Patient with left anterior limb of internal capsule infarct with change in the behaviour, cognition. 2.5x1.5 cm how can we make his cognition better
Reading File
Finding Sources
Finding Sources
Searching PubMed
"internal capsule" AND "cognitive impairment" AND stroke
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
"post-stroke cognitive impairment" AND treatment
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
"vascular cognitive impairment" AND "cognitive rehabilitation"
Finding Sources
Finding Sources
Reading Article
PMID: 37004840
Reading Article
PMID: 41198594
Reading File
Reading File
Finding Sources
I now have comprehensive data to synthesize a detailed, clinically actionable answer. Let me compose it.
Left Anterior Limb of Internal Capsule (ALIC) Infarct — Cognitive & Behavioural Sequelae and Management
Why this infarct causes cognition/behaviour changes
The anterior limb of the internal capsule (ALIC) is anatomically ~2 cm long, separating the caudate head from the lenticular nucleus. It carries:
- Frontopontine fibres
- Thalamocortical and corticothalamic fibres (bidirectional frontal lobe ↔ thalamus connections, including DLPFC–thalamic loops)
- Caudate–putaminal fibres
Blood supply: Recurrent artery of Heubner (ACA branch) ± superior lenticulostriate branches of the MCA.
A 2.5 × 1.5 cm lesion here is large enough to constitute a "strategic infarct" — disrupting frontal–subcortical circuits that subserve executive function, working memory, motivation, processing speed, and behavioural regulation. Kaplan & Sadock's Comprehensive Textbook explicitly notes that "thalamic and internal capsule strokes may produce cognitive impairment by interfering with frontal networks." - Kaplan & Sadock's Comprehensive Textbook of Psychiatry
Expect: abulia, apathy, executive dysfunction, slowed processing, memory-encoding difficulties, and behavioural disinhibition — rather than the amnestic profile of hippocampal disease.
Management Framework
1. Vascular Risk Factor Control (First Priority)
This is the single most evidence-based intervention for preventing further cognitive decline after a vascular event.
| Target | Goal |
|---|---|
| Blood pressure | <130/80 mmHg (AHA Life's Essential 8 guidelines; SPRINT-MIND data showed SBP <120 mmHg reduced MCI incidence HR 0.81) |
| Glycaemia | HbA1c optimisation |
| Lipids | Statin therapy (secondary stroke prevention) |
| Antiplatelet | Aspirin ± clopidogrel per stroke aetiology |
| Atrial fibrillation | Screen; anticoagulate if present |
| Lifestyle | Physical exercise, Mediterranean diet, smoking cessation, sleep hygiene |
Harrison's 22E states: "At a minimum, treatment should assiduously follow primary stroke prevention guidelines … managing blood pressure, controlling cholesterol, reducing blood sugar, maintaining an active lifestyle, adhering to a heart-healthy diet, losing weight, discontinuing tobacco, and getting healthy sleep." - Harrison's Principles of Internal Medicine 22E
2. Cognitive/Behavioural Rehabilitation
A. Structured Cognitive Training
- Targeted neuropsychological rehabilitation focusing on executive function, attention, and working memory (matching the ALIC frontal-network deficits)
- Computer-assisted cognitive retraining programmes
- Bradley & Daroff's notes VR-based cognitive rehab shows encouraging early results for post-stroke patients - Bradley and Daroff's Neurology in Clinical Practice
B. Repetitive Transcranial Magnetic Stimulation (rTMS)
A 2023 systematic review and meta-analysis (PMID 37004840) of 8 RCTs in post-stroke cognitive impairment found:
- rTMS + cognitive training → large effect on global cognition (Hedges' g = 0.780)
- Large effect on executive function (g = 0.769) — exactly the domain disrupted by ALIC infarcts
- Medium improvement in working memory (g = 0.609)
- Medium improvement in ADL (g = 0.418)
- Typical targets: DLPFC; 10 Hz excitatory stimulation on the affected hemisphere
- No benefit on episodic memory or attention alone
C. Physical Exercise
A 2025 systematic review on VCI therapeutic strategies (PMID 41198594, Masserini et al., Alzheimer's & Dementia) of 173 trials found physical exercise showed small-to-moderate improvements in cognition alongside cognitive rehabilitation.
