Did u know about shia zanjeer zani back muscles injuries
zanjeer zani self-flagellation injuries
Shia zanjeer zani back muscle injuries Ashura flagellation medical
self-flagellation musculoskeletal injury back wounds
Shia Zanjeer Zani - Back Muscle Injuries
What Happens Biomechanically
- Trapezius (upper and middle fibers) - the most exposed muscle, sits right under the skin across the upper back and shoulders
- Latissimus dorsi - the broad back muscle; gets hit in mid-back strikes
- Rhomboids (major and minor) - lie beneath the trapezius and can sustain deeper trauma if blades penetrate
- Erector spinae group (iliocostalis, longissimus, spinalis) - the paravertebral muscles running along the spine, at risk with central/lower strikes
- Muscle fiber tearing
- Hematoma formation within the muscle belly
- Damage to the thoracodorsal nerve (supplying latissimus dorsi) in severe lateral strikes
- Accessory nerve injury if the trapezius is deeply cut at the shoulder region
- Infraspinatus / teres minor (rotator cuff) - stressed during the deceleration phase of the swing
- Posterior deltoid - activated throughout the swing
- Serratus anterior - stabilizes the scapula under load
- Repeated high-velocity swinging can cause acute muscle strains or even partial rotator cuff tears, especially in participants who swing for extended durations
Skin and Superficial Tissue Layer
- Skin - lacerations, abrasions, contusions. Repeated strikes cause the skin to break down, leading to open wounds
- Subcutaneous fat - bruising and fat necrosis
- Superficial fascia - torn in deeper strikes
Infection Risk
- Tetanus - a key concern; chains are metal, often not sterile
- Staphylococcal and streptococcal wound infections
- Cellulitis progressing to necrotizing fasciitis in neglected cases (the deep fascia of the back can become infected, spreading along fascial planes)
- Osteomyelitis of posterior ribs or spinous processes is rare but documented in severe cases with very deep penetration
Neurological Risks
- Branches of the posterior rami of thoracic spinal nerves run through the back muscles - trauma can cause localized numbness or neuropathic pain patches across the back
- Spinal cord itself is protected by the vertebral column, so direct cord injury from surface strikes is extremely rare
- Pneumothorax - theoretically possible if a blade-equipped chain penetrates deep enough between the ribs, though this is uncommon
Specific Back Muscles - Summary Table
| Muscle | Location | Injury Type from Zanjeer |
|---|---|---|
| Trapezius | Upper/mid back, shoulders | Lacerations, contusions, hematoma |
| Latissimus dorsi | Mid/lower back | Contusions, deeper lacerations |
| Rhomboids | Between spine and scapula | Deeper penetrating injury |
| Erector spinae | Paravertebral columns | Contusions, strains |
| Rotator cuff muscles | Shoulder (swinging arm) | Repetitive strain, partial tears |
| Serratus anterior | Lateral chest wall | Scapular winging from strain |
Medical Management
- Wound cleaning - irrigation to remove debris, metal fragments
- Tetanus prophylaxis - mandatory
- Laceration closure - or delayed primary closure if contaminated
- Antibiotics - if signs of infection (cellulitis, deep tissue involvement)
- Imaging - ultrasound or CT if deep tissue injury, hematoma, or foreign bodies (chain fragments) are suspected
- Physiotherapy - for muscle strain recovery, especially rotator cuff
Note on Formal Literature
How to select best and commonly used suturing threads and techniques for it
suture selection guide thread types techniques clinical surgery 2024
Suture Thread Selection and Techniques
Part 1 - Characteristics of the Ideal Suture
- Easy to handle
- Predictable tensile strength
- Glides through tissues easily
- Secure knotting ability
- Minimal tissue reaction (non-allergenic, non-carcinogenic)
- Non-capillary (doesn't wick bacteria)
- Sterile and inexpensive
Part 2 - Five Key Properties to Understand Before Choosing
1. Physical Structure: Monofilament vs. Multifilament (Braided)
| Type | Pros | Cons |
|---|---|---|
| Monofilament | Slides easily, low infection risk, less tissue drag | Harder to knot, high "memory" (coils), fractures if gripped by needle holder |
| Multifilament (Braided) | Knots well, easier to handle, better feel | Bacteria lodge in interstices - avoid in contaminated wounds |
2. Strength
3. Tensile Behaviour (Memory)
4. Absorbability - the most critical selection factor
5. Biological Behaviour
Part 3 - Suture Materials: Absorbable vs Non-Absorbable
Absorbable Sutures
| Material | Trade Name | Duration of Strength | Best Uses |
|---|---|---|---|
| Polyglactin 910 | Vicryl | ~3-4 weeks | Deep tissue, fascial layers, GI anastomosis, ligatures, subcuticular skin |
| Polyglycolic acid | Dexon | ~3-4 weeks | Same as Vicryl; ligatures, bowel anastomosis |
| Polydioxanone | PDS | ~6 weeks | Abdominal wall closure, tendons, pediatric cardiac surgery - long support needed |
| Chromic catgut | (no trade name) | ~1 week | Urothelium, bile duct, mucosa - rarely used now in the UK |
| Poliglecaprone | Monocryl | ~2-3 weeks | Subcuticular skin, soft tissue - very smooth monofilament |
Non-Absorbable Sutures
| Material | Trade Name | Key Property | Best Uses |
|---|---|---|---|
| Polypropylene | Prolene | High tensile strength, retains strength indefinitely, memory | Vascular anastomosis, skin closure, hernia repair |
| Monofilament nylon | Ethilon / Monosof | High tensile strength, memory, inexpensive | Skin closure, wound closure |
| Braided nylon | Nurolon | Non-absorbable, knots well | Colonic/oesophageal anastomosis |
| Braided silk | Silk | Knots beautifully, most handleable | Colonic/oesophageal anastomosis - but loses strength over years |
| Polyester | Ethibond / Ticron | High tensile, minimal creep | Cardiac, vascular, fascial closure |
| Stainless steel | Wire | Maximum strength | Sternal closure, tendon repair |
Important: Silk and other biological non-absorbables fragment with time and should never be used in vascular anastomoses due to risk of late fistula formation. Polypropylene retains strength indefinitely and is preferred for vessels.
