Epidural anaesthesia for me anaesthesia exam question
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the content needed for a comprehensive exam-focused answer. Here is the full structured revision guide on epidural anaesthesia:
Epidural Anaesthesia - Comprehensive Exam Guide
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e, Miller's Anesthesia 10e, Barash's Clinical Anesthesia 9e, Goodman & Gilman's Pharmacological Basis of Therapeutics
1. Anatomy of the Epidural Space
The epidural space surrounds the dura mater posteriorly, laterally, and anteriorly, bounded by:
- Posteriorly: ligamentum flavum and vertebral laminae
- Laterally: pedicles and intervertebral foramina
- Anteriorly: posterior longitudinal ligament and vertebral bodies
Contents: fatty connective tissue, lymphatics, Batson's venous plexus, and spinal nerve roots as they exit through the foramina.
The space extends from the foramen magnum to the sacral hiatus. It communicates with the paravertebral spaces through the intervertebral foramina - this is why connective tissue septa can occasionally cause unilateral blocks.
Key anatomical point: The epidural space is a potential space (not a true anatomical space with negative pressure at rest). Negative pressure is most reliable in the thoracic region due to tenting of the dura away from the ligamentum flavum.
2. Indications
| Category | Examples |
|---|---|
| Surgical anaesthesia | Lower abdominal, hip/lower limb, urological, gynaecological, obstetric surgery |
| Obstetric analgesia | Labour analgesia (most common use) |
| Postoperative analgesia | Major thoracic, abdominal, and vascular surgery |
| Chronic pain management | Cancer pain, chronic back pain |
| Thoracic epidural | Post-thoracotomy pain, rib fractures, pulmonary benefit |
Advantages over spinal: controllable onset, adjustable level, extendable duration via catheter, can titrate motor vs. sensory block density, segmental block possible.
3. Contraindications
Absolute:
- Patient refusal
- Infection at the injection site (local sepsis)
- True allergy to local anaesthetics
- Raised intracranial pressure (risk of brainstem herniation with dural puncture)
- Coagulopathy / uncorrected anticoagulation
Relative:
- Systemic sepsis / bacteraemia
- Spinal deformity (scoliosis, previous spinal surgery)
- Hypovolaemia / haemodynamic instability (sympathetic block exaggerates hypotension)
- Neurological disease (controversial - medicolegal concern)
- Patient inability to cooperate
- Anticoagulant therapy (requires timing as per ASRA guidelines - see below)
4. Equipment
Needles
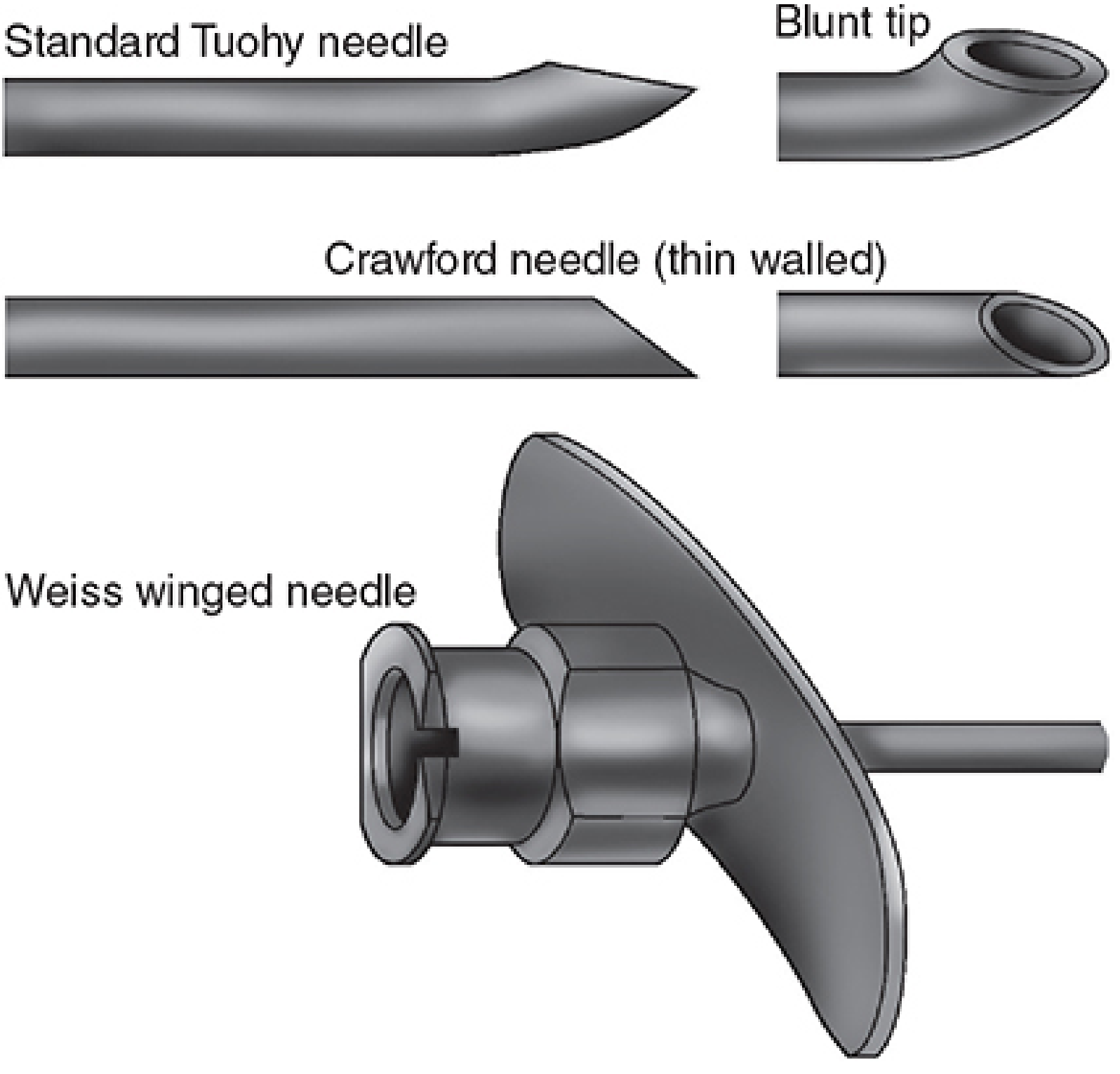
Epidural needle types - Morgan & Mikhail's Clinical Anesthesiology 7e
- Tuohy needle (most common): 17-18 gauge, 3-3.5 inches, blunt bevel with a 15-30° curve (Huber tip). The curve directs the catheter cephalad and theoretically deflects the dura rather than puncturing it.
