Treatment of acute pancreatitis
Reading File
Finding Sources
Searching PubMed
"acute pancreatitis"[MeSH Terms] AND "therapy"[MeSH Terms]
Finding Sources
Searching PubMed
"acute pancreatitis" management treatment
Reading File
Reading File
Reading Article
PMID: 40651900
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have excellent, comprehensive content from Harrison's 22E (2025), Current Surgical Therapy 14e, Rosen's Emergency Medicine, Sleisenger & Fordtran, and the IAP 2025 guidelines. Let me compile the full answer.
Treatment of Acute Pancreatitis
Management algorithm from Maingot's Abdominal Operations:
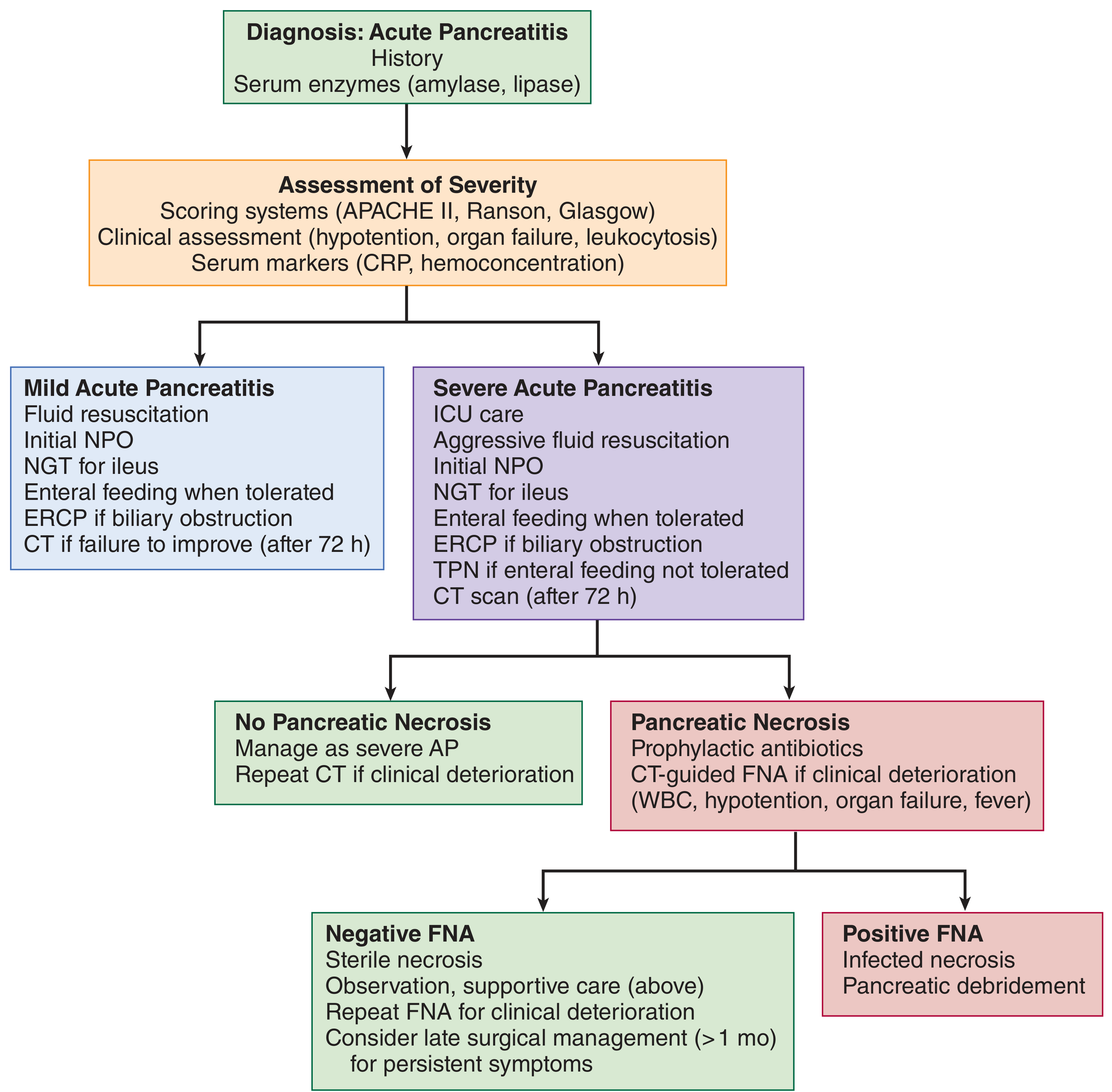
1. Initial Assessment and Severity Stratification
Before initiating treatment, severity must be determined in the emergency department to triage patients appropriately. Tools used include:
- BISAP score (most practical): BUN >25 mg/dL, impaired mental status, SIRS, age >60 years, pleural effusion. Score ≥3 predicts substantially increased in-hospital mortality.