Part 4 - Suture Size (USP System)
| Size | Common Use |
|---|---|
| 0 / 1 | Abdominal wall, heavy fascial closure |
| 2-0 / 3-0 | Deep tissues, muscle, fascia, GI anastomosis |
| 3-0 / 4-0 | General skin closure |
| 4-0 / 5-0 | Face, hands - areas needing fine closure |
| 5-0 / 6-0 | Vascular anastomosis, ophthalmic, microsurgery |
Part 5 - The Four Core Suturing Techniques
1. Interrupted Sutures
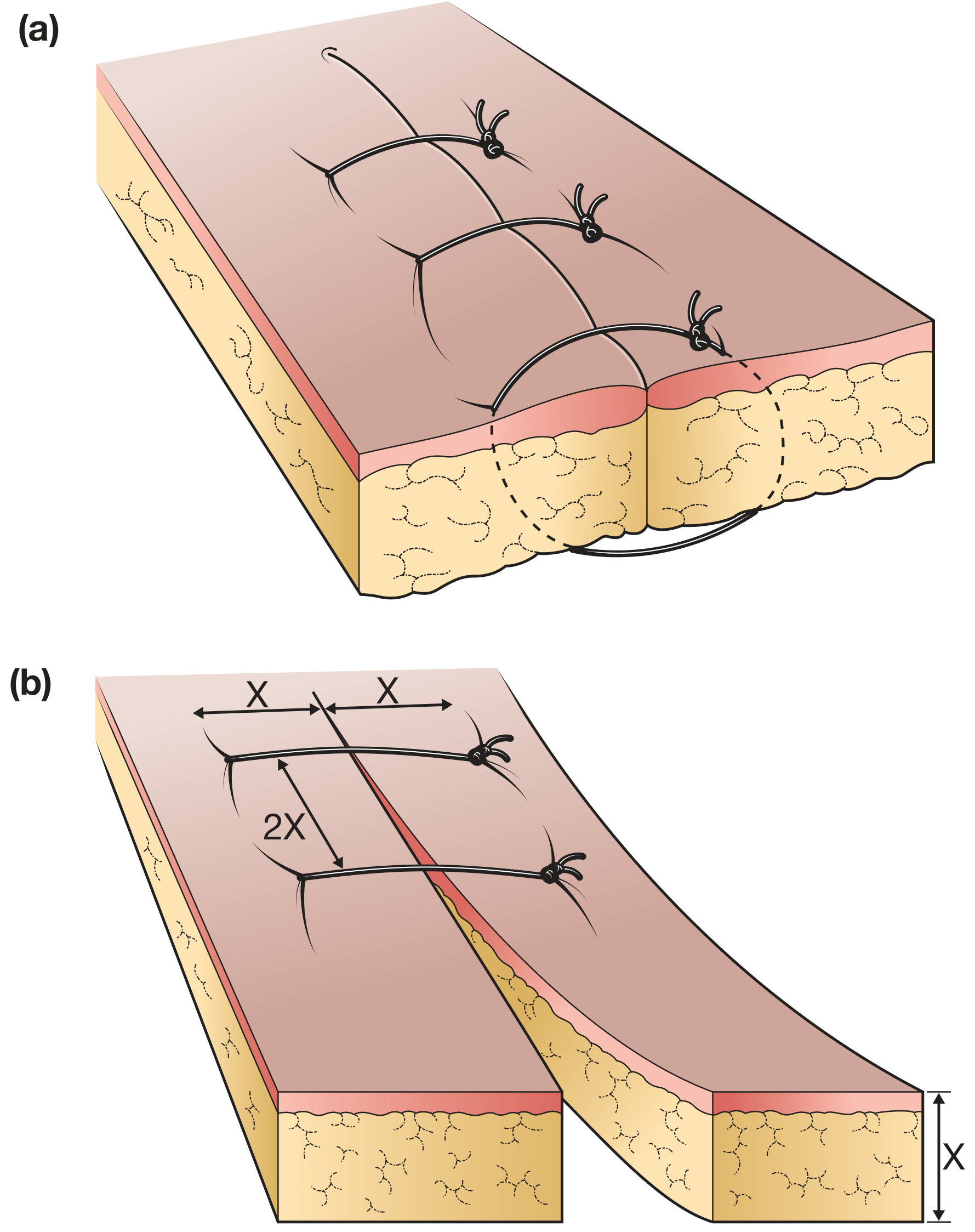
- Distance from needle entry to wound edge = depth of tissue (X)
- Spacing between sutures = 2X
- Each suture is tied and cut independently
- Advantage: if one suture fails or gets infected, the rest hold
- Best for: skin closure, contaminated wounds, areas needing individual tension control
- In long wounds, place the central suture first, then halve each remaining gap
2. Continuous Sutures
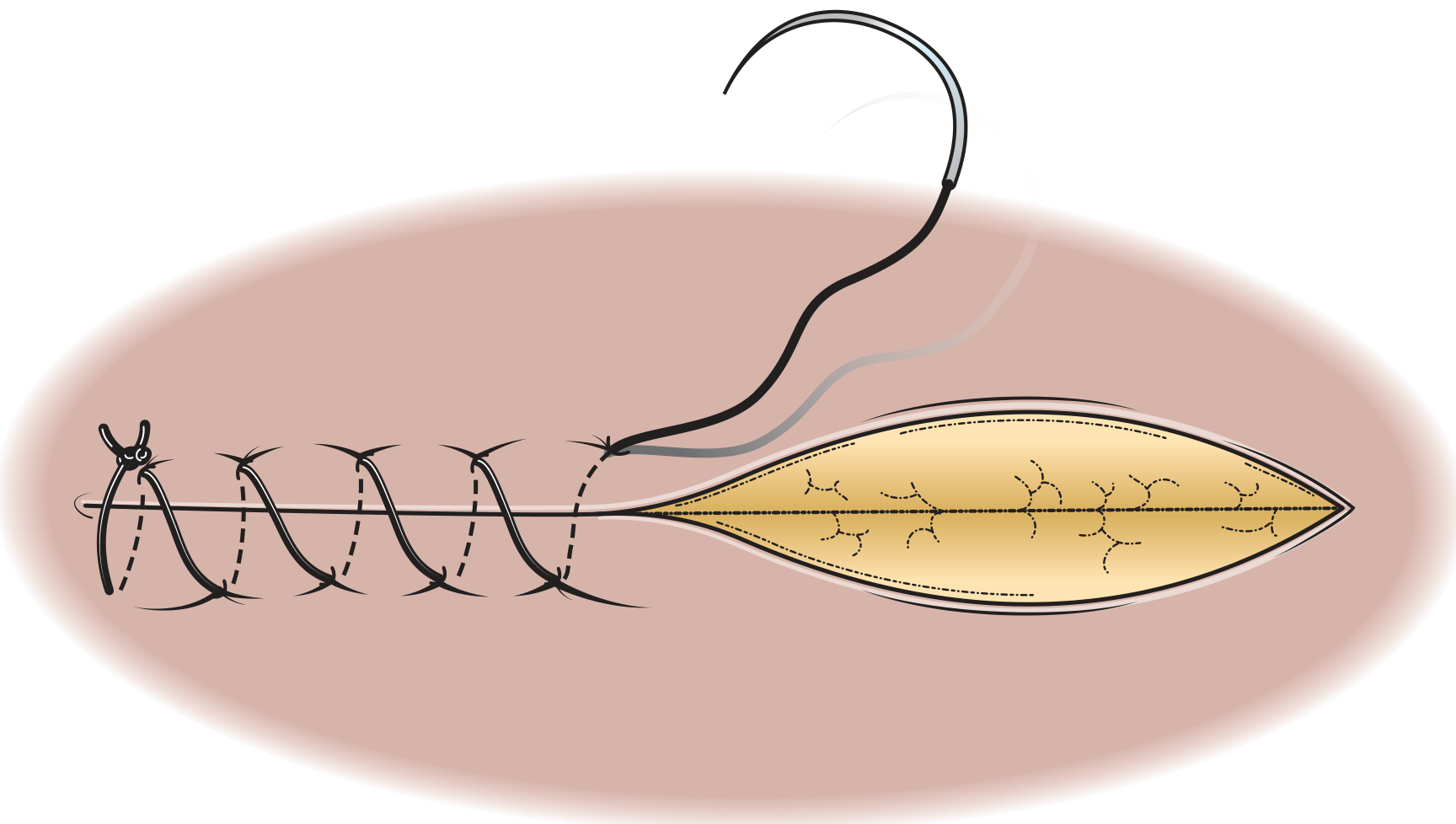
- Requires an assistant to maintain even tension throughout
- Too little suture length = purse-stringing; too slack = poor apposition
- Secured at end with an Aberdeen knot, or by tying the free end to the last loop
- Advantage: faster, watertight/airtight seal in internal organs
- Best for: bowel anastomosis, peritoneum, fascial layers, vascular anastomosis
3. Mattress Sutures (Vertical and Horizontal)
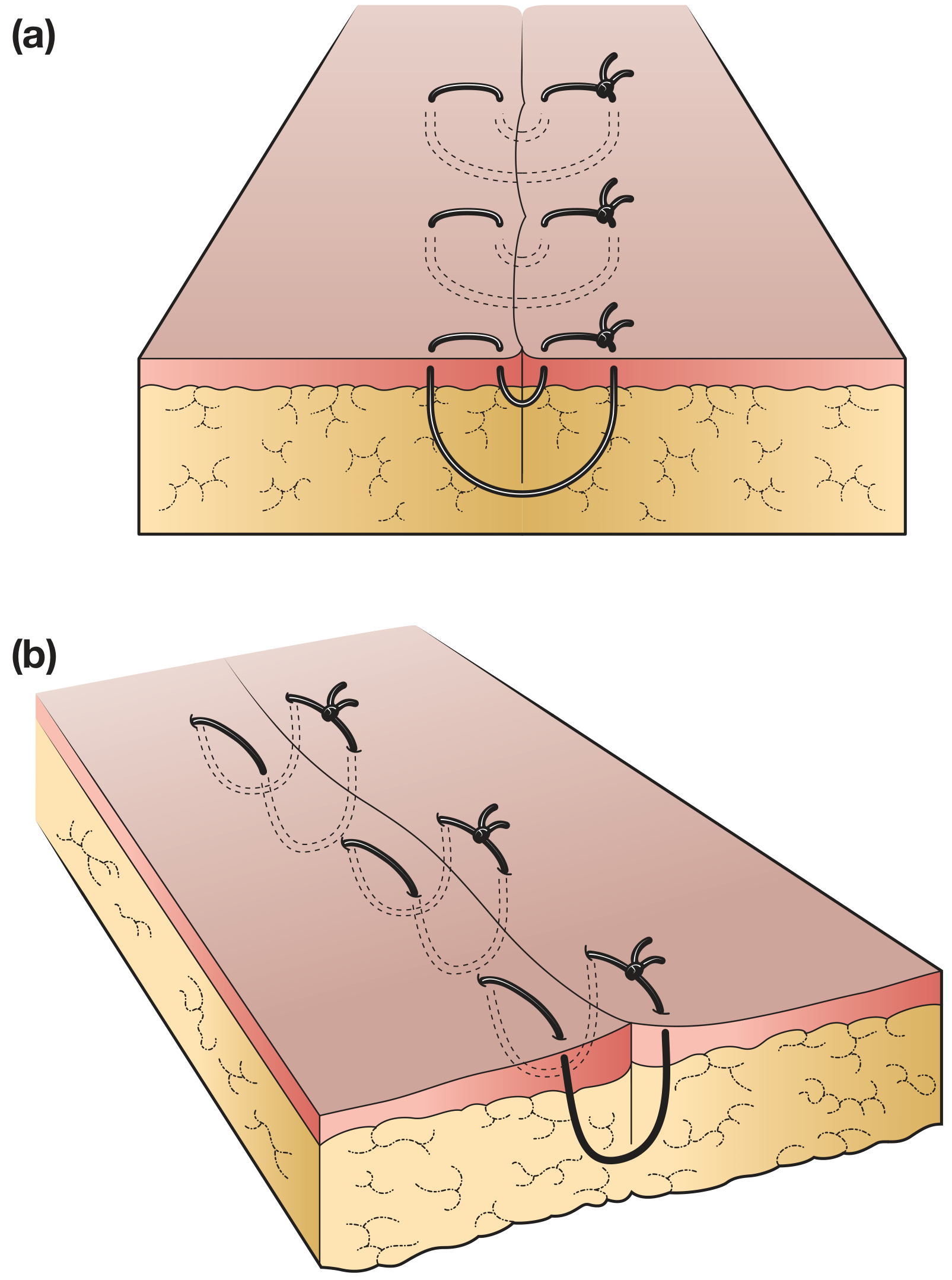
- Vertical mattress: inverts or everts wound edges; useful for skin under tension
- Horizontal mattress: good for irregular depth wounds; distributes tension over a wider area
- Best for: areas under tension (scalp, back, joints), irregular wound edges, preventing inversion
4. Subcuticular (Intradermal) Suture
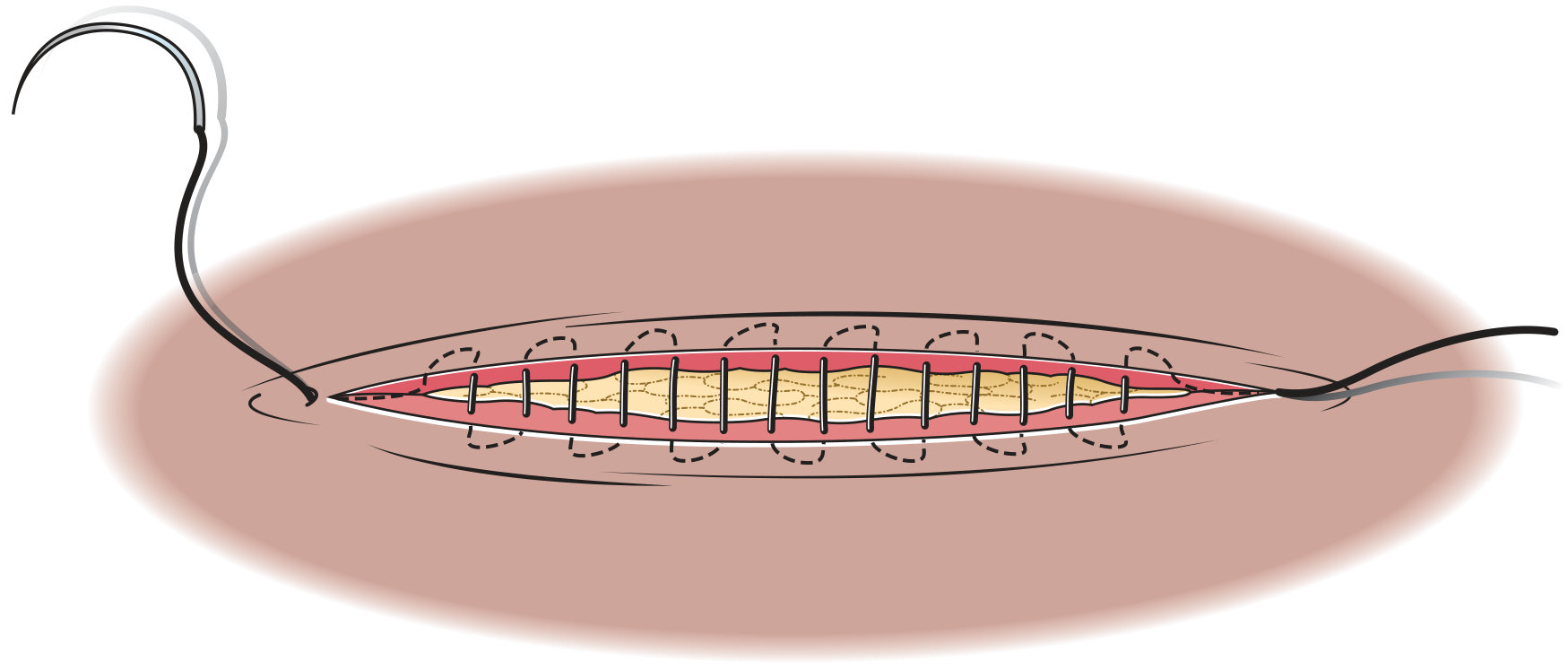
- Can be absorbable (buried knot) or non-absorbable (ends left protruding for later removal)
- No cross-hatched "train track" marks on the skin
- Best for: cosmetically important areas - face, neck, elective surgical incisions
- Requires well-aligned, tension-free wound edges
Part 6 - Practical Selection Guide by Location
| Location | Recommended Suture | Size | Technique |
|---|---|---|---|
