1 year old with severe ascariasis
Reading File
Finding Sources
Finding Sources
Searching PubMed
ascariasis children treatment anthelmintic
Reading File
Reading File
Reading File
Searching PubMed
ascariasis infant treatment albendazole mebendazole
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Searching the Web
ascariasis treatment 1 year old infant albendazole safe dose WHO guidelines
Loading Image
Finding Sources
I now have everything needed for a thorough, well-cited answer. Here is the complete clinical review:
Severe Ascariasis in a 1-Year-Old
This is a special-population pediatric case requiring careful attention to drug dosing, complications common in young children, and surgical thresholds.
The Pathogen
Ascaris lumbricoides is the largest intestinal nematode infecting humans (15-40 cm long). Eggs ingested from fecally contaminated soil hatch in the gut, larvae penetrate the intestinal wall, migrate through the portal circulation to the lungs, ascend the bronchial tree, are swallowed, and mature into adult worms in the small intestine - a process taking 2-3 months. Each female produces >200,000 eggs/day. Adult worms live 1-2 years.
Prevalence and intensity of infection peak in the first 2-3 years of life due to oral hand-to-mouth behavior and immature hygiene. The smaller lumen of an infant's intestine makes bowel obstruction far more likely than in adults. - Goldman-Cecil Medicine, p. 3475
Why "Severe" in a 1-Year-Old Is a Medical Emergency
Severity in this age group arises from two phases:
1. Pulmonary Phase (Loeffler Syndrome)
- Larvae traversing alveoli cause eosinophilic pneumonitis (Loeffler syndrome): wheezing, dyspnea, paroxysmal nonproductive cough, high fever, urticaria, angioedema
- Peripheral eosinophilia and transient infiltrates on CXR
- Larvae (not eggs) may be found in sputum/gastric aspirates at this stage
- Self-limited (2-3 weeks), but distressing and potentially severe in infants
2. Intestinal Phase - Complications (especially severe at age 1)
| Complication | Features in infants |
|---|---|
| Intestinal obstruction | Most common severe complication; small lumen = higher risk; presents as colicky pain, vomiting, abdominal distension, palpable worm mass |
| Biliary/pancreatic duct invasion | Worms migrate into biliary tree or pancreatic duct → cholangitis, jaundice, pancreatitis |
| Appendiceal invasion | Can mimic appendicitis |
| Malnutrition/malabsorption | Decreased fat/protein absorption, vitamin A and C deficiency, lactose intolerance → stunted growth, impaired cognitive development |
| Volvulus, intussusception, perforation | Rare but life-threatening; require surgery |
- Harrison's Principles, 22e, p. 1858; Goldman-Cecil Medicine, p. 3476
Diagnosis
| Method | Notes |
|---|---|
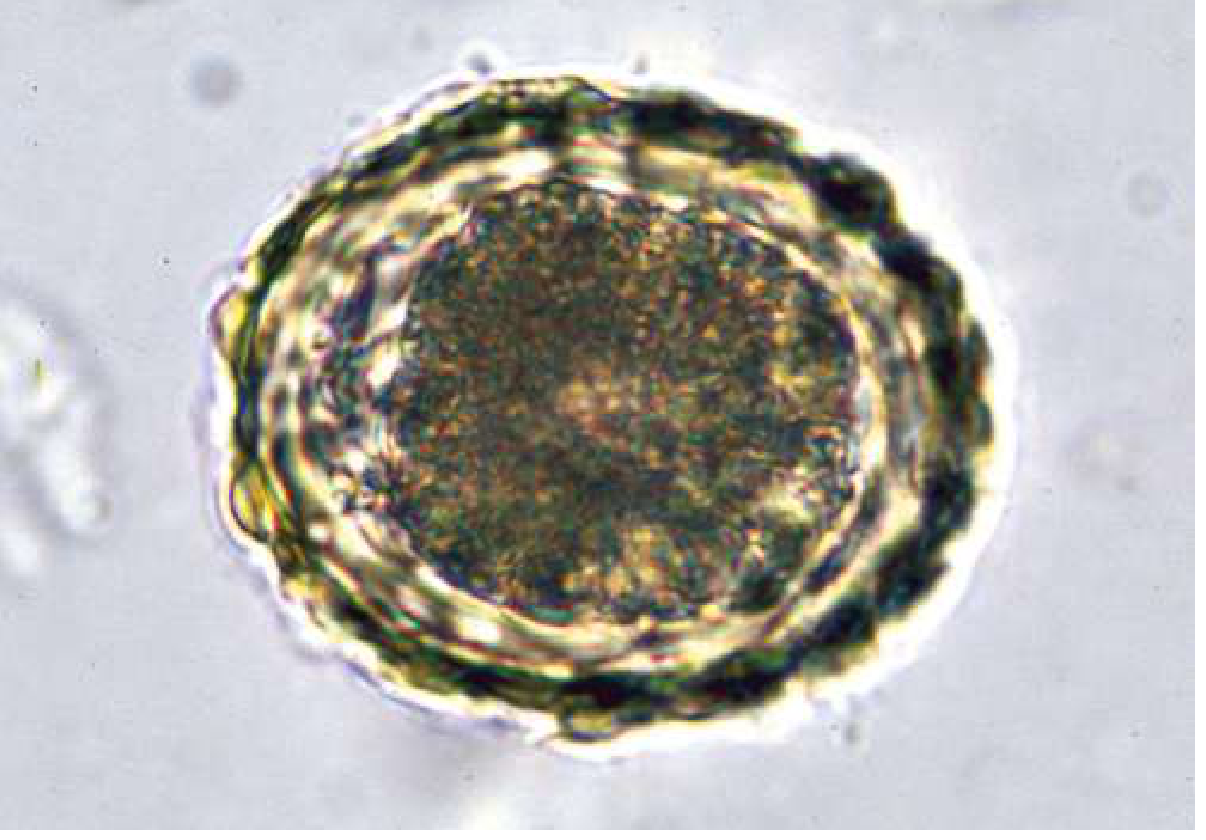
| Stool microscopy | Characteristic thick-shelled fertilized eggs (~65 × 45 µm); standard first test |
| Stool PCR | More sensitive/specific; research/specialized labs |
| Sputum/gastric aspirate | Larvae during pulmonary phase |
| Abdominal X-ray | Worm mass in gas-filled loops during obstruction |
| Abdominal ultrasound | Worms in intestine, bile ducts, or pancreatic duct |
| ERCP | Biliary/pancreatic Ascaris; also therapeutic |
Treatment
⚠️ Age-Specific Drug Dosing (Critical for a 1-Year-Old)
| Drug | Standard Adult/Older Child Dose | Dose for Child <2 Years (Age 1) |
|---|---|---|
| Albendazole (first-line) | 400 mg single dose | 200 mg single dose (WHO recommendation for children <24 months) |
| Mebendazole | 100 mg BID × 3 days OR 500 mg once | 100 mg BID × 3 days (same dose; safe in children) |
| Pyrantel pamoate | 11 mg/kg once (max 1 g) | 11 mg/kg once - weight-based, safe in infants |
| Ivermectin | 150-200 µg/kg once | Use with caution; safety unclear in children <15 kg |
Key points on albendazole safety in infants:
- The FDA notes safety is "uncertain" in children under 6 years, but studies using albendazole in children as young as 1 year suggest it is safe
