Laminar airflow in orthopedics 10 mark pg answer with flow chart and images
Reading File
Finding Sources
Finding Sources
Searching the Web
laminar airflow orthopedic surgery clean room infection prevention 10 marks
Reading File
Finding Sources
Reading Web Page
https://openorthopaedicsjournal.com/VOLUME/9/PAGE/495/FULLTE…
Reading File
Finding Sources
Searching PubMed
"laminar airflow" AND "orthopedic" AND "surgical site infection"
Reading File
Searching PubMed
"laminar airflow" AND "arthroplasty" AND "infection"
Reading File
Reading Web Page
https://orthopedicreviews.openmedicalpublishing.org/article/…
Loading Image
Searching the Web
laminar airflow operating room vertical horizontal diagram orthopedic site:ncbi.nlm.nih.gov OR site:pubmed.ncbi.nlm.nih.gov
Loading Image
Loading Image
I now have all the information needed to write a comprehensive 10-mark answer. Let me compose it.
Laminar Airflow in Orthopaedics
Definition
Laminar airflow (LAF) refers to a ventilation system in which a body of air within the operating theatre moves with uniform velocity in a single direction along parallel flow lines, without turbulence or mixing. True laminar flow is achieved when approximately 100% HEPA (High-Efficiency Particulate Air) filter coverage is in place, producing ultraclean air (UCA) containing less than 10 colony-forming units per cubic metre (CFU/m³) of bacteria.
Historical Background
LAF was pioneered in orthopaedic surgery by Sir John Charnley in the 1960s-1970s for total hip arthroplasty. He combined laminar flow with body-exhaust suits, achieving a dramatic reduction in deep infection rates (from ~9% to <1%). Lidwell et al. subsequently confirmed in large RCTs that ultraclean air environments, combined with body-exhaust suits and prophylactic antibiotics, significantly reduced sepsis rates in joint arthroplasty. This led to widespread global adoption in orthopaedic operating theatres.
Why Air Contamination Matters in Orthopaedics
The operating room air carries:
- Skin squames (shed from personnel)
- Respiratory droplets
- Dust particles acting as bacterial carriers (particles ≥5 µm)
Staff movement and door opening increase microbial load. In prosthetic joint surgery, even a small inoculum of bacteria (e.g., Staphylococcus epidermidis, S. aureus) can cause catastrophic periprosthetic joint infection (PJI), which is one of the most devastating complications of total joint arthroplasty (TJA).
Components of a LAF System
| Component | Function |
|---|---|
| Fan/blower unit | Draws room air in and forces it through the filter |
| Pre-filter | Removes large particles (lint, dust) |
| HEPA filter | Removes particles ≥0.3 µm with 99.97-99.995% efficiency |
| Plenum chamber | Distributes air evenly across the filter face |
| Exhaust/return vents | Low-level exhaust removes contaminated air from the periphery |
| Positive pressure system | Maintains positive pressure relative to adjacent rooms to prevent ingress of contaminants |
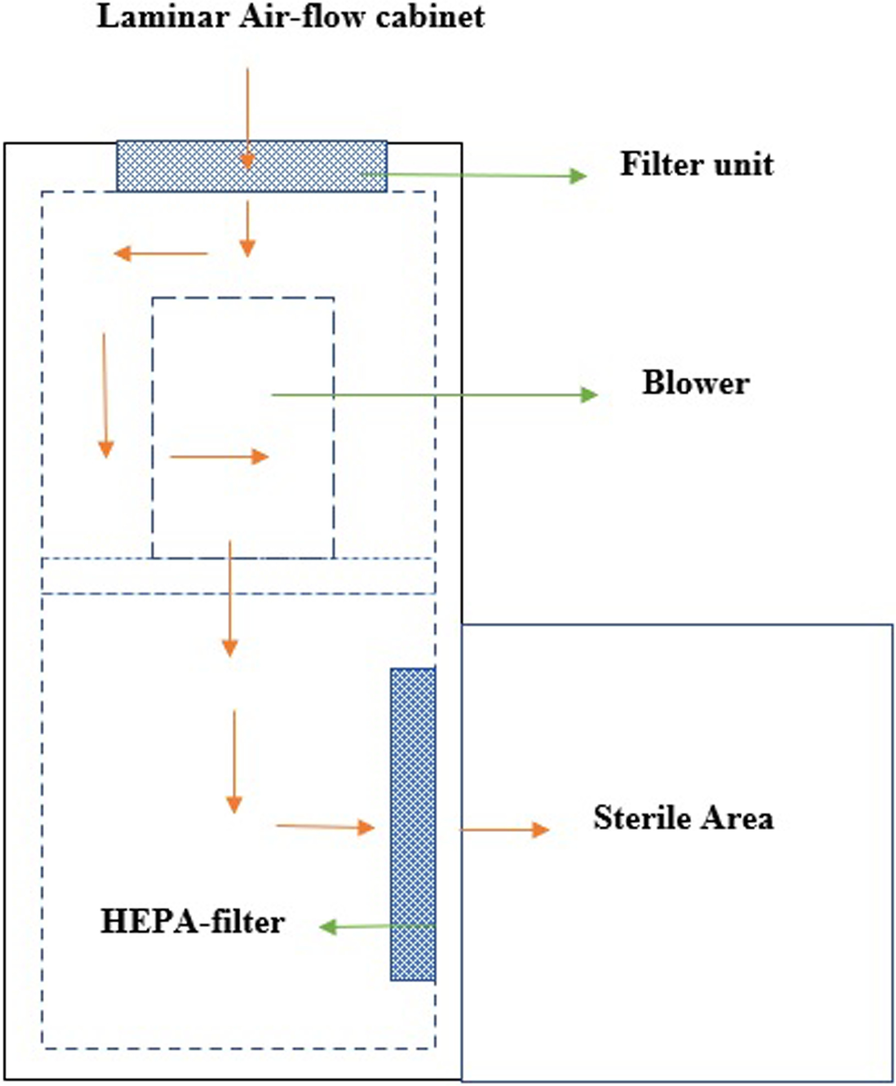
LAF cabinet diagram:
Types of Laminar Airflow
1. Vertical Laminar Flow (Downflow / Ceiling-Mounted)
- Air flows downward from a ceiling-mounted HEPA filter array over the surgical field
