Mechanism of hypermelanosis in Addison disease
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a complete, textbook-sourced explanation of the mechanism.
Mechanism of Hypermelanosis in Addison Disease
The Core Pathway: Loss of Negative Feedback
In primary adrenal insufficiency (Addison disease), the adrenal cortex is destroyed and fails to produce cortisol. Normally, cortisol exerts negative feedback on both the hypothalamus and the anterior pituitary to suppress secretion of CRH and ACTH respectively. When this feedback is lost, the pituitary corticotroph cells become hyperactive and massively upregulate transcription of the POMC gene.
"Persistently low cortisol levels do not provide negative regulatory feedback to the hypothalamus and pituitary. This results in unchecked production of POMC, ACTH, and melanocyte-stimulating hormone, which increase melanogenesis."
- Fitzpatrick's Dermatology, p. 2543
POMC: The Key Precursor Molecule
Pro-opiomelanocortin (POMC) is a single large precursor polypeptide synthesised by the corticotroph cells of the anterior pituitary. Endopeptidases cleave it into several biologically active fragments simultaneously:
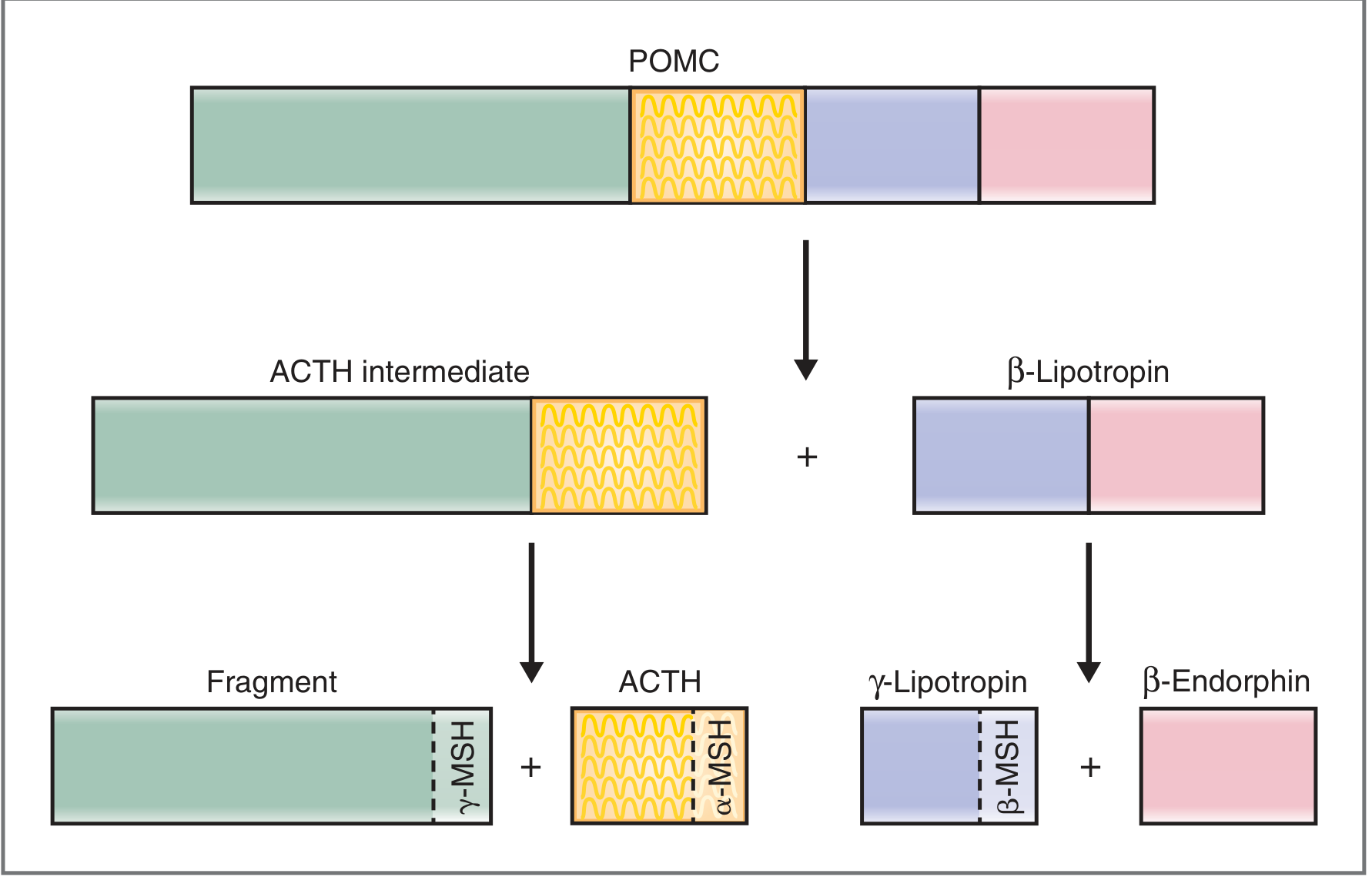
Fig. 9.10 - Hormones derived from POMC. Note that MSH activity is embedded in three separate fragments. (Costanzo Physiology, 7th ed., p. 414)
The critical point is that MSH sequences are embedded within the POMC molecule at multiple sites:
- The fragment (leftover from ACTH intermediate cleavage) contains γ-MSH
- ACTH itself contains α-MSH within its sequence
- γ-Lipotropin contains β-MSH
Because POMC and ACTH are elevated together in Addison disease, all three MSH-containing fragments are simultaneously elevated.
How MSH Causes Hyperpigmentation
MSH (especially α-MSH) acts on MC1R (melanocortin-1 receptor) on dermal and epidermal melanocytes. This receptor activation:
- Stimulates adenylyl cyclase → cAMP signalling
- Upregulates tyrosinase activity (the rate-limiting enzyme in melanin synthesis)
- Increases production and transfer of eumelanin (dark melanin) to surrounding keratinocytes
ACTH itself also has direct melanotrophic activity since it contains the α-MSH sequence, compounding the effect.
Why Hyperpigmentation is NOT Seen in Secondary/Tertiary Adrenal Insufficiency
This is a diagnostically important distinction:
| Feature | Primary (Addison) | Secondary (pituitary) | Tertiary (hypothalamic) |
|---|---|---|---|
| ACTH level | High | Low | Low |
| POMC/MSH level | High | Low | Low |
| Hyperpigmentation | Present | Absent | Absent |
In secondary and tertiary adrenal insufficiency, the pituitary either cannot produce ACTH (e.g., pituitary adenoma destroying corticotrophs) or lacks CRH stimulation. POMC and MSH levels are therefore low, and no pigmentary change occurs - Robbins, Cotran & Kumar, p. 1037.