3. Pharmacological Treatment
No drug is currently licensed specifically for vascular cognitive impairment, but off-label use with shared decision-making is reasonable:
| Drug | Evidence | Dose |
|---|---|---|
| Donepezil | Modest cognitive benefit in VaD RCTs; Cochrane meta-analysis: moderate-to-high certainty for slight benefit | 5 mg → 10 mg/day |
| Galantamine | Similar modest benefit | 16–24 mg/day |
| Memantine | Improvements in cognition and global status in VCI; useful in moderate–severe impairment | 20 mg/day |
| Rivastigmine | Less certain evidence; further study needed | 6–12 mg/day or patch |
Maudsley Prescribing Guidelines (15th ed.) states: "Memantine was found to provide significant efficacy in global status. They were all safe and well tolerated … The effect is modest, but in the absence of any other treatments, these agents may be considered in people living with vascular cognitive impairments." - The Maudsley® Prescribing Guidelines in Psychiatry, 15ed
Key caveat: These drugs show effects comparable to Alzheimer's disease but of uncertain clinical significance — discuss realistic expectations with patient/family.
For Behavioural Symptoms (apathy, disinhibition):
- Apathy: Methylphenidate (off-label) has the best evidence for post-stroke apathy; small trials support modest benefit. SSRIs (sertraline, citalopram) for comorbid depression–apathy overlap.
- Agitation/disinhibition: SSRIs first-line; avoid antipsychotics unless necessary (increased stroke risk).
4. Emerging / Adjunctive Therapies
| Intervention | Evidence |
|---|---|
| Ginkgo biloba extract (EGb761) | 2025 meta-analysis (PMID 41198594): largest effect size among tested drugs (Cohen's d 0.83 for cognition); evidence certainty low |
| Cerebrolysin | Small-to-moderate improvement in cognition in VCI meta-analysis |
| Intermittent Theta Burst Stimulation (iTBS) | 2024 meta-analysis (PMID 38651344) shows benefit for cognitive dysfunction |
| Music therapy | 2024 RCT (PMID 39098085): personalised music listening improved post-stroke cognition |
| Occupational therapy | Goal-directed ADL training to compensate for executive dysfunction |
5. Neuropsychiatric Monitoring
This patient needs serial cognitive assessment with tools sensitive to frontal–executive domains:
- MoCA (Montreal Cognitive Assessment) — sensitive to executive/attention deficits
- FAB (Frontal Assessment Battery) — directly targets this lesion's network
- Trail Making Test B, CLOX, FAS verbal fluency — executive battery
- Depression screening (PHQ-9) — depression accelerates cognitive decline post-stroke
Summary of Priorities
1. Aggressive vascular risk factor control (BP <130/80, statin, antiplatelet)
2. Multidisciplinary cognitive rehabilitation (neuropsychologist + OT)
3. rTMS + cognitive training (strongest evidence for executive function)
4. Consider donepezil 10 mg or memantine (modest but reasonable in absence of alternatives)
5. Treat comorbid depression/apathy (SSRI ± methylphenidate for apathy)
6. Serial MoCA + FAB to monitor trajectory
7. Physical exercise programme
Recent Evidence Update: The 2025 Masserini et al. meta-analysis (Alzheimer's & Dementia, PMID 41198594) is the most comprehensive review of VCI therapeutics to date (173 trials, 22,347 participants). It confirms modest benefits for AChEIs, memantine, cerebrolysin, physical exercise, and cognitive rehabilitation — but highlights the need for subtype-specific trials. Ginkgo biloba showed the largest effect size but with low certainty evidence.
How early bp should be controlled?
Finding Sources
Finding Sources
Searching PubMed
"blood pressure" AND "acute ischemic stroke" AND management
Reading File
Reading File
Reading File
Comprehensive data. Here is the full, phase-by-phase answer:
Blood Pressure Control Timing After Ischemic Stroke — Complete Framework
The Core Principle: Early Aggressive Lowering is Harmful
BP typically rises acutely after stroke (Cushing response, pain, anxiety, pre-existing hypertension) and falls spontaneously over 2–4 days without any treatment. Aggressive early lowering reduces perfusion to the ischaemic penumbra, which is pressure-dependent, and is associated with neurological deterioration. - Adams and Victor's Principles of Neurology, 12th Edition
Phase 1: Acute Phase (First 24 Hours)
This is the most critical and counterintuitive phase — permissive hypertension is the rule.