- The clean air "washes" the operative site from above
- Return vents are at floor level on the sides
- Preferred type for orthopaedic surgery - surgeons are positioned within the clean air stream and do not stand between the air supply and the wound
- Coverage typically 2.7 m × 2.7 m to 3.6 m × 3.6 m
2. Horizontal Laminar Flow (Cross-flow / Wall-Mounted)
- Air flows horizontally across the room from one wall to the opposite wall
- Disadvantage in orthopaedics: Surgical team members may stand between the air source and the operative field, causing turbulence and actually increasing wound contamination
- Campbell's 15th ed. notes that horizontal flow has been shown to increase postoperative infection rates in TKA for this reason
3. Conventional/Turbulent Ventilation (non-LAF)
- Air introduced at ceiling in turbulent mixing pattern
- Achieves 300-400 CFU/m³ typically
- Not considered ultraclean
Airborne Bacterial Count Standards
| System | Bacterial Count |
|---|---|
| Conventional ventilation | 180-900 CFU/m³ |
| HEPA filtered turbulent | ~35 CFU/m³ |
| Laminar flow (ultraclean) | <10 CFU/m³ |
| Laminar flow + body exhaust suit | <1 CFU/m³ |
FLOWCHART: Laminar Airflow - Mechanism and Workflow
┌─────────────────────────────────────────────────────────┐
│ CONTAMINATED OPERATING ROOM AIR │
│ (skin squames, respiratory droplets, dust) │
└──────────────────────────┬──────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────┐
│ BLOWER / FAN UNIT │
│ (forces air through the filter system) │
└──────────────────────────┬──────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────┐
│ PRE-FILTER │
│ (removes large particles >5 µm) │
└──────────────────────────┬──────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────┐
│ HEPA FILTER │
│ (removes 99.97-99.995% of particles ≥0.3 µm) │
│ Bacterial count → <10 CFU/m³ │
└──────────────────────────┬──────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────┐
│ ULTRACLEAN AIR DELIVERED TO FIELD │
│ │
│ VERTICAL FLOW HORIZONTAL FLOW │
│ (ceiling → floor) (wall → wall) │
│ [PREFERRED ✓] [RISK of turbulence ✗] │
└──────────────────────────┬──────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────┐
│ SURGICAL FIELD (Sterile Zone) │
│ - Clean air sweeps over the wound and implants │
│ - Contaminated air pushed peripherally │
└──────────────────────────┬──────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────┐
│ LOW-LEVEL EXHAUST / RETURN VENTS │
│ (contaminated air removed from room perimeter) │
└─────────────────────────────────────────────────────────┘
│
▼
[AIR RECIRCULATED back to blower]
FLOWCHART: LAF in Reducing Periprosthetic Joint Infection (PJI)
TOTAL JOINT ARTHROPLASTY (THA / TKA)
│
┌───────┴────────┐
│ │
WITHOUT LAF WITH LAF
(turbulent) (ultraclean air)
│ │
Air: ~180-900 Air: <10
CFU/m³ CFU/m³
│ │
▼ ▼
Higher bacterial Minimal bacterial
wound load wound load
│ │
▼ ▼
SSI/PJI risk ↑ SSI/PJI risk ↓
│ │
PJI rate: PJI rate:
~1-3% historically ~0.5-1%
(with antibiotics
+ body suit)
Additional Measures Used with LAF
- Body-exhaust suits (space suits) - Helmet-enclosed suits that vent personnel-shed bacteria away from the wound via a negative-pressure exhaust hose. Originally developed by Charnley.
