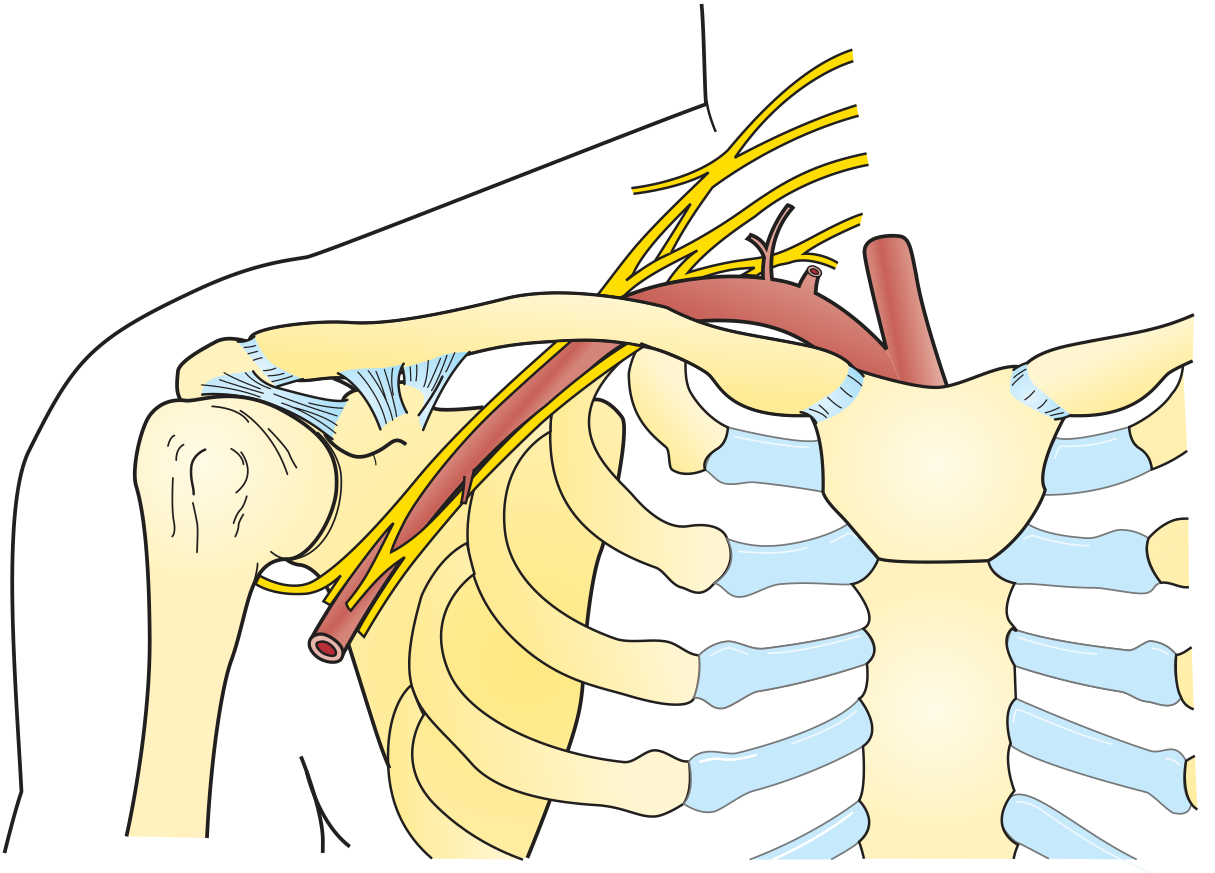
1. Costoclavicular Syndrome (a subtype of Thoracic Outlet Syndrome)
This is the most clinically fitting diagnosis given the history.
"Narrowing of the costoclavicular space is most common in persons with drooping shoulders, a flat back, retracted shoulders (from carrying heavy loads), a deformed first rib, or a previous clavicular fracture. Any narrowing of the costoclavicular space can be aggravated by lowering and retracting the shoulder girdle."
- Thieme Atlas of Anatomy (General Anatomy and Musculoskeletal System)
What happens in a sewing worker:
- Prolonged sitting rounds the thoracic spine and drops the shoulders forward and downward
- This narrows the space between the clavicle and first rib
- The neurovascular bundle (subclavian artery/vein + brachial plexus) gets compressed
- Results in anterior shoulder/clavicle aching, arm heaviness, and SC joint soreness
Symptoms to ask about:
- Arm or hand tingling/numbness (especially ulnar distribution)
- Heaviness or fatigue in the arm after sewing for a while
- Venous swelling of the hand/forearm
- Pain that worsens as the day progresses (worse with prolonged sitting)
- Relief when lying down or elevating the arm
Provocative tests:
-
Costoclavicular maneuver: Posterior rotation of the shoulders - reproduces symptoms
-
Adson's test: Head rotated to affected side + deep inspiration - radial pulse diminishes
-
EAST test (Elevated arm stress test): Arms raised 90°, open/close hands for 3 min - reproduces symptoms
-
Harrison's Principles of Internal Medicine 22E (2025); Thieme Atlas of Anatomy
2. Myofascial Pain Syndrome - Trapezius / Levator Scapulae / Pectoralis Minor
Classic occupational condition in seamstresses, typists, and assembly-line workers.