- Crawford needle: straight, thin-walled - higher risk of dural puncture.
- Weiss winged needle: wings aid in controlled advancement.
Catheters
- 19-20 gauge catheter threaded through the 17-18 gauge needle
- Advanced 2-6 cm into the epidural space (too short = dislodgement; too long = unilateral block, vascular cannulation, knotting)
- Single-port (end-hole) or multi-port (closed tip with side holes) - side-port catheters have fewer paresthesias and lower intravascular puncture rate
5. Levels and Needle Angulation
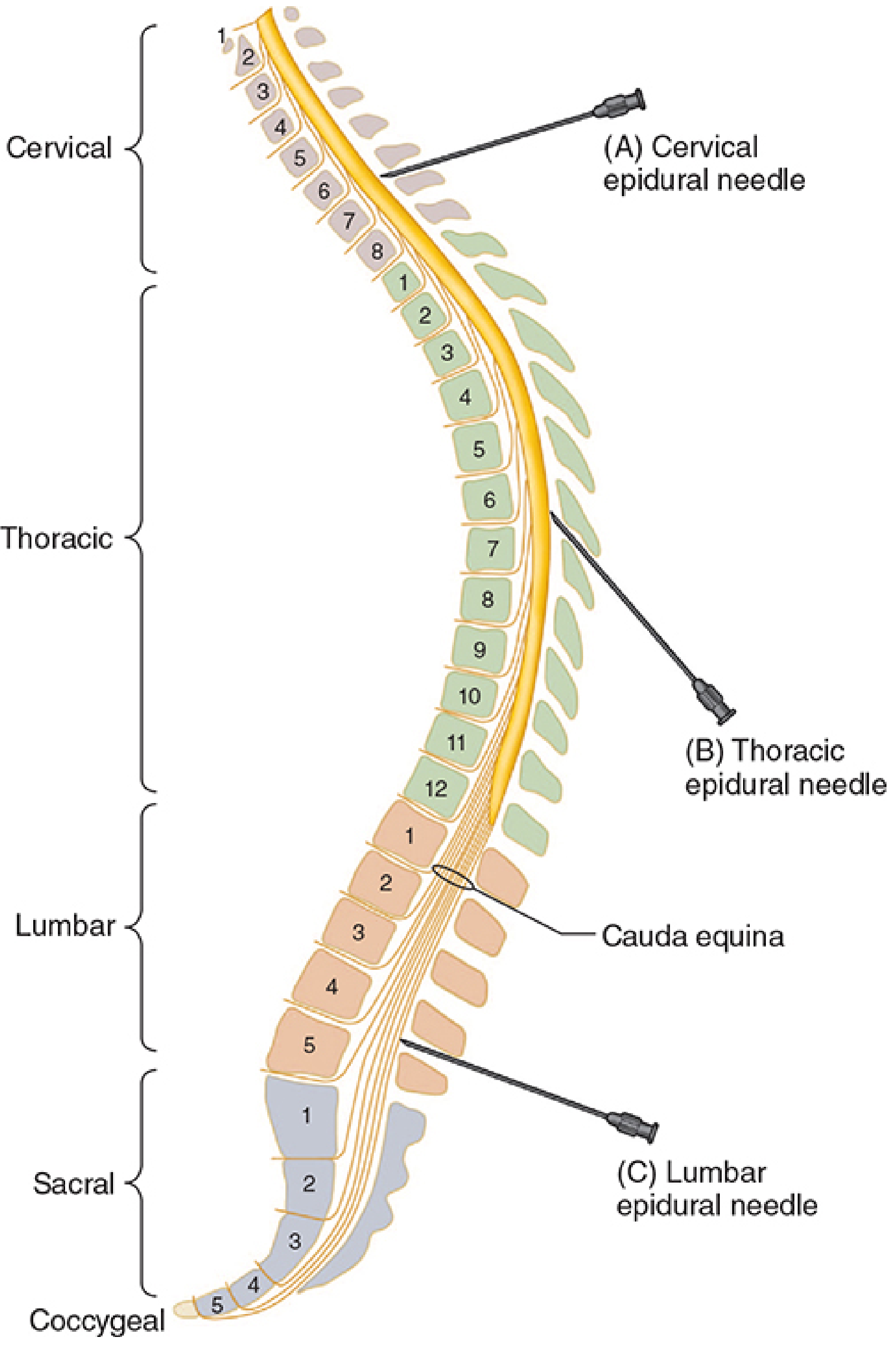
Angulation at different spinal levels - Morgan & Mikhail's Clinical Anesthesiology 7e
| Level | Angulation | Clinical Use | Notes |
|---|---|---|---|
| Lumbar | Slight cephalad (~10-15°) | Most common; surgical and obstetric | Cord ends at L1, safer below L2 |
| Thoracic | Acute cephalad (30-50°) | Post-thoracotomy, abdominal analgesia | Technically harder; spinous process overlap |
| Cervical | Minimal angulation | Chronic pain | Patient usually sitting, neck flexed |
6. Patient Positioning
- Sitting (preferred for obese patients, easier midline identification): patient arches back ("rainbow"), feet supported, assistant in front
- Lateral decubitus (preferred for hip fractures, labour, uncooperative patients): hips and knees flexed to chest to flex lumbar spine
- Lateral position is preferred for children - bending moves spinal cord forward, expanding the epidural space
7. Approaches
Midline approach: needle passes through skin → subcutaneous tissue → supraspinous ligament → interspinous ligament → ligamentum flavum → epidural space.