| Face / neck | Nylon or Prolene | 5-0 / 6-0 | Interrupted or subcuticular |
| Scalp | Nylon or staples | 3-0 | Interrupted or staples |
| Trunk (clean) | Vicryl (deep), Nylon (skin) | 2-0 deep, 3-0 skin | Layered closure |
| Back / shoulder | Vicryl (deep), Nylon (skin) | 0/2-0 deep, 3-0 skin | Interrupted (high tension) |
| Fascia / aponeurosis | PDS or Prolene | 0 / 1 | Continuous mass or interrupted |
| Bowel anastomosis | Vicryl or PDS | 3-0 / 2-0 | Continuous or interrupted |
| Vascular anastomosis | Prolene | 5-0 to 7-0 | Continuous |
| Tendon | PDS or Ethibond | 3-0 / 4-0 | Interrupted or Kessler |
| Contaminated wound | Monofilament (nylon/PDS) | Appropriate size | Interrupted (never braided) |
| Deep absorbable layer | Vicryl or Monocryl | 2-0 / 3-0 | Interrupted buried knot |
Part 7 - Knot Tying Rules
- Tie firmly but do not strangulate tissue
- Keep the knot as small as possible to minimize foreign material
- Do not "saw" the thread - it cuts through tissue and weakens the material
- Lay the thread square during tying to prevent breakage
- Only grip the free end with the needle holder - gripping the thread body damages it
- Standard knot = reef knot + 1 extra throw (3 total)
- For monofilament sutures: 6 throws are required for security due to high memory and poor knot grip
Quick Decision Summary
Is the wound contaminated or infected?
YES → Monofilament only (nylon, PDS), interrupted, leave open if severe
Does the layer need to dissolve?
YES → Absorbable (Vicryl for most, PDS for prolonged support)
NO → Non-absorbable (Prolene/Nylon for skin, Prolene for vessels)
Is cosmesis important?
YES → Fine monofilament (5-0/6-0), subcuticular technique
Is there high tension?
YES → Larger size (0/1), mattress technique, consider deep layer first
Is it vascular?
YES → Prolene only (retains strength indefinitely), continuous, fine (5-0+)
- Bailey and Love's Short Practice of Surgery, 28th Ed., pp. 125-129
- Pye's Surgical Handicraft, 22nd Ed., Table 18.1
What can be best for zanjeer zani wounds
contaminated traumatic laceration wound management suture selection guidelines