"In the upper part of the trunk, a common trigger point cluster involves the muscles of the neck and shoulder area, including the trapezius, levator scapulae, and infraspinatus muscles."
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Mechanism in sewing:
- Sustained isometric contraction of the upper trapezius (holding the arm up to sew)
- Pectoralis minor overactivity from protracted posture
- This overactivity of pectorals + weakness of upper trapezius leads to:
- Subacromial impingement symptoms
- Thoracic outlet syndrome symptoms
- Anterior shoulder and SC joint referred pain
"Excessive depression of the scapula... weakness of the upper trapezius or overactivity of the pectorals and latissimus dorsi can lead to pain and symptoms of subacromial impingement or brachialgia and thoracic outlet syndrome."
- Rheumatology 2-Volume Set (Elsevier 2022)
Clinical finding: Tender trigger points in the upper trapezius, levator scapulae, pectoralis minor; pain reproduced by palpation.
3. SC Joint Stress / Overuse Subluxation
The SC joint is stressed by repetitive shoulder cycling during sewing (arm moves forward/backward thousands of times per day). This can cause:
- Ligamentous laxity and microinstability at the SC joint
- Painful subluxation with palpable crepitus
- Localized SC joint tenderness
"The most common problem involves ligamentous injury and painful subluxation, which can be diagnosed by palpable instability and crepitus over the sternoclavicular joint."
- Firestein & Kelley's Textbook of Rheumatology
4. Thoracic Outlet Syndrome - Neurogenic Form
More broadly, any sustained posture compressing structures between the scalene triangle, costoclavicular space, or under pectoralis minor can produce:
- Anterior shoulder + clavicular aching
- Radiating arm pain (often ulnar)
- Paresthesias in the hand
The three anatomical compression zones are:
- Interscalene space (scalene syndrome - cervical rib or muscle)
- Costoclavicular space between clavicle and first rib - most relevant here
- Sub-pectoralis minor space (hyperabduction syndrome)
- Thieme Atlas of Anatomy; Harrison's Principles of Internal Medicine 22E
5. SC Joint Osteoarthritis / Inflammatory Flare
Repetitive low-grade stress on the SC joint from years of sewing can result in:
- Degenerative OA of the SC joint (common in middle-aged to older patients)
- Appears as pseudosubluxation anteriorly on imaging
- Pain and stiffness worse after prolonged use, eases with rest
Revised Diagnostic Priority in This Patient
| Priority | Diagnosis | Key Occupational Link |
|---|---|---|
| 1st | Costoclavicular syndrome (TOS variant) | Drooped shoulders from prolonged sitting |
| 2nd | Myofascial pain - trapezius/pectoralis | Sustained isometric contraction during sewing |
| 3rd | SC joint overuse subluxation/laxity | Repetitive arm cycling at work |
| 4th | SC joint OA | Chronic low-grade stress accumulation |
| 5th | Subacromial impingement | Protracted shoulder posture |
What to Look For in Examination
- Posture assessment: Rounded shoulders? Forward head? Thoracic kyphosis?
- SC joint palpation: Tenderness, swelling, crepitus, subluxation
- Costoclavicular maneuver and Adson's test to reproduce symptoms
- Trigger points: Upper trapezius, pectoralis minor, levator scapulae
- Neurological screen: Sensation in medial forearm + hand (ulnar nerve territory)
- Pulse comparison in provocative positions
Investigations
| Test | Purpose |
|---|---|
| Chest X-ray | Cervical rib? Drooped clavicle? |
| CT of thoracic outlet / SC joint | Costoclavicular space measurement; SC OA |
| Nerve conduction / EMG | Rule out neurogenic TOS |
| Doppler ultrasound | Vascular TOS screening |
| MRI shoulder | Rotator cuff, impingement, SC joint |
Management Principles
- Ergonomic correction - raise the sewing table height, use armrests, support the forearms
- Postural exercises - shoulder retraction, chin tucks, thoracic extension
- Physiotherapy - trigger point release, scapular stabilization exercises
- NSAIDs for pain control
- Rest breaks every 30-45 minutes during work
- Surgical decompression (first rib resection) only if conservative management fails over 3-6 months - Harrison's Principles of Internal Medicine 22E (2025)
This is a shared conversation. Sign in to Orris to start your own chat.