Paramedian (lateral) approach: needle inserted 1-2 cm lateral to midline and angled slightly medially. Used when:
- Calcified supraspinous / interspinous ligaments (elderly patients)
- Thoracic epidural (avoids acute spinous process angulation)
- Patient cannot flex adequately
8. Identifying the Epidural Space
Loss of Resistance (LOR) - Most Common
- Needle advanced to ligamentum flavum with stylet in situ
- Stylet removed, glass syringe filled with saline or air attached
- Within the ligament: resistance to injection is felt
- Advance slowly, millimetre by millimetre with continuous or intermittent pressure
- On entering epidural space: sudden loss of resistance - syringe empties freely
Air vs. saline for LOR:
- Air: simpler, easier to recognise dural puncture (instant CSF flow)
- Saline: associated with fewer complications (less risk of air emboli, pneumocephalus, incomplete blocks, pain)
- A recent meta-analysis found no statistically significant advantage of one over the other; outcomes are similar with either technique (Barash 9e, p. 2825)
Hanging Drop Technique
- Needle tip within ligamentum flavum, hub filled with saline
- Drop "hangs" at hub while in ligament
- On entering epidural space: negative pressure sucks the drop in
- More reliable for thoracic epidural (more consistent negative pressure there)
- Risk: if needle plugged, drop not drawn in → accidental dural puncture may occur
9. Activating the Epidural (Test Dose and Incremental Dosing)
Epidural volumes are large. An accidental intrathecal or intravascular injection of the full epidural dose is life-threatening.
Test Dose
Classic: 3 mL of 1.5% lidocaine + 1:200,000 epinephrine (15 mcg)
- Intrathecal injection → dense spinal block within 2-3 min (lidocaine 45 mg)
- Intravascular injection → heart rate increase ≥20% within 1 min (epinephrine 15 mcg)
Limitations of epinephrine marker:
- False positives: uterine contractions causing HR increase in laboring women
- False negatives: beta-blockade blunts HR response
- Aspiration alone is unreliable (false-negative aspirations occur with both needles and catheters)
Incremental Dosing
- Each dose is a test dose - inject in 5 mL fractions
- Large enough to produce mild symptoms (tinnitus, metallic taste) of inadvertent IV injection
- Small enough to avoid seizures or cardiovascular collapse
10. Drugs for Epidural Anaesthesia
Local Anaesthetics
| Agent | Concentration | Onset | Sensory Block | Motor Block |
|---|---|---|---|---|
| Chloroprocaine | 2-3% | Fast | Analgesic / Dense | Mild to Dense |
| Lidocaine | 1.5-2% | Intermediate | Dense | Moderate to Dense |
| Mepivacaine | 1-2% | Intermediate | Analgesic to Dense | Minimal to Dense |
| Bupivacaine | 0.0625-0.5% | Slow | Analgesic to Dense | Minimal to Moderate |
| Ropivacaine | 0.2-1.0% | Slow | Analgesic to Dense | Minimal to Moderate |
Adapted from Morgan & Mikhail's Table 45-5
Concentration determines nerve fibre type blocked (bupivacaine as example):
- 0.5%: sympathetic + sensory + motor block (surgical)
- 0.25%: sensory block without significant motor block
- 0.0625%: preganglionic sympathetic block only (labour analgesia)
Key fact - bupivacaine 0.75% is NOT approved for obstetrical use due to enhanced cardiotoxicity in pregnant patients.
Dosing rule: ~1-2 mL per segment to be blocked (e.g., 1.5% lidocaine in healthy non-pregnant adults). Volume needed decreases with: increasing age, pregnancy, and in children.
Adjuvants
| Adjuvant | Role |
|---|---|
| Epinephrine 5 mcg/mL (1:200,000) | Prolongs block duration, reduces vascular absorption, lowers peak plasma levels, helps detect IV injection |
| Opioids (fentanyl 2 mcg/mL, morphine) | Improve block quality ("density") more than duration; allow reduced LA concentration |
| Sodium bicarbonate 1 mEq/10 mL LA | Raises pH → more uncharged (active) form of LA → faster onset. Not added to bupivacaine (precipitates above pH 6.8) |
| Clonidine | Alpha-2 agonist; enhances and prolongs analgesia |
11. Factors Affecting Spread of Epidural Block
| Factor | Effect |
|---|---|
| Volume injected | Primary determinant of spread (1-1.5 mL per segment with 2% lidocaine) |
| Age | Older = decreased epidural compliance = wider spread per mL |
| Pregnancy | Engorged epidural veins reduce space → greater spread |
| Height | Taller patients need more mL per segment |
| Position / gravity | Lateral, Trendelenburg, and reverse-Trendelenburg can direct spread |
| Level of injection | Segmental spread differs by level |
12. Complications
Immediate/Technical
| Complication | Key Points |
|---|---|
| Accidental dural puncture (ADP) | Incidence ~1%; causes post-dural puncture headache (PDPH) - positional, worse upright, frontal/occipital, may have CN VI palsy |
| Intravascular injection | Epidural veins (Batson's plexus) - risk of LA systemic toxicity (LAST): CNS (tinnitus, seizures) then CVS (arrhythmias, cardiac arrest) |
| High/total spinal | From intrathecal injection of full epidural volume; causes apnoea, cardiovascular collapse |
| Subdural injection | Rare but delayed, patchy, sometimes exaggerated block |
| False loss of resistance | Soft ligaments, paraspinous muscle entry; off-centre approach |
| Unilateral block | Catheter exiting foramen or coursing laterally; fix by withdrawing 1-2 cm and reinjecting with unblocked side down |
| Sacral sparing | Large L5/S1/S2 nerve roots resist penetration; raise head of bed, reinject |
Physiological Effects / Cardiovascular
- Sympathetic blockade → vasodilation → hypotension (more predictable than spinal, develops over 10-20 min)
- Treat with IV fluids, vasopressors (phenylephrine for non-obstetric, ephedrine if bradycardia also present)
- Block of cardiac accelerator fibres (T1-T4) → bradycardia (less common than spinal)
Delayed Complications
| Complication | Details |
|---|---|
| Epidural haematoma | Risk 1 in 150,000 (estimates vary); presents with back pain + progressive neurological deficit. Surgical emergency - laminectomy within 6-8 h. Risk increases with anticoagulants. |
| Epidural abscess | Rare (<1 in 10,000); fever, back pain, neurological signs; requires drainage |