Best Management of Zanjeer Zani Wounds
- Multiple lacerations across the upper back
- Metal (chain) instrument - contaminated, often non-sterile, may have blade attachments
- Irregular wound edges from repeated strikes
- Variable depth - some superficial, some reaching fascia
- Delayed presentation - participants often present hours after the ritual ends
- High bacterial load from skin flora + metal contamination
- No single wound - multiple wounds at different stages simultaneously
Step 1 - Classify Each Wound Before Touching It
- How deep is it? (Superficial skin only vs. into fascia/muscle)
- How old is it? (Less than 8 hours = primary closure still possible if cleaned well; over 12 hours = delayed closure)
- Are wound edges viable? (Devitalized, macerated tissue must be debrided first)
- Any signs of infection already? (Redness, pus, warmth = no closure, treat open)
Step 2 - Wound Preparation (Most Important Step)
A. Anesthesia First
- Infiltrate each wound with lidocaine 1% without epinephrine (epinephrine is avoided on highly vascular areas under tension)
- Regional nerve blocks of the thoracic posterior rami can be considered for multiple simultaneous wounds
B. Skin Disinfection Around (Not Inside) the Wound
- Chlorhexidine applied to surrounding skin is preferred over povidone-iodine (meta-analysis of 13 RCTs, 6,997 patients: chlorhexidine gave 30% lower surgical site infection rate)
- Allow 2-3 minutes to dry for full effect
- Do not pour antiseptic directly into the wound - it damages tissue defences and impairs healing
C. Wound Irrigation - the single most important infection-prevention step
- Irrigate with normal saline or clean tap water
- Use moderate pressure (10-15 psi with a 35 mL syringe and 19-gauge needle, or splash shield)
- Very high pressure (>15 psi) is avoided - it drives bacteria deeper into tissue
- Volume: at least 100-200 mL per wound for heavily contaminated ones
- If extremely dirty: pre-irrigation with soap and water under running tap before anesthesia is acceptable when patient tolerates it
D. Sharp Debridement