- APACHE II ≥8 at 24 h
- Hemoconcentration (Hct >44%) and admission BUN >20 mg/dL
- Persistent SIRS at 24 h is the strongest predictor of organ failure and necrosis
- CRP >100 mg/L during hospitalization suggests severity
Triage:
- Low BISAP, no SIRS → regular ward
- Persistent SIRS or comorbidities → step-down unit
- High BISAP, non-responder to IV fluids, organ failure → ICU
(Harrison's Principles of Internal Medicine 22E, 2025)
2. Fluid Resuscitation (Cornerstone of Treatment)
Early IV fluid resuscitation is the single most important treatment intervention.
- Preferred fluid: Lactated Ringer's (LR) - shown to lower CRP levels, reduce systemic inflammation, and cause less metabolic acidosis compared to normal saline. It is more physiologic and may have anti-inflammatory properties.
- Dosing strategy: Recent RCT evidence has shifted practice toward a goal-directed rather than fixed aggressive approach:
- Bolus: 10-15 mL/kg, then 1.5-3 mL/kg/h, titrated to response
- An overly aggressive strategy (20 mL/kg bolus + 3 mL/kg/h) was associated with fluid overload without improvement in outcomes
- Target: HR normalization, MAP adequate, urine output >0.5 mL/kg/h; in severe cases, CVP 8-12 mmHg, mixed venous O2 sat ≥70%
- Monitoring response: Check hematocrit and BUN every 8-12 h. A falling BUN and Hct within the first 12-24 h confirms adequate resuscitation. A rising BUN is associated with higher in-hospital mortality.
- Avoid fluid overload: Watch for tachypnea, hypoxia, edema, pleural effusions; diurese once hypovolemia resolves.
(Harrison's 22E; Current Surgical Therapy 14e; Rosen's Emergency Medicine)
3. Analgesia
- IV opioid analgesics are the standard for pain control. There is no convincing evidence to prefer one opioid agent over another (e.g., morphine vs. hydromorphone).
- The old contraindication to morphine (sphincter of Oddi spasm) is not clinically significant.
- NSAIDs and rectal indomethacin have roles in post-ERCP pancreatitis prevention but are not the primary analgesic in management.
(Rosen's Emergency Medicine; Sleisenger & Fordtran)
4. Nutrition
A major paradigm shift has occurred - patients should not be kept NPO unnecessarily.
| Setting | Approach |
|---|---|
| Mild AP, minimal SIRS | Offer oral diet as tolerated early; advance as able |
| Severe AP, ICU admission, mechanical ventilation | Nasogastric (NG) or nasojejunal (NJ) tube + enteral nutrition (EN) within 24-36 h |
| Failure to advance oral diet after 4 days | Start EN |
| EN not tolerated | Parenteral nutrition (PN) as fallback |
Why EN over PN? Two meta-analyses showed EN provides:
- ~2-fold reduction in total and pancreatic infectious complications
- ~2.5-fold reduction in risk of death
- Lower rates of infected peripancreatic necrosis (OR 0.28), single organ failure (OR 0.25), MOF (OR 0.41) vs PN
Gastric vs. jejunal feeding: Three RCTs found no significant difference in tolerance or clinical outcome.
(Sleisenger & Fordtran's Gastrointestinal and Liver Disease)
5. Antibiotics
- Prophylactic antibiotics are NOT recommended - sterile necrosis does not benefit, and prophylaxis selects for resistant organisms.
- Do not use probiotics - a multicenter RCT showed mortality more than doubled in the probiotic group, possibly from intestinal ischemia.