| Meningitis | Rare; usually from contamination |
| Neurological injury | Rate of neurologic complications after central neuraxial blockade <4 in 10,000; permanent injury is rare |
13. Epidural vs. Spinal - Key Exam Comparison
| Feature | Epidural | Spinal |
|---|---|---|
| Onset | Slow (10-20 min) | Fast (2-5 min) |
| Endpoint | Subjective LOR | Objective: free-flowing CSF |
| Density of block | Variable, titratable | Dense, reliable |
| Dose required | Large (toxic if wrong space) | Small |
| Motor block | Optional (dilute LA) | Usually present |
| Duration control | Catheter allows indefinite extension | Fixed by drug choice |
| Segmental block | Yes (e.g., thoracic for upper abdomen) | Limited |
| Hypotension | Gradual, more manageable | More rapid onset |
| Failure rate | Higher (10-15%) | Lower |
| Headache risk | Only if dural puncture (ADP) | Higher (especially with cutting needles) |
| Main use for labour | Yes (preferred) | Less preferred (denser block) |
14. Anticoagulation and Neuraxial Timing (ASRA Guidelines)
| Drug | Needle/catheter insertion | Catheter removal |
|---|---|---|
| Low-dose SC heparin (prophylactic) | 4-6 h after dose | 4-6 h after dose |
| IV heparin (intraoperative) | Before heparin; delay 1 h if traumatic | 4 h after last dose |
| LMWH (prophylactic, once daily) | 12 h after dose | 12 h after dose |
| LMWH (therapeutic, twice daily) | 24 h after last dose | 4 h before next dose |
| Warfarin | INR ≤1.4 | INR ≤1.4 |
| Clopidogrel | 7 days | - |
| Aspirin alone | Not a contraindication | - |
15. Benefits of Epidural Analgesia (Post-operative)
- Reduced postoperative pulmonary complications after thoracic and abdominal surgery (preserves pulmonary function, facilitates physiotherapy)
- Reduced opioid requirements → less nausea, sedation, ileus
- Better pain control at rest and on movement
- Earlier mobilisation
- May reduce risk of deep vein thrombosis
- May improve outcomes in high-risk cardiac patients undergoing major surgery
High-Yield Exam Facts
- Ligamentum flavum is the key structure - it provides the resistance before LOR
- Tuohy needle is standard; blunt curved tip to deflect dura
- Catheter advanced 2-6 cm into epidural space (not more)
- Test dose = 3 mL of 1.5% lidocaine + 15 mcg epinephrine
- Epinephrine marker: HR rise ≥20% within 60 seconds indicates IV placement
- Sodium bicarbonate speeds onset but do NOT add to bupivacaine (precipitates at pH >6.8)
- Bupivacaine 0.75% is contraindicated in obstetrics
- Epidural haematoma is a surgical emergency - laminectomy within 6-8 hours of onset
- Hanging drop is more reliable at thoracic level (more consistent negative epidural pressure)
- Unilateral block: withdraw catheter 1-2 cm, turn patient with unblocked side down, reinject
- Sacral sparing (L5/S1): raise head of bed and reinject with additional local anaesthetic
- Epidural acts primarily on spinal nerve roots (but also spinal cord and paravertebral nerves)
- Rate of serious neurological complications from central neuraxial blockade: <4 per 10,000
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e (Chapter 45), Miller's Anesthesia 10e (Chapters 74, 77), Barash's Clinical Anesthesia 9e (Chapter 35), Goodman & Gilman's Pharmacological Basis of Therapeutics (Chapter 20)
Spinal anaesthesia for MD anaesthesiology exam question
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive material. Let me compile the complete MD-level exam guide:
Spinal Anaesthesia - Comprehensive MD Anaesthesiology Exam Guide
Sources: Miller's Anesthesia 10e, Morgan & Mikhail's Clinical Anesthesiology 7e, Barash's Clinical Anesthesia 9e, Goodman & Gilman's Pharmacological Basis of Therapeutics
1. Definition and Historical Context
Spinal anaesthesia (subarachnoid block, intrathecal block) involves injection of local anaesthetic into the cerebrospinal fluid (CSF) in the lumbar intrathecal space. The first spinal anaesthetic in humans was performed by August Bier in 1898 using cocaine. Subsequent landmarks:
- Procaine: Braun 1905
- Tetracaine: Sise 1935
- Lidocaine: Gordh 1949
- Bupivacaine: Emblem 1966
Advantages: small drug dose produces rapid, profound, and reproducible analgesia with negligible plasma levels - systemic pharmacological effects are essentially absent.
2. Anatomy Relevant to Spinal Anaesthesia
Layers traversed (midline approach, superficial to deep):
Skin → subcutaneous fat → supraspinous ligament → interspinous ligament → ligamentum flavum → epidural space → dura mater → subdural space → arachnoid mater → subarachnoid space (CSF)
Key anatomical facts:
- Spinal cord terminates at L1 in adults (L3 in neonates - descends with growth)
- Thecal sac ends at S2 in adults
- Between L1 and S2 lies the cauda equina bathed in a relatively large volume of CSF - this is why lumbar puncture below L1 minimises spinal cord injury risk
- Tuffier's line (intercristal/bicristal line): connects the two iliac crests and crosses the spine at L4-L5 interspace (or L4 spinous process) in adults - used as a landmark for needle insertion
CSF characteristics:
- Volume: 120-150 mL total; approximately 25-35 mL in the lumbosacral space
- Density: 1.00059 g/mL at 37°C
- Production: ~0.35 mL/min by choroid plexus
3. Indications
| Category | Examples |
|---|---|
| Lower abdominal surgery | Caesarean section, herniorrhaphy, gynaecological operations |
| Urological | TURP, cystoscopy, prostatectomy |
| Lower limb | Hip replacement, knee arthroplasty, foot surgery, amputation |
| Anorectal / perineal | Haemorrhoidectomy, saddle block for vaginal delivery |
| Emergency | When patient has a full stomach (avoids airway manipulation) |
| Obstetric | Caesarean section - preferred over GA in most institutions |
Dermatomal level required for common procedures (Miller's Table 41.2):
| Procedure | Level Required |
|---|---|
| Upper abdominal surgery | T4 |
| Caesarean section | T4 |
| TURP / hip surgery | T10 |
| Foot and ankle surgery | L2 |
Note: visceral structures have sensory levels well above the skin incision - the peritoneum is T4, the bladder and uterus are T10.