- Remove all obviously devitalized tissue, clotted haematoma, and embedded debris with scissors or scalpel
- Metal fragments from chains must be actively searched for - use plain X-ray to locate radiopaque fragments, ultrasound for soft tissue foreign bodies
- Do not leave dead tissue behind - it is a culture medium for bacteria
E. Wound Exploration
- Systematically probe each wound for depth
- Check for tendon injury (ask patient to move shoulder and scapular muscles)
- Check neurovascular status distal to the injury site
Step 3 - Closure Decision by Wound Type
Superficial lacerations (skin/subcutaneous only, <8 hours old, clean after irrigation)
Deep lacerations (into fascia/muscle, or >8-12 hours old, or heavily contaminated)
- Pack the wound open with petrolatum (Vaseline) gauze between edges
- Start the patient on oral antibiotics (cephalexin 500 mg QID x 5 days)
- Return on Day 3 - re-anaesthetise, re-irrigate, then close primarily
- At delayed closure: use non-absorbable monofilament skin sutures only - no deep sutures, as deep sutures in contaminated wounds increase infection risk significantly
Infected / frankly purulent wounds
- Daily dressing changes
- Consider NPWT (wound VAC) for large open back wounds - changes every 2-3 days
Step 4 - Best Suture Choice for These Wounds
| Wound Layer | Best Suture | Size | Reason |
|---|---|---|---|
| Skin (clean, primary closure) | Monofilament nylon (Ethilon) or Prolene | 3-0 | Monofilament = no bacterial harbouring in interstices; non-absorbable = removable, predictable |
| Skin (delayed primary, Day 3) | Monofilament nylon | 3-0 | Same reason - no deep sutures at this stage |
| Deep fascia (clean, primary only) | PDS (polydioxanone) | 1-0 / 0 | Slow absorption, holds tension for weeks while contaminated deep tissue heals |
| Muscle layer (if needed) | Vicryl | 2-0 | Absorbable, dissolves without removal |
Never use braided sutures (Vicryl, silk, braided nylon) for skin closure in these wounds. The interstices of braided material harbour bacteria and dramatically increase infection risk in a dirty wound. Monofilament only for skin.