- WHO guidelines for mass drug administration include children aged 12-23 months at a half-dose (200 mg)
- Ascariasis should always be treated even if asymptomatic - to prevent serious complications - Harrison's, 22e, p. 1859
Sources: CDC STH clinical care guidelines, WHO deworming recommendations, Goldman-Cecil Medicine Table 327-1
Pulmonary Ascariasis (Severe Loeffler Syndrome)
- No anthelmintic is needed in the pulmonary phase alone (self-limited)
- If severe pneumonitis: corticosteroids to reduce inflammation
- In cases with ongoing pulmonary + intestinal involvement: 2 doses of albendazole (200 mg in this age group) one month apart - the first kills mature intestinal worms, the second kills those that were still migrating during the first dose
- Sleisenger & Fordtran's GI Disease, p. 2267
Intestinal Obstruction (Management Algorithm)
Partial obstruction → Conservative management:
• IV fluid resuscitation
• Nasogastric (NG) decompression
• IV antibiotics
• Piperazine instilled via NG tube
(75 mg/kg/24h × 2 days; max 3.5 g)
[paralyzes worms, allows passage]
• Albendazole 200 mg once AFTER
obstruction resolves
Complete obstruction → Surgical emergency:
(or volvulus, intussusception, • Enterotomy with manual worm removal
perforation, peritonitis) • Albendazole post-op to kill remaining worms
- Harrison's 22e, p. 1859; Sleisenger & Fordtran's, p. 2267
Note on piperazine: It paralyzes worms (flaccid paralysis via GABA agonism) and is historically preferred for obstruction because paralyzed worms pass naturally without dying in situ. It is not widely available in many countries.
Biliary/Pancreatic Ascariasis
- Conservative first: IV fluids, bowel rest, antibiotics
- Albendazole is NOT effective for worms already inside the bile duct (poorly concentrated in bile; paralyzed worms in the duct cannot exit and may become trapped)
- Give albendazole only after worms have migrated back out of the duct
- Emergent ERCP with balloon/basket/forceps extraction for: acute cholangitis, obstructive jaundice, acute pancreatitis
- Avoid sphincterotomy - it facilitates future worm entry into the ducts
- Sleisenger & Fordtran's GI Disease, p. 2268
Key Points for Infants Specifically
- Intestinal obstruction is the most feared complication - the immature, narrow lumen of a 1-year-old makes this especially likely with heavy worm burdens
- Albendazole 200 mg single dose (not 400 mg) is the WHO-recommended dose for children under 24 months
- Malnutrition risk is amplified - monitor weight, albumin, vitamins A and C; supplement as needed
- Never withhold treatment - even asymptomatic ascariasis should be treated in a 1-year-old given the risk of complications
- Fever or other anthelmintic drugs (including antipyretics) can stimulate worm migration to ectopic sites - monitor closely during treatment
- Infection control: treat the household, improve sanitation; reinfection is the rule in endemic settings without environmental interventions
Summary Table
| Scenario | Management |
|---|---|
| Uncomplicated intestinal ascariasis | Albendazole 200 mg single dose (age <2 yrs) |
| Pulmonary (Loeffler) - severe | Corticosteroids; albendazole × 2 doses 1 month apart |
| Partial intestinal obstruction | NG decompression + IV fluids + antibiotics + piperazine via NG; albendazole after resolution |
| Complete obstruction / peritonitis | Emergency surgery + post-op albendazole |
| Biliary/pancreatic obstruction | Conservative; ERCP if cholangitis/pancreatitis; albendazole after worm exits duct |
| Malnutrition | Nutritional support + vitamins A/C + micronutrients |
Sources: Harrison's Principles of Internal Medicine 22e, p. 1858-1859; Goldman-Cecil Medicine, p. 3475-3476; Sleisenger & Fordtran's GI Disease, p. 2267-2268; CDC STH Guidelines; WHO Deworming Recommendations
This is a shared conversation. Sign in to Orris to start your own chat.