4. Contraindications
Absolute:
- Patient refusal
- Local infection at the puncture site
- True allergy to local anaesthetics
- Raised intracranial pressure (risk of brainstem herniation)
- Coagulopathy / therapeutic anticoagulation
- Severe hypovolaemia / haemodynamic instability
Relative:
- Systemic sepsis / bacteraemia (avoid until antibiotics started and response demonstrated)
- Spinal deformity, previous spinal surgery
- Neurological disease (medicolegal concern, not absolute)
- Patient inability to cooperate
- Anticoagulant therapy (timing per ASRA guidelines)
- Severe aortic stenosis / fixed cardiac output states (cannot compensate for sympathetic block)
5. Equipment: Spinal Needles
Needle Tip Types
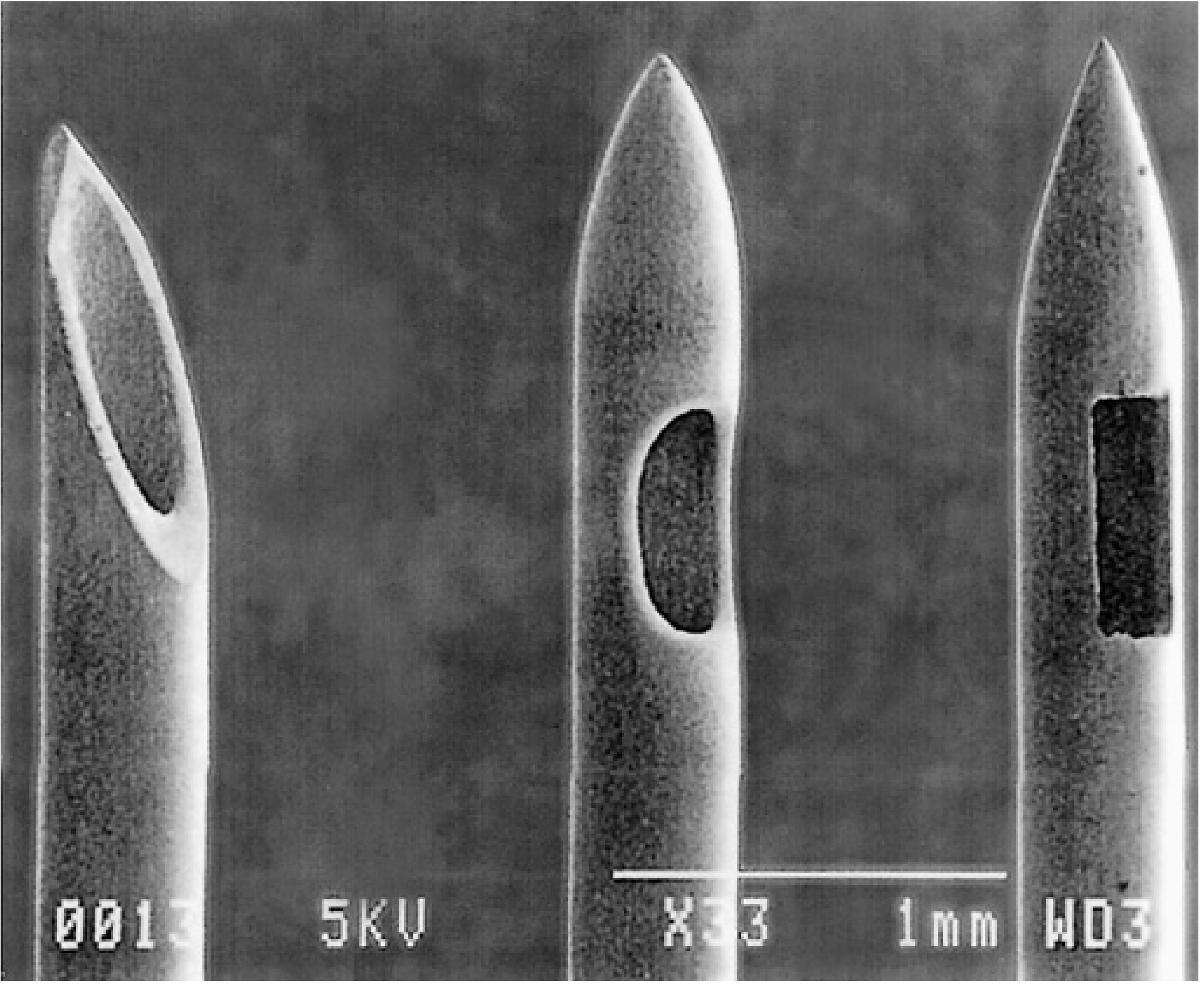
SEM of spinal needle tip designs: Quincke (cutting), Sprotte and Whitacre (pencil-point) - Miller's Anesthesia 10e
| Category | Needles | Tip Description | PDPH Risk |
|---|---|---|---|
| Cutting-tip | Quincke-Babcock, Pitkin | Bevelled cutting edge - cuts dural fibres | Higher |
| Pencil-point (atraumatic) | Whitacre, Sprotte, Pencan | Conical solid tip; side injection port | Lower |
Why pencil-point needles cause fewer PDPHs:
- The arachnoid mater cells are oriented parallel to the long axis of the spine. A parallel-bevel cutting needle slits these cells narrowly; pencil-point needles separate rather than cut. This minimises CSF leakage.
- For cutting-tip needles: orienting the bevel parallel to the long axis of the spine (i.e., parallel to the dural fibres) reduces PDPH risk by more than half.