- Prophylactic antibiotics - First-generation cephalosporins (cefazolin); the combination of LAF + antibiotics was shown to be synergistic by Lidwell et al.
- Minimizing personnel in theatre - Each additional person increases CFU/m³ by ~150 CFU/m³
- Minimizing door openings - Each opening disrupts the LAF envelope
- Ultraviolet (UV) light - Some centres use UV irradiation as an alternative or adjunct to achieve ultraclean air with bacterial counts equivalent to LAF (Campbell's 15th ed.)
- Draping - Full body drape of patient reduces skin squame dispersal
Indications in Orthopaedics
LAF is recommended (or was traditionally recommended) for:
- Total hip arthroplasty (THA)
- Total knee arthroplasty (TKA)
- Spinal instrumentation surgery
- Complex revision arthroplasty
- Open fracture fixation with implants (Campbell's 15th ed. - "A shorter duration of surgery and the presence of a free laminar airflow barrier may decrease bacterial loads")
Current Evidence and Controversy
Recent meta-analyses and registry data have repeatedly challenged the benefit of LAF in reducing SSIs and PJIs. Key points:
- 2021 Meta-Analysis (Bao & Li, PMID 33256867): Found the type of OR ventilation did not significantly affect SSI rates
- German KISS database study (2008): Paradoxically found a statistically significant increase in SSI rates with vertical laminar flow for hip prosthesis insertion compared to turbulent HEPA-filtered air
- New Zealand Joint Registry (Hooper et al., 2011): LAF combined with space suits showed no reduction in early deep infection over 10 years
- Lancet Infectious Diseases (Systematic Review): Meta-analysis concluded LAF is not superior to conventional HEPA-filtered ventilation for SSI prevention in orthopaedic surgery
Possible explanations for lack of benefit:
- Modern prophylactic antibiotics mask the effect of air quality
- LAF may cause turbulence around the surgical team (especially horizontal flow)
- Most bacteria causing PJI originate from the patient's own skin flora, not airborne sources
- Door openings and staff movement disrupt the LAF envelope
Current recommendations (ICM 2018): Recent orthopaedic literature has not demonstrated that LAF reduces SSIs or PJIs. Performing clean orthopaedic surgery in an LAF-equipped theatre is not necessary based on current evidence. (Consensus vote: Agree 81%)
Summary Table
| Feature | Details |
|---|---|
| Definition | Unidirectional uniform airflow, <10 CFU/m³ |
| Pioneer | Sir John Charnley (1960s-70s) |
| Mechanism | HEPA filtration + positive pressure + unidirectional flow |
| Preferred type | Vertical (downflow) |
| Standard | ISO 5 (Class 100) - <3520 particles ≥0.5 µm per m³ |
| HEPA efficiency | 99.97% for particles ≥0.3 µm |
| Best used with | Body exhaust suits + prophylactic antibiotics + minimal personnel |
| Current evidence | Conflicting - no clear reduction in SSI/PJI vs HEPA turbulent |
| Organisms prevented | S. aureus, S. epidermidis, Streptococcus spp. |
References:
- Campbell's Operative Orthopaedics, 15th ed. (2026) - Chapter on TKA Infection Prevention
- Campbell's Operative Orthopaedics, 15th ed. (2026) - Chapter on Fracture Related Infections
- Open Orthopaedics Journal - Current Evidence for LAF in Reducing Infection
- Orthopedic Reviews - Clean Air, Safe Joints
- Bao J & Li J. Meta-analysis on OR ventilation type and SSI. Infect Control Hosp Epidemiol 2021 Aug. [PMID 33256867]
This is a shared conversation. Sign in to Orris to start your own chat.