Clinical Distribution of Hyperpigmentation
The pigmentation is generalised but accentuated in:
- Sun-exposed areas (face, neck, dorsum of hands) - UV also stimulates local MSH release
- Pressure points - elbows, knees, knuckles
- Flexural folds and skin creases, including palmar creases
- Scars (new scars formed during the disease show enhanced pigmentation)
- Oral mucosa - buccal mucosa patches
- Nails - longitudinal pigmented bands
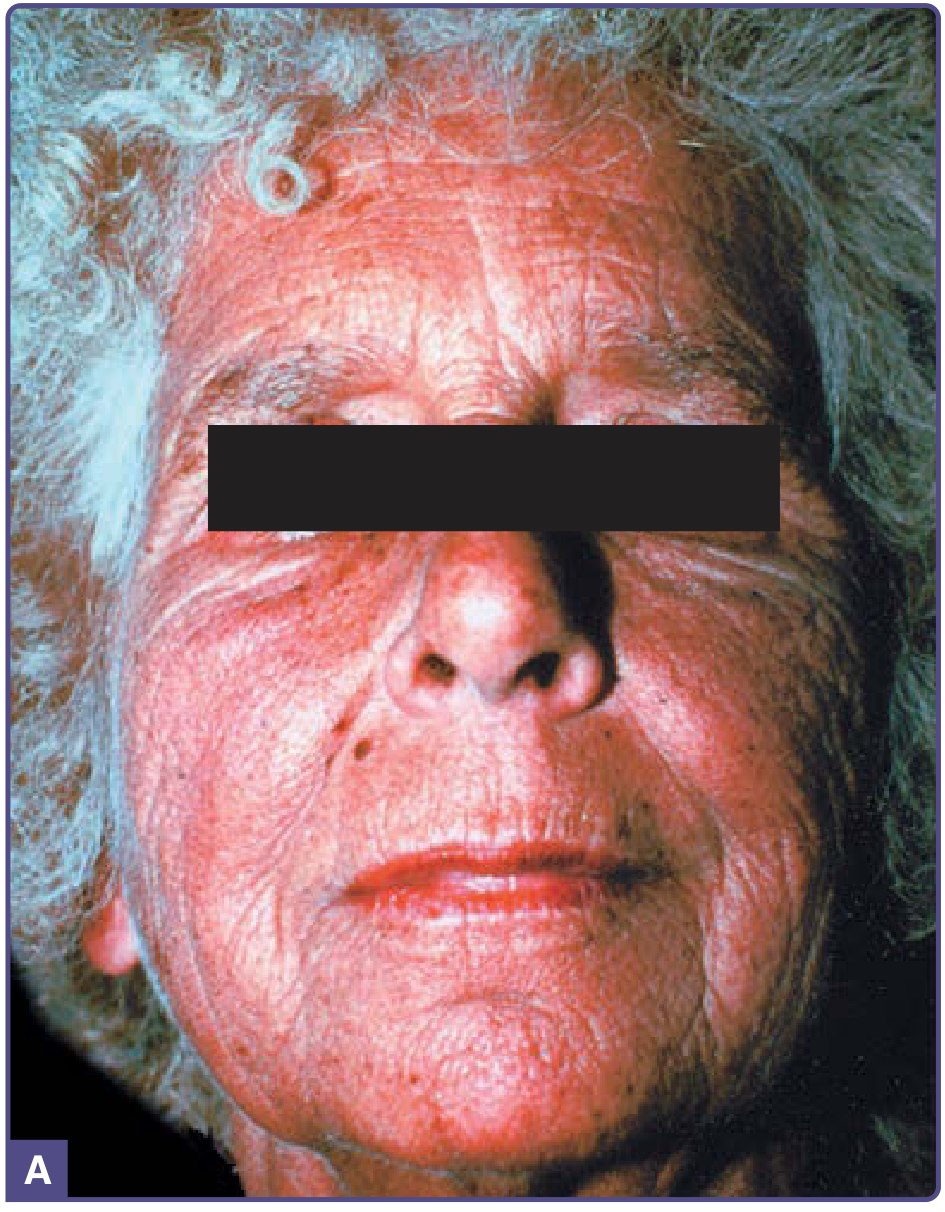

Clinical photos from Fitzpatrick's Dermatology, Fig. 137-12.
Summary Flowchart
Adrenal cortex destruction
↓
↓ Cortisol
↓
Loss of negative feedback on pituitary/hypothalamus
↓
↑ POMC transcription (corticotrophs)
↓
↑ POMC cleavage → ↑ ACTH + ↑ α-MSH + ↑ β-MSH + ↑ γ-MSH
↓
MSH binds MC1R on melanocytes
↓
↑ Tyrosinase → ↑ Melanin synthesis
↓
Generalised hyperpigmentation
Key point to remember: The hyperpigmentation is a marker of primary adrenal failure specifically - its presence implies the pituitary-hypothalamic axis is intact and responding normally to low cortisol. Its absence in secondary adrenocortical insufficiency is an equally useful clinical clue.
Sources: Costanzo Physiology 7th ed., p. 414; Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1037; Fitzpatrick's Dermatology, p. 2543; Dermatology 2-Volume Set 5e.
This is a shared conversation. Sign in to Orris to start your own chat.