Gauge considerations:
- Larger gauge → better tactile feel but higher PDPH rate (~40% with 22G cutting)
- Smaller gauge → lower PDPH (<2% with 29G) but higher failure rate
- Optimal balance: 25-26G pencil-point needle - lowest combined risk of PDPH and failure
Needle side-port orientation matters for pencil-point needles (not cutting needles):
- Orient cephalad to ensure adequate spread and reduce risk of local anaesthetic pooling around cauda equina
- Orienting to one side can achieve a more pronounced unilateral block
6. Patient Positioning
Sitting position:
- Easier midline identification (especially obese patients)
- Greatest lumbar flexion - maximally opens interspaces
- Preferred for saddle block (hyperbaric solution pools in sacral region while patient remains seated)
Lateral decubitus:
- Preferred for hip fractures, labour, uncooperative or haemodynamically compromised patients
- Thin patients and those with BMI <25 are more comfortable laterally
- Used for unilateral spinal (hyperbaric drug pools in dependent side)
Prone (rarely used):
- Jackknife position - described for specific perineal/sacral procedures
7. Approaches
Midline approach:
- Needle inserted in midline with slight cephalad angulation (10-15°)
- Path: skin → supraspinous ligament → interspinous ligament → ligamentum flavum → dura → arachnoid → CSF
- Characteristic "pop" or "give" as needle passes through ligamentum flavum then dura
Paramedian approach:
- Skin entry 1 cm lateral to the superior edge of the inferior spinous process
- Needle angled 10-15° off the sagittal plane, cephalomedially
- Bypasses calcified supraspinous/interspinous ligaments (elderly)
- Useful for thoracic level access
- Does not traverse supraspinous or interspinous ligaments
- If bone contacted, walk cephalad up the lamina
CSF confirmation:
- After "pop", remove stylet - CSF should appear at hub
- Small gauge → longer wait for CSF flow, especially in lateral position
- If no CSF: rotate in 90° increments; advance slightly; if still no CSF, withdraw and restart
- Confirm CSF by free flow and ability to aspirate before injecting
8. Baricity and Spread - The Core MD Concept
Baricity = density of LA solution ÷ density of CSF (at 37°C)
| Type | Baricity | CSF density comparison | Example preparation |
|---|---|---|---|
| Hyperbaric | >1.0000 | Denser than CSF | Bupivacaine + 8% dextrose |
| Isobaric | ≈1.0000 | Same as CSF | Plain bupivacaine 0.5% |
| Hypobaric | <1.0000 | Less dense than CSF | Bupivacaine + sterile water |
Clinical importance of baricity:
- Hyperbaric solutions flow to dependent (lower) regions by gravity
- Hypobaric solutions float to non-dependent (upper) regions
- Isobaric solutions are not significantly influenced by gravity
Clinical applications:
| Situation | Strategy |
|---|---|
| Saddle block (perineal surgery) | Hyperbaric solution, patient sitting → drug stays sacral |
| Unilateral spinal (e.g., hip surgery) | Hyperbaric solution, lateral decubitus, operate on the down side |
| Hip surgery requiring T10 in lateral patient | Hypobaric solution, lateral decubitus, operate on the up (non-dependent) side |
| Caesarean section (T4 needed) | Hyperbaric bupivacaine, supine - spreads to thoracic kyphosis |
Important subtlety: Plain bupivacaine 0.5% is isobaric at 24°C but slightly hypobaric at 37°C. Warming to body temperature increases spread in patients who remain seated after injection (density decreases with temperature).
The two most important determinants of spinal block height (Miller's Key Point):
- CSF volume (decreased volume → higher block)
- Baricity of the local anaesthetic solution
9. Other Factors Affecting Block Height
Drug Factors (controllable)
- Dose - primary determinant of duration and quality
- Volume × Concentration = Dose (inextricably linked)
- Baricity - most clinically important for spread control
- Temperature - warming increases hypobaricity
Patient Factors (not fully controllable)
- CSF volume: reduced by: pregnancy, obesity, increased intraabdominal pressure, Valsalva - all increase spread
- Age: decreased CSF volume and compliance with age → increased spread
- Height: taller patients need more drug to achieve same level
- Pregnancy: engorged epidural veins reduce CSF volume + thoracic kyphosis effect
Technical Factors
- Level of injection: more cephalad injection → higher block (especially with isobaric solutions)
- Speed of injection: slower injection may paradoxically increase spread; very fast injection can cause discomfort
- Barbotage (repeated CSF aspiration/reinjection): does NOT consistently affect block height
- Needle orifice orientation: affects hypobaric solutions more than hyperbaric (cephalad orientation → more cephalad spread for hypobaric)
10. Pharmacology of Intrathecal Local Anaesthetics
Classification by Duration
| Class | Agents |
|---|---|
| Short-acting | Procaine, chloroprocaine, articaine |
| Intermediate-acting | Lidocaine, prilocaine, mepivacaine |
| Long-acting | Tetracaine, bupivacaine, levobupivacaine, ropivacaine |
Key Drugs
Bupivacaine (most commonly used worldwide for spinal):
- Highly protein-bound, lipid-soluble amide
- pKa 8.1 → slow onset
- 0.5% hyperbaric (with 8% glucose): surgical anaesthesia; onset ~20 min, duration up to 225 min
- 0.5% isobaric: slightly longer duration than hyperbaric equivalent
- 0.75% not FDA-approved for obstetric neuraxial use (enhanced cardiotoxicity in pregnant patients)
- Epinephrine only slightly prolongs duration (~15 min)
Lidocaine:
- Intermediate duration (50-100 mg, ~1-1.5 hours)
- Traditionally 5% in 7.5% glucose - associated with Transient Neurological Symptoms (TNS) and cauda equina syndrome with continuous spinal technique
- Popularity has declined; still used by some practitioners
Chloroprocaine (ester):
- Ultra-short-acting; rapid metabolism by pseudocholinesterase
- 30-60 mg preservative-free preparation → reliable short-duration spinal; faster recovery than lidocaine
- TNS can still occur
- Gaining popularity for ambulatory surgery
Ropivacaine:
- Less cardiotoxic than bupivacaine; greater motor-sensory differentiation