Technique for the Back
- Interrupted sutures - mandatory (not continuous) because:
- If one suture site gets infected, you can remove that single suture and drain it without losing the entire closure
- Back wounds are under tension with shoulder movement - interrupted handles differential tension better
- Easier to adjust for irregular wound edges
- Vertical mattress sutures for areas under high tension (upper back near shoulder) - distributes tension, prevents inversion
- Do not use subcuticular sutures in these wounds - too risky in contaminated tissue, cannot be partially opened if infection develops
Siting Rule (from Bailey & Love)
- Needle entry distance from wound edge = depth of tissue being sutured (X)
- Spacing between sutures = 2X
- Knot: reef knot + 1 extra throw (3 total); for nylon/monofilament = 6 throws for security
Step 5 - Tetanus Prophylaxis (Mandatory)
| Vaccination Status | Action |
|---|---|
| Up to date (booster within 5 years) | Nothing needed |
| Last booster >5 years ago | Td/Tdap booster |
| Unknown / unvaccinated | Td/Tdap + Tetanus Immunoglobulin (TIG) on opposite limb |
Step 6 - Antibiotics
| Situation | Antibiotic |
|---|---|
| Clean wound, primary closure | Not routinely needed |
| Delayed primary closure | Cephalexin 500 mg QID x 5 days |
| Signs of infection (cellulitis) | Co-amoxiclav (Augmentin) or Cephalexin |
| Deep tissue / fascia involvement | Add metronidazole for anaerobic cover (especially if wound is deep and closed off) |
| Suspected necrotising fasciitis | Surgical emergency - IV Pip-Tazo + Clindamycin, immediate debridement |
Step 7 - Dressings After Closure
- Closed wounds: non-adherent primary dressing (Mepore/Melolin) + secondary absorbent pad
- Open wounds (secondary intention): saline-moistened gauze or NPWT (Wound VAC) for large wounds
- Change dressings daily for open wounds
- Keep dry for 24-48 hours post-closure
Suture Removal Timeline for Back Wounds
| Location | Removal |
|---|---|
| Face | 3-5 days |
| Trunk / abdomen | 10-14 days |
| Back (high tension) | 12-14 days minimum |
| Scalp | 7-10 days |
Summary - Quick Decision Card for Zanjeer Zani
Every wound → irrigate first, debride devitalized tissue, search for metal fragments
< 8 hours old + clean after irrigation?
→ Primary closure: interrupted monofilament nylon 3-0, no braided sutures
> 8-12 hours old OR heavily contaminated?
→ Pack open, antibiotics, delayed primary closure Day 3
Infected / purulent?
→ Leave open, secondary intention, daily dressings
ALWAYS: Tetanus prophylaxis, assess vaccination status
ALWAYS: X-ray to exclude retained metal fragments
During hot summer what precautions should be applied regarding suturing and dressing
wound care suturing hot weather summer heat sweating infection precautions dressing
Suturing and Dressing Precautions in Hot Summer Weather
Why Hot Weather Makes Wounds Worse - The 5 Mechanisms
1. Sweating = Moisture = Bacterial Growth
2. Maceration
3. Excess Wound Exudate
4. Desiccation at the Wound Surface
5. Dressing Adhesive Failure
Precautions During the Suturing Procedure Itself
Keep the Wound and Operative Field Cool and Dry
- Work in an air-conditioned or shaded, cool environment if possible
- Patient should be lying prone (for back wounds) and comfortable - excessive sweating during the procedure itself contaminates the field
- Fan or cool cloth on non-operative areas reduces sweating during procedure
Do Not Rush Wound Preparation
Suture Selection Adjustments for Hot Weather
| Factor | Standard Advice | Hot Weather Modification |
|---|---|---|
| Material for skin | Monofilament nylon/Prolene | Same - monofilament remains best choice. Braided sutures harbour more bacteria; worse in summer |
| Absorbable deep layer | Vicryl | PDS preferred in hot/humid conditions - slower absorption means it holds longer if wound healing is delayed by heat/infection |
| Suture tightness | Snug | Slightly looser - swelling from heat/inflammation means tight sutures cut through oedematous tissue within 24-48 hours |
| Number of sutures | As needed | Minimum necessary - each suture is a foreign body and a portal for infection; fewer is better in contaminated/hot conditions |
| Deep sutures | Used routinely | Avoid or minimize in contaminated wounds in summer - deep sutures in a warm, swollen wound increase infection risk significantly |
Do Not Use Subcuticular/Intradermal Sutures in Summer Back Wounds
Dressing Selection in Hot Weather
Dressing Types and Their Summer Suitability
| Dressing Type | How It Works | Summer Suitability | Best For |
|---|---|---|---|
| Plain dry gauze | Absorbs, but dries wound | Poor - causes rapid desiccation in dry heat, becomes saturated in humidity | Avoid as sole dressing in summer |
| Petroleum-impregnated gauze (Jelonet/Vaseline gauze) | Non-adherent, keeps wound moist | Good - prevents desiccation, non-traumatic removal | Fresh suture lines, superficial wounds |