If the patient did NOT receive thrombolysis (tPA) or thrombectomy:
| BP Threshold | Action |
|---|---|
| SBP < 220 mmHg AND DBP < 120 mmHg | Do NOT lower — withhold antihypertensives |
| SBP ≥ 220 mmHg OR DBP ≥ 120 mmHg | Lower cautiously — maximum 15% reduction in first 24 hours |
Washington Manual: "BP should not be lowered acutely unless necessary for acute coronary syndrome, CHF, hypertensive crisis with end-organ involvement, or SBP >220 or DBP >120 mmHg. BP lowering should proceed cautiously, with 15% during the first 24 hours being a reasonable goal." - The Washington Manual of Medical Therapeutics
If patient received IV tPA (thrombolysis):
| Before tPA | During/after tPA (first 24 h) |
|---|---|
| Lower BP to < 185/110 mmHg before giving tPA | Maintain BP < 180/105 mmHg for at least 24 hours post-infusion |
AHA/ASA and ESO guidelines per Comprehensive Clinical Nephrology, 7th Edition: pre-thrombolysis target <185/110, post-thrombolysis maintenance <180/105 for 24 hours.
If patient received mechanical thrombectomy:
Recent 2024 meta-analyses (PMID 38386320, JAMA Network Open) show intensive BP control post-thrombectomy (target SBP <140 mmHg) may increase risk of poor outcome — conventional targets (~<180 mmHg) are generally safer unless reperfusion is confirmed on imaging.
Phase 2: 24–72 Hours (Stabilisation Phase)
- Resume or initiate antihypertensives only when neurological status has stabilised
- Avoid if patient is still deteriorating or fluctuating
- If pre-stroke antihypertensives were being taken, restart at reduced dose (to avoid precipitous drop, especially in non-compliant patients)
Adams and Victor's: "The treatment of previously unappreciated hypertension is preferably deferred until the neurologic deficit has stabilised. It may be prudent to avoid antihypertensive drugs in the first few days unless there is active myocardial ischaemia or the BP is high enough to pose a risk to other organs." - Adams and Victor's Principles of Neurology, 12th Edition
Phase 3: After 72 Hours / Sub-acute Phase
- Initiate or optimise long-term antihypertensive therapy
- This is when BP control demonstrably reduces recurrent stroke risk and cognitive decline
- Gradual titration is preferred — avoid sudden drops
Phase 4: Long-term (Secondary Prevention)
| Population | Target BP |
|---|---|
| General stroke survivors | < 140/90 mmHg |
| High cardiovascular risk (10-year CVD risk ≥10%) | < 130/80 mmHg |
| Very elderly / frail | Individualise — avoid over-treatment |
Preferred agents for secondary stroke prevention:
- ACE inhibitors or ARBs (e.g., perindopril, ramipril, telmisartan) — PROGRESS trial
- Thiazide diuretics (e.g., indapamide) — often combined with ACEi
- Avoid beta-blockers as first-line unless cardiac indication (less effective for stroke prevention)
SPRINT-MIND data: SBP target <120 mmHg reduced incident MCI (HR 0.81) and combined MCI/dementia (HR 0.85) — relevant to your patient with cognitive impairment. - Harrison's Principles of Internal Medicine 22E
Summary Table
| Time Point | Action |
|---|---|
| 0–24 h (no tPA) | Permissive hypertension; treat only if SBP ≥220 or DBP ≥120; max 15% reduction |
| 0–24 h (with tPA) | Pre-tPA: <185/110; Post-tPA: maintain <180/105 |
| 24–72 h | Restart prior meds at reduced dose once stable; no aggressive lowering |
| >72 h | Gradual optimisation; target <140/90 |
| Long-term | <130/80 for high CVD risk; ACEi/ARB + thiazide preferred |
Bottom line for your ALIC infarct patient: Since this is a lacunar/small vessel infarct (2.5×1.5 cm in the internal capsule territory), BP is both the cause and the ongoing threat. In the first 24 hours, tolerate elevated BP. From day 2–3 once stable, begin gentle antihypertensive therapy, titrating to a long-term target of <130/80 mmHg given the cognitive impairment — this is both stroke prevention and dementia prevention.
Other than cv Doppler and 2d echo any specific evaluation required?
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"ischemic stroke" AND "etiological evaluation" AND "small vessel"
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
All the data needed is now in hand. Here is the comprehensive answer:
Specific Evaluation Required for Left ALIC Infarct (Beyond Carotid Doppler & 2D Echo)
The ALIC is supplied by the recurrent artery of Heubner (ACA branch) and superior lenticulostriate arteries (MCA branch). This is typically a small-vessel / lacunar infarct, but embolic and other causes must be excluded systematically. The workup is organised by category:
1. Neuroimaging
| Investigation | Purpose |
|---|---|
| MRI Brain (DWI + ADC + FLAIR + GRE/SWI) | Confirm infarct acuity, exclude haemorrhage, detect additional silent infarcts/white matter disease suggesting small vessel disease |
| MR Angiography (MRA) or CTA of head & neck | Images entire arterial tree in one study — intracranial stenosis, ACA/MCA disease, carotid bifurcation; replaces need for conventional angiography in most cases |
| Transcranial Doppler (TCD) | Detect intracranial stenosis, microemboli signals (HITS — high-intensity transient signals), right-to-left shunt (bubble study for PFO) |
| CT Perfusion / MR Perfusion | If penumbra assessment needed in acute setting |
Harrison's 22E: "Because MRA images the entire arterial system relevant to stroke, with the exception of the heart, much of the clinician's stroke workup can be completed with this single imaging study." - Harrison's Principles of Internal Medicine 22E
2. Cardiac Monitoring (Arrhythmia Detection)
This is critical even for small-vessel infarcts — the STROKE-AF trial showed paroxysmal AF is detected in a significant proportion of strokes attributed to small/large vessel disease.