- Potency = 0.6× that of bupivacaine
- Equivalent doses → less motor block and earlier recovery
Spinal Additives
| Additive | Dose | Effect |
|---|---|---|
| Morphine (hydrophilic) | 100-300 mcg (obstetric); up to 1000 mcg (major surgery) | 12-24 h analgesia; delayed respiratory depression risk; nausea, pruritus, urinary retention |
| Fentanyl (lipophilic) | 10-25 mcg | Rapid onset, limited spread; augments block quality; less delayed respiratory depression |
| Sufentanil (lipophilic) | 5-10 mcg | More potent than fentanyl intrathecally; similar profile |
| Epinephrine | 200-300 mcg | Prolongs bupivacaine/tetracaine duration by 30-50%; less effect on lidocaine |
| Clonidine (α2-agonist) | 15-45 mcg | Prolongs sensory and motor block; may cause hypotension and sedation |
| Neostigmine | 10-50 mcg | Analgesic via acetylcholine; limited by severe nausea/vomiting - not in widespread use |
Lipophilic vs hydrophilic opioids - key distinction:
- Lipophilic (fentanyl, sufentanil): rapid CSF uptake into neural tissue and vasculature → limited rostral spread → lower risk of delayed respiratory depression; relative intrathecal:IV potency = 10-20:1
- Hydrophilic (morphine): slow CSF uptake → wide rostral spread → risk of late respiratory depression (up to 18-24 h); relative intrathecal:IV potency = 200-300:1
11. Physiology of Spinal Block - Differential Blockade
Order of nerve fibre blockade (smallest/most myelinated blocked first):
- Preganglionic sympathetic fibres (B fibres) - smallest, blocked first
- Temperature / pain (C and Aδ fibres)
- Touch, pressure (Aβ fibres)
- Motor (Aα fibres) - largest, blocked last
Clinical consequence - block level hierarchy:
- Sympathetic block is typically 2 dermatomes HIGHER than sensory block
- Sensory block to cold is 1-2 dermatomes higher than pinprick
- Pinprick is 1-2 dermatomes higher than touch
- Motor block is 2 dermatomes LOWER than sensory block
Bromage Scale for Motor Block:
| Grade | Finding |
|---|---|
| 0 | No motor block |
| 1 | Cannot raise extended leg; can move knee and feet |
| 2 | Cannot raise extended leg or move knee; can move feet |
| 3 | Complete block - no movement |
Sensory block assessment: Cold (ethyl chloride/ice) is most sensitive (highest level); pinprick is the standard clinical test; touch gives the lowest level.
Cardiovascular Effects of Sympathetic Blockade
- Sympathetic fibres leave cord at T1-L2
- Vasodilation is predominantly venous (capacitance vessels) → reduced preload → reduced cardiac output
- Hypotension is more marked with higher block levels
- Cardiac accelerator fibres: T1-T4 - block causes bradycardia (Bezold-Jarisch reflex also contributes - venous pooling → decreased ventricular filling → paradoxical bradycardia)
- Sudden asystole can occur from loss of cardiac sympathetic + unopposed vagal activity at SA node
Treatment of spinal hypotension:
- Crystalloid/colloid preload or co-load
- Left lateral tilt in obstetric patients (aortocaval decompression)
- Phenylephrine (first-line in obstetrics - preserves uteroplacental blood flow)
- Ephedrine (when bradycardia also present - mixed α/β agonist)
- Atropine 0.6 mg for bradycardia
- Head-down tilt / leg elevation (increases venous return)
Respiratory Effects
- Low/mid lumbar block: minimal respiratory effects
- T10: intercostal muscle weakness
- High thoracic/total spinal: loss of diaphragmatic function (C3-C5) → apnoea
- Patients with high block may describe difficulty breathing due to loss of chest wall proprioception, even if diaphragm intact
Gastrointestinal Effects
- Sympathetic fibres T5-L1 inhibit peristalsis → their blockade increases gut motility
- Vagal tone becomes dominant → contracted, hyperperistaltic bowel (good surgical condition for bowel surgery)
- Nausea during spinal (especially with opioid addition or hypotension)
Urinary Effects
- Sacral (S2-S4) parasympathetic blockade → urinary retention
- Detrusor muscle paralysis - catheterisation may be required
12. Block Monitoring
After injection, assess:
- Sensory level: cold sensation (ethyl chloride) - most sensitive; pinprick - standard
- Motor block: modified Bromage scale
- Sympathetic block: HR and BP changes
- Adequate block: sensory level 2-3 segments above expected surgical stimulus + inability to straight-leg raise (ensures lumbar roots blocked)
13. Complications
Immediate
| Complication | Mechanism / Details | Management |
|---|---|---|
| Hypotension | Sympathetic vasodilation; most common complication | Fluids, vasopressors, positioning |
| Bradycardia | Block of T1-T4 cardiac accelerators + Bezold-Jarisch reflex | Atropine, ephedrine |
| Nausea/vomiting | Hypotension → cerebral ischaemia; unopposed vagal activity | Treat hypotension; antiemetics |
| High/total spinal | Excessive cephalad spread; motor block of respiratory muscles | Intubation, vasopressors, CPR if needed |
Total spinal: presents as apnoea (not hypotension alone), unconsciousness, cardiovascular collapse. Manage with airway, ventilation, circulatory support.
Risk factors for high block: obesity, short stature, pregnancy, previous failed epidural, spinal deformity.
Post-procedure
Post-Dural Puncture Headache (PDPH)
Mechanism: CSF leaks through dural tear → brain sags → traction on pain-sensitive intracranial structures AND/OR compensatory cerebral vasodilation.
Features:
- Postural - worsens upright, relieved lying flat (pathognomonic)
- Frontal or occipital distribution
- Associated: nausea, tinnitus, diplopia, CN VI palsy (longest intracranial course), hearing loss, neck stiffness
- Onset: usually 24-72 hours post-puncture; >90% begin within 3 days
- Spontaneous resolution: 72% by 7 days, 87% by 6 months
Risk factors (higher risk):
- Young age (especially 18-30 years)
- Female sex
- Low BMI
- Larger needle gauge
- Cutting needle tip
- Bevel perpendicular to spine axis
- History of PDPH or chronic headaches
Serious associations: PDPH carries substantially increased risk of cerebral venous thrombosis and subdural haematoma (aOR 19.0) and bacterial meningitis (aOR 39.7) - requires monitoring and treatment.