| Foam dressing (e.g., Mepilex) | Absorbs excess exudate, cushions | Excellent for summer - handles high exudate from heat-related inflammation, breathable | Moderately-heavily exuding wounds, back wounds |
| Hydrocolloid (e.g., DuoDERM) | Semi-occlusive gel-forming | Moderate - waterproof but may trap heat; change every 3-5 days | Low-moderate exudate, skin intact around wound |
| Film dressing (e.g., Tegaderm) | Transparent, waterproof, not absorptive | Poor for hot weather - traps sweat under it, zero absorption | Only for very low exudate, sealed clean wounds |
| Silver-containing dressing (e.g., Aquacel Ag) | Antimicrobial + absorptive | Excellent for infected/high-risk summer wounds - silver inhibits bacterial growth continuously | Contaminated wounds, high infection risk, post-op back wounds |
| Hydrogel sheet | Donates moisture, cooling | Good for dry wounds in dry heat | Dry/sloughy wounds, not exuding wounds |
Best Choice for Back Wounds in Summer (Zanjeer Zani context):
- Primary layer: Petroleum gauze (Jelonet) or non-adherent silicone layer (Mepitel) - atraumatic, won't stick to wound surface
- Secondary layer: Foam dressing (Mepilex/Allevyn) - absorbs sweat + exudate, breathable, stays in place better than plain gauze
- For high infection risk: Add silver alginate layer against the wound bed before foam
Dressing Change Frequency in Summer
| Condition | Standard Change | Summer Change |
|---|---|---|
| Clean sutured wound, low exudate | Every 24-48 hours | Every 24 hours minimum |
| Contaminated/back wound, moderate exudate | Daily | Twice daily if sweating heavily |
| Infected wound | Daily | Twice daily with irrigation each time |
| Open wound (secondary intention) | Daily | Twice daily - moist saline gauze |
- Gentle cleansing with normal saline (not povidone-iodine directly into wound)
- Visual inspection for early infection signs (see below)
- Fresh dressing applied to dry skin
Warning Signs to Actively Teach the Patient (Especially in Summer)
- Redness spreading beyond the wound edges (cellulitis)
- Increasing warmth and throbbing pain after the first 24 hours (pain should be decreasing, not increasing)
- Pus or cloudy discharge from the wound
- Fever >38°C
- Red lines tracking up from the wound (lymphangitis - this is a medical emergency)
- Foul odour from the wound or dressing
- Sutures cutting into swollen, tight skin
- Dressing coming off and wound being exposed to dirt/sweat for hours
Patient Instructions Specific to Summer
Keep the Wound Area Cool and Dry
- Stay in shade or air-conditioned areas as much as possible
- Do not leave the wound exposed to direct sunlight - UV and heat both impair healing and increase inflammation
- Avoid activities causing heavy sweating for at least the first 48-72 hours
Clothing
- Wear loose, breathable cotton over back wounds - not tight synthetic fabric that traps heat and sweat against the wound
- No polyester, no tight elastic waistbands near wounds
Hydration - Critical and Often Overlooked
- Hot weather dehydration reduces blood volume directly
- Less blood flow to the wound = less oxygen + fewer immune cells delivered = slower healing + higher infection risk
- Minimum 2.5-3 litres of water per day in summer for wound patients
Bathing
- Safe to gently wet the wound 24 hours after repair
- After bathing: pat dry immediately, do not rub; re-apply dressing
- No swimming or immersion in water (pools, rivers) until fully healed - these carry high bacterial load + prolonged moisture exposure
Nutrition
- Protein (chicken, fish, lentils), Vitamin C (citrus), and Zinc (nuts, seeds) all directly support wound healing
- These requirements are elevated in summer when the body is under thermal stress
Suture Removal - Adjust for Summer
- Wound edges are fully approximated and sealed
- No signs of infection
- Skin around sutures is not macerated or breaking down
Quick Summer Wound Checklist
AT SUTURING:
✓ Cool environment, chlorhexidine skin prep, allow to dry 2-3 min
✓ Monofilament sutures only (nylon/Prolene) for skin
✓ Slightly looser ties - allow for swelling
✓ Minimum sutures needed - avoid unnecessary deep sutures
✓ Tetanus prophylaxis (especially for metal wounds)
DRESSING:
✓ Non-adherent primary layer (Jelonet or Mepitel)
✓ Absorptive foam secondary layer - NOT plain dry gauze alone
✓ Silver-containing layer if contaminated/high risk
✓ Change every 24h minimum; twice daily in heavy sweating
PATIENT INSTRUCTIONS:
✓ Stay cool, loose cotton clothing
✓ Hydrate 2.5-3L/day
✓ No swimming, no direct sun on wound
✓ Return immediately for: spreading redness, fever, pus, red lines, foul smell
✓ Suture removal at 12-14 days (back wounds)
Can we protect our face through mask
face protection mask shield sports trauma laceration prevention types
https://www.drducic.com/wp-content/uploads/2022/01/FACIAL1.p…
Can a Mask Protect the Face During Zanjeer Zani?
What Are You Protecting Against?