| Investigation | Duration & Indication |
|---|---|
| 12-lead ECG | Immediate — detect AF, LVH, ischaemia |
| Inpatient telemetry | Minimum 24–48 hours; detects AF in ~5% |
| Ambulatory Holter / event monitor (30-day) | If telemetry negative; detects occult AF in up to 25% of cryptogenic strokes |
| Implantable loop recorder (ILR) | If 30-day monitoring negative and high clinical suspicion; can monitor for 1–3 years |
"The use of extended cardiac rhythm monitoring (30-day event-triggered loop monitoring or an implanted monitor) reveals occult atrial fibrillation in up to 25% of patients with an otherwise cryptogenic stroke." - Goldman-Cecil Medicine
3. Cardiac Structural Evaluation (Beyond TTE/2D Echo)
| Investigation | When to Use |
|---|---|
| Transesophageal Echo (TEE) | Superior to TTE for: PFO detection, left atrial appendage thrombus, aortic arch atheroma, bacterial endocarditis, atrial septal aneurysm — consider if TTE inconclusive or embolic source suspected |
| Bubble contrast echo (agitated saline) | Via TTE or TEE — for PFO/right-to-left shunt detection, especially in younger patients |
| Cardiac MRI | If cardiomyopathy, LV thrombus, or cardiac tumour suspected |
| Cardiac enzymes (Troponin, BNP) | Acute MI as precipitant; Troponin elevation is common post-stroke |
4. Haematological & Laboratory Workup
| Test | Rationale |
|---|---|
| CBC + differential | Polycythaemia, thrombocytosis, leukaemia, anaemia (sickling) |
| PT, aPTT, INR | Baseline coagulation; guided thrombophilia interpretation |
| Fasting lipids (LDL, HDL, TG) | Atherosclerotic risk |
| HbA1c + fasting glucose | Diabetes — a major ALIC small vessel disease risk factor |
| Renal function (eGFR, creatinine) | Renovascular hypertension; AKI from contrast |
| ESR, CRP | Vasculitis, inflammatory cause |
| Homocysteine | Elevated in 25–30% of young stroke; independent risk factor |
| Syphilis serology (VDRL/RPR) | Luetic vasculitis |
| HbA1c | If not already done |
5. Thrombophilia Screen (Selective — especially if young, no obvious risk factors, or recurrent strokes)
Per Bradley & Daroff's Box 65.7: - Bradley and Daroff's Neurology in Clinical Practice
- Antiphospholipid antibodies: Anticardiolipin IgG/IgM, β2-glycoprotein-1 IgG/IgM, Lupus anticoagulant
- Protein C activity
- Protein S (total and free antigen)
- Antithrombin III activity
- Factor V Leiden mutation
- Prothrombin G20210A mutation
- Plasma homocysteine
- Fibrinogen
- Haemoglobin electrophoresis (if sickle cell suspected)
Note: Thrombophilia testing should be done off anticoagulation and ideally in a non-acute setting (acute-phase proteins alter results).