- When to use antibiotics:
- Documented infected pancreatic necrosis (radiographic or positive fluid culture)
- Clinical sepsis with a clear infectious source
- Cholangitis
- Antibiotic choice for infected necrosis: Carbapenems (imipenem, meropenem) penetrate pancreatic necrosis better than cephalosporins or fluoroquinolones.
- Goal of antibiotics in infected necrosis: Stabilize the patient and defer intervention until at least 4 weeks after onset to allow collection to mature and wall off.
(Current Surgical Therapy 14e; Rosen's Emergency Medicine)
6. Etiology-Directed Treatment
Gallstone Pancreatitis
- Abdominal ultrasound should be performed in all patients to assess for biliary etiology.
- ERCP is indicated only if there is: ascending cholangitis OR biliary obstruction (not for uncomplicated gallstone pancreatitis alone).
- ERCP should be performed within 24-48 h if cholangitis is present.
- Cholecystectomy during the same admission is recommended for mild AP to prevent recurrence. Endoscopic biliary sphincterotomy is an alternative for poor surgical candidates.
Hypertriglyceridemia (TG >1000 mg/dL)
- Insulin infusion (drives triglyceride uptake into cells), fibrates, and plasmapheresis in severe cases.
- Long-term: fibrate therapy, dietary fat restriction.
Hypercalcemia
- Treat the underlying cause (hyperparathyroidism, malignancy).
Drug-induced
- Discontinue the causative agent.
(Harrison's 22E 2025)
7. Management of Necrotizing Pancreatitis and Complications
Sterile Necrosis
- Conservative management. No surgical intervention unless symptomatic sterile necrosis persists >8 weeks (e.g., gastric outlet obstruction, pain, disconnected pancreatic duct).
- CT-guided FNA can confirm sterility if clinical deterioration occurs.
Infected Necrosis - The "Step-Up Approach"
The modern standard replaces emergent open necrosectomy (which carried 50% mortality):
- Antibiotics to stabilize + defer
- Minimally invasive drainage first: endoscopic or percutaneous drainage (wait at least 4 weeks for the collection to "wall off" - walled-off necrosis is more amenable to drainage)
- Step up to endoscopic necrosectomy or surgical (video-assisted retroperitoneal debridement/VARD) only if drainage alone fails
Why wait 4 weeks? Surgical intervention carries:
- 75% mortality in first 2 weeks
- 45% mortality at 2-4 weeks
- 8% mortality if delayed beyond 30 days
Recent data favor endoscopic drainage over percutaneous as primary approach due to higher success rates. Combination (both percutaneous + endoscopic) may reduce pancreatic fistula and avoid surgical necrosectomy.
Emergent indications (regardless of timing):
- Intestinal ischemia
- Perforated viscus
- Acute uncontrolled hemorrhage
- Abdominal compartment syndrome
(Current Surgical Therapy 14e; Maingot's Abdominal Operations)
8. Monitoring and Discharge
- Serial vitals, urine output every 6-8 h
- Hematocrit + BUN every 8-12 h
- Lipase/amylase need not be serially tracked (levels don't correlate with severity)
- CT scan: not routinely indicated at presentation; use if diagnosis uncertain, failure to improve by 72 h, or to assess for complications
- Patients with mild AP can be discharged when pain is controlled and oral intake is tolerated
Recent Guideline Update (2025)
The IAP/APA/EPC Revised Guidelines 2025 (endorsed by American Pancreatic Association, European Pancreatic Club, Indian Pancreas Club, and Japan Pancreas Society) represent the most current international guidance, covering 96 questions across 18 domains including pain control, fluid therapy, nutritional support, interventional treatment for infected necrosis, complication management, and prevention of recurrence. Special attention is given to AP in pregnancy, trauma, and metabolic causes.
Summary of the key principles:
- Fluid resuscitation with LR - goal-directed, not reflexively aggressive
- Oral or enteral nutrition early - NPO only when truly needed
- No prophylactic antibiotics
- ERCP only for cholangitis/obstruction, not routine
- Delayed (>4 weeks), step-up, minimally invasive approach to necrotizing pancreatitis
This is a shared conversation. Sign in to Orris to start your own chat.