- Accidental chain swing - the chain overshoots and strikes the face (most common injury mechanism)
- Blade-tipped chains - lacerations to cheek, nose, periorbital area
- Blunt impact - from chain links hitting the nose, cheekbones, or orbit
- Eye injury - the orbit is the most dangerous - even a single chain link at velocity can rupture the globe
Types of Face Protection - What Works and What Doesn't
1. Cloth / Surgical Masks
- Designed only for respiratory protection (dust, droplets)
- Offer zero resistance to chain impact or lacerations
- Actually dangerous if used with a false sense of security
- Do NOT use as trauma protection
2. Hard Polycarbonate Face Shield (Full-Face or Half-Face)
- The gold standard for high-impact facial protection
- Polycarbonate is shatter-resistant, lightweight, and can absorb and disperse kinetic energy
- Used in combat sports, industrial work, and by surgeons repairing facial fractures to prevent re-injury
- Covers: forehead, nose, cheeks, chin
- Custom-made versions (moulded over a cast of the face) offer the best fit and energy dissipation
- Off-the-shelf versions (e.g., anti-riot shields, sports face guards) offer good protection at lower cost
- Evidence: helmets and face guards reduce facial injury risk by 28-69% in high-impact sports (American Association of Oral and Maxillofacial Surgeons data)
3. Wire Cage / Metal Face Guard (like a fencing mask or hockey cage)
- The cage structure deflects chain links effectively
- Used in ice hockey, lacrosse, cricket wicket-keepers
- Gaps between wire = risk of thin blade-tipped chain link passing through at high velocity
- Better than nothing; ideal if polycarbonate is unavailable
- Must fit tightly - a loose cage can be pushed into the face on impact
4. Sports Face Guard (Attached to Helmet)
- Football/rugby/cricket helmet + face guard combination
- Helmet protects the skull and temporal region; face guard deflects chain from face
- NOCSAE-standard face guards (US standard) are tested for significant impact
- Bulky but provides the most comprehensive craniofacial protection
- Ideal for those wishing to participate while minimising all risk
5. Eye Protection (Goggles / Wraparound Glasses)
- Orbital blowout fractures and globe rupture are the most devastating injuries from chain strikes
- A chain link hitting the orbit at speed can cause permanent vision loss
- Use polycarbonate wraparound goggles (not regular glasses - glass lenses shatter and worsen injury)
- These should be worn even under a full face shield as a secondary layer
- Industrial safety goggles rated for ballistic/impact (ANSI Z87.1 standard) are appropriate
6. Nose Guard (Nasal Splint/Shield)
- Thermoplastic or polycarbonate nasal guards protect the nasal bones from fracture
- Used by athletes after nasal fracture repair to prevent re-injury
- Covers only the nose - does not protect the rest of the face
- Useful as additional coverage if a full face mask is not worn
The Most Important Vulnerable Areas on the Face
| Area | Risk from Chain Strike | Protection Priority |
|---|---|---|
| Eyes / orbit | Globe rupture, orbital fracture, vision loss | Highest - must protect |
| Nose | Nasal bone fracture, septal haematoma | High |
| Cheeks / zygomatic arch | Zygomatic fracture, laceration | Moderate |
| Lips / teeth | Lacerations, dental avulsion | Moderate |
| Forehead / temples | Lacerations, temporal artery injury | Moderate |
| Ears | Auricular haematoma (cauliflower ear), lacerations | Lower |
What to Actually Recommend
Minimum Protection
- Polycarbonate wraparound safety goggles (impact-rated) - mandatory for eye protection
- A wire cage face guard or half-face polycarbonate shield covering nose and cheeks
Best Protection
- Full-face polycarbonate shield (like a motorcycle visor or industrial face shield)
- Polycarbonate goggles underneath for secondary eye protection
- Mouthguard (boil-and-bite or custom) to protect teeth and absorb jaw impact
For Bystanders / Medical Personnel
- Surgical/N95 mask + eye protection - adequate for bloodborne exposure protection (splatter from open wounds)
- This is actually important: open back wounds in multiple participants = hepatitis B/C and HIV transmission risk from chain sharing and blood splatter
Why the Face is So High-Risk - Anatomically
- Rich blood supply - facial lacerations bleed heavily even when small; chain cuts to the face bleed dramatically
- Thin bone - the nasal bones, orbital walls (as thin as paper in places), and the zygomatic arch fracture relatively easily
- Vital structures close to surface - the globe, facial nerve branches, parotid duct, lacrimal system are all superficial
- Cosmetic consequences - facial scars are permanent and visible; sutures on the face must be fine (5-0 / 6-0) and meticulous
- Airway proximity - severe mid-face trauma can compromise the nasal airway
If a Face Injury Occurs Despite Protection
| Injury | Immediate Action |
|---|---|
| Eye hit / visual change | Cover eye, do NOT press, go to ophthalmology immediately |
| Nose hit + deformity | Ice pack (not direct), ENT review within 5-7 days before swelling makes assessment impossible |
| Deep cheek laceration | Assess for facial nerve injury (ask patient to smile/raise eyebrows) before suturing |
| Heavy facial bleeding | Direct pressure, DO NOT pack nose blindly if there is head injury |
| Tooth knocked out | Store in milk or saliva, dental referral within 30-60 minutes for re-implantation |
Bottom Line
| Mask Type | Trauma Protection | Recommended? |
|---|---|---|
| Cloth / surgical mask | None | No (for trauma) |
| Wire cage face guard | Good | Yes - minimum standard |
| Polycarbonate face shield | Excellent | Yes - first choice |
| Full helmet + face guard | Excellent | Best overall |
| Impact goggles | Excellent for eyes | Yes - always, even under other masks |
| Nasal guard only | Good for nose only | Use as addition, not sole protection |
What if I close facia and subcutaneous with together