6. Vasculitis / Autoimmune Screen (if clinically suggested)
- ANA, ANCA, anti-dsDNA
- Complement C3/C4
- CSF examination — if CNS vasculitis or infectious aetiology suspected
7. Specialised Investigations (if still cryptogenic after standard workup)
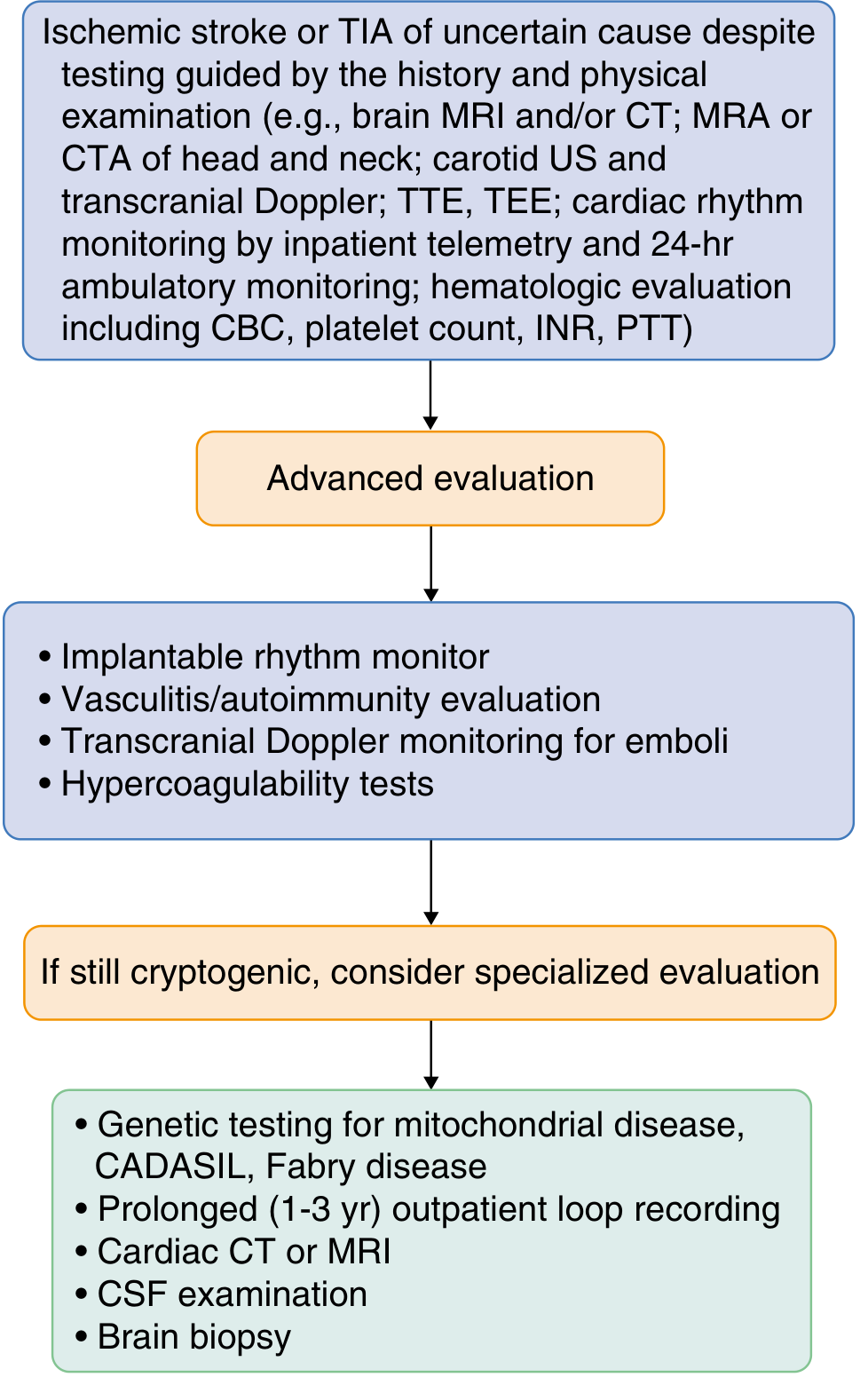
- Genetic testing: CADASIL (NOTCH3), Fabry disease (α-galactosidase A), MELAS (mitochondrial) — consider in young patients with white matter disease or family history
- Prolonged outpatient loop recording (1–3 years) for paroxysmal AF detection
- Aortic arch imaging (TEE or CTA) — significant source of artery-to-artery emboli
- Brain biopsy — only if CNS vasculitis or unusual pathology suspected
For Your Specific Patient (Left ALIC Infarct, 2.5×1.5 cm)
Given the location (small vessel territory, recurrent artery of Heubner / lenticulostriates), the most likely mechanism is hypertensive small vessel disease. However, the priority workup should include:
| Priority | Investigation |
|---|---|
| Essential | MRI brain + MRA head & neck, 12-lead ECG + 24–48h telemetry, HbA1c, fasting lipids, homocysteine, CBC, renal function |
| Important | TEE if TTE non-diagnostic or embolic features; TCD with bubble for PFO |
| If no cause found | 30-day Holter, antiphospholipid screen, thrombophilia panel |
| If young / atypical | CADASIL/Fabry genetics, vasculitis screen, CSF |
This is a shared conversation. Sign in to Orris to start your own chat.