Treatment:
- Conservative: bed rest (relieves symptoms, does not shorten duration), adequate hydration (no strong evidence but practised), analgesics (paracetamol, NSAIDs, opioids)
- Caffeine (weak evidence - some temporary relief via vasoconstriction)
- Epidural blood patch (EBP) - definitive treatment:
- 10-20 mL autologous blood injected into epidural space at or one level below puncture site
- Clot seals dural tear; also transiently raises epidural pressure
- Success: 75-90% permanent relief with single patch
- Second patch effective for incomplete relief
- Timing: more effective if performed ≥72 hours after puncture (allow some CSF pressure to restore)
- Complication: back pain during injection (stop if severe); rarely epidural haematoma
Transient Neurological Symptoms (TNS)
- Buttock and lower extremity pain radiating symmetrically, without neurological deficit
- Onset 6-36 hours after recovery from spinal, resolves within 1-7 days
- Strongly associated with lidocaine (especially 5% hyperbaric): incidence 10-40%
- Also with: lithotomy position, ambulatory surgery, obesity, same-day procedures
- Mechanism: direct neurotoxicity of concentrated lidocaine at cauda equina
- Treatment: NSAIDs, reassurance; self-limiting
- This is why lidocaine's popularity for spinal has declined
Cauda Equina Syndrome (CES)
- Permanent neurological injury: saddle anaesthesia, bowel/bladder dysfunction, lower limb weakness
- Associated with continuous spinal anaesthesia using micro-catheters + hyperbaric 5% lidocaine (drug pooled in sacral space → neurotoxic concentrations)
- Micro-catheters for continuous spinal now largely abandoned because of this
Neurological Complications (General)
- Rate of serious neurological complications from central neuraxial blockade: <4 per 10,000
- Risk increased in elderly and those with pre-existing spinal pathology
- Epidural haematoma: rare; increased by anticoagulation; surgical emergency (laminectomy within 6-8 h)
- Meningitis: usually from contamination (Streptococcus viridans from operator's oral flora - hence face mask mandatory)
- Epidural abscess: rare; fever, back pain, neurological deterioration
Hearing Loss
- Transient low-frequency hearing loss from decreased CSF pressure affecting inner ear (endolymph-perilymph pressure differential)
- More common with large-gauge needles
- Usually resolves within ~1 month; permanent loss reported rarely
14. Combined Spinal-Epidural (CSE)
- Spinal needle passed through epidural needle (needle-through-needle technique) into CSF
- Advantages: speed + reliability of spinal + flexibility + duration of epidural catheter
- Epidural injection after spinal → increases spinal block height (volume effect compresses dural sac)
- Application: labour analgesia (spinal component for rapid onset, epidural for maintenance), prolonged surgeries, caesarean section
- Risk: epidural drugs may enter intrathecal space via dural hole → potentiated effect; always titrate carefully
15. Saddle Block
- Targeted block of sacral roots (S1-S5) only
- Patient remains seated for 5-10 min after injection of hyperbaric solution
- Drug stays in sacral (dependent) region
- Uses: anorectal surgery, perineal/perianal procedures, operative vaginal delivery
- Saddle block for vaginal delivery: hyperbaric tetracaine 3-4 mg or bupivacaine 2.5-5 mg ± fentanyl 12.5-25 mcg ± sufentanil 5-7.5 mcg
16. Unilateral and Selective Spinal Anaesthesia
- Small-dose hyperbaric solution + lateral position for 10-15 min → preferential block of dependent side
- e.g., 4-5 mg hyperbaric bupivacaine for knee arthroscopy
- Benefits: less haemodynamic instability, faster recovery, earlier discharge
- Selective spinal: minimum dose to anaesthetise only the surgical area
17. Continuous Spinal Anaesthesia
- Large-bore needle (or micro-catheter) threaded into subarachnoid space
- Allows titration of dose (useful in elderly, high-risk cardiac patients)
- Micro-catheters (≤28G) largely abandoned due to cauda equina syndrome
- Currently: 17-19G catheters via large-bore needles used (accepted high PDPH risk)
- Application: elderly patients with severe cardiac disease for major surgery
18. High-Yield MD Exam Facts Summary
- August Bier (1898) performed the first spinal anaesthetic in humans (cocaine)
- CSF density = 1.00059 g/mL at 37°C
- Spinal cord ends at L1 in adults; thecal sac ends at S2
- Tuffier's line = intercristal line = L4-L5 interspace in adults
- Two most important determinants of block height: CSF volume + baricity
- Sympathetic block is 2 segments HIGHER than sensory; motor is 2 segments LOWER
- Cardiac accelerator fibres = T1-T4; sympathetic outflow = T1-L2
- Hyperbaric → dependent regions; hypobaric → non-dependent; isobaric → gravity-independent
- Pencil-point needles (Whitacre, Sprotte) reduce PDPH vs Quincke (cutting)
- Optimal needle: 25-26G pencil-point (lowest combined PDPH + failure risk)
- Cutting needle bevel parallel to long axis of spine → reduces PDPH by >50%
- Needle side-port cephalad orientation → ensures adequate spread, prevents cauda equina pooling
- TNS: strongly associated with lidocaine (10-40%), especially in lithotomy; self-limiting 1-7 days
- Cauda equina syndrome: concentrated hyperbaric lidocaine via micro-catheter → permanent deficit
- PDPH: postural headache; onset 24-72 h; epidural blood patch 20 mL = definitive treatment; single EBP cures 75-90%
- EBP is more successful when performed ≥72 h after dural puncture
- PDPH associated with cerebral venous thrombosis (aOR 19.0) and meningitis (aOR 39.7) - serious!
- Phenylephrine is first-line vasopressor for spinal hypotension in obstetrics
- Epidural injection after spinal raises block height (CSE effect)
- Total spinal → presents as apnoea not just hypotension; treat with airway + CPR
- Morphine intrathecal: delayed respiratory depression up to 18-24 hours post-injection
- Relative intrathecal:IV potency: morphine 200-300:1; fentanyl 10-20:1
- Aseptic technique mandatory; face mask worn to prevent Streptococcus viridans meningitis
- Rate of serious neurological complications: <4 per 10,000 neuraxial blocks
Sources: Miller's Anesthesia 10e (Chapter 41), Morgan & Mikhail's Clinical Anesthesiology 7e (Chapters 45, 41), Barash's Clinical Anesthesia 9e (Chapter 35), Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.