i am urology resident patient came here with complaint of luts and he is case of BPH so teach me how to proceed it
"benign prostatic hyperplasia" AND "lower urinary tract symptoms" AND management
BPH with LUTS: Complete Clinical Approach for the Urology Resident
1. ANATOMY FIRST - Know Your Prostate Zones
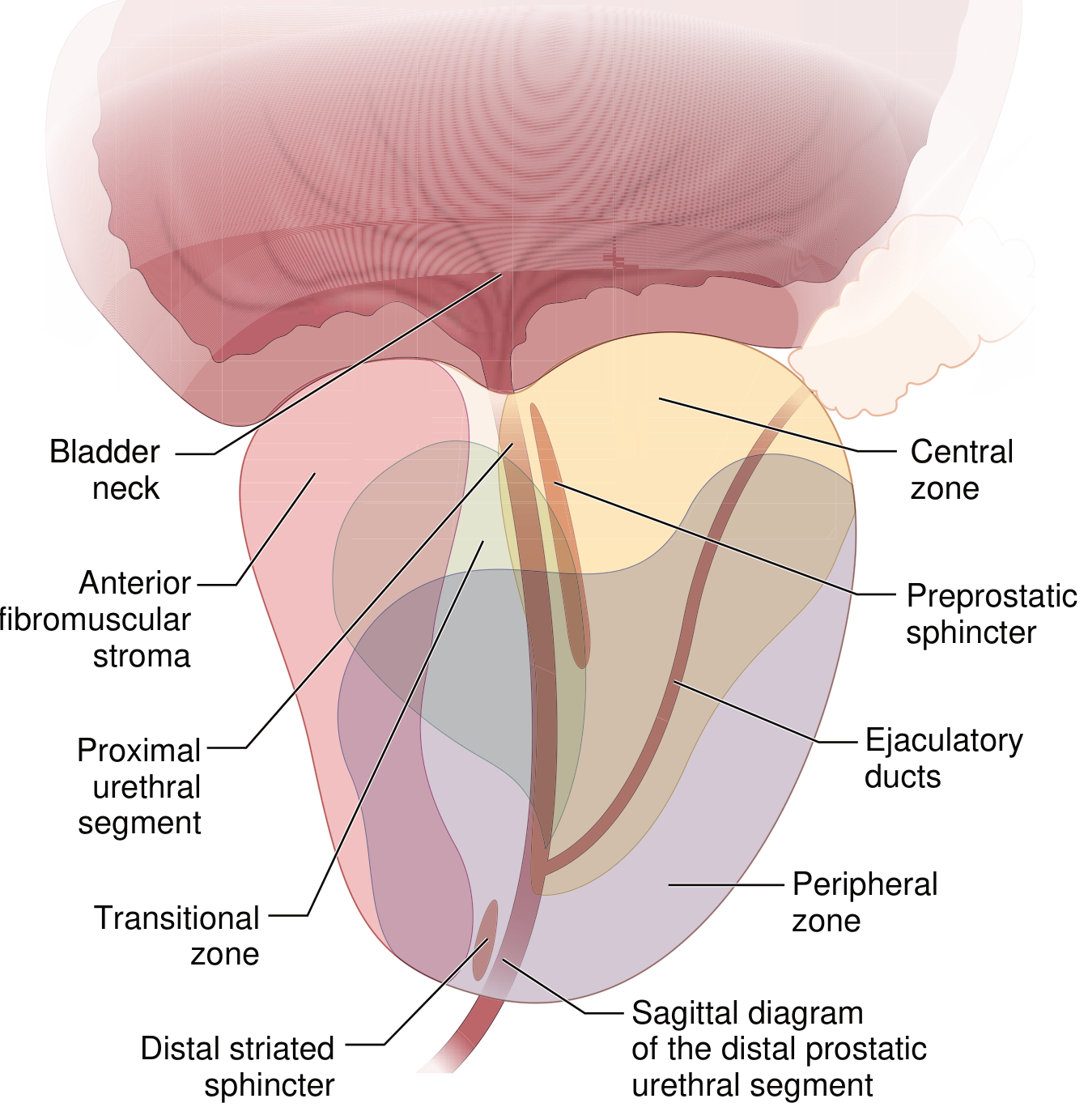
- Transitional zone - where BPH arises (nodular hyperplasia here)
- Peripheral zone - where 70% of prostate cancers arise (palpable on DRE)
- Central zone - surrounds ejaculatory ducts
- Anterior fibromuscular stroma - no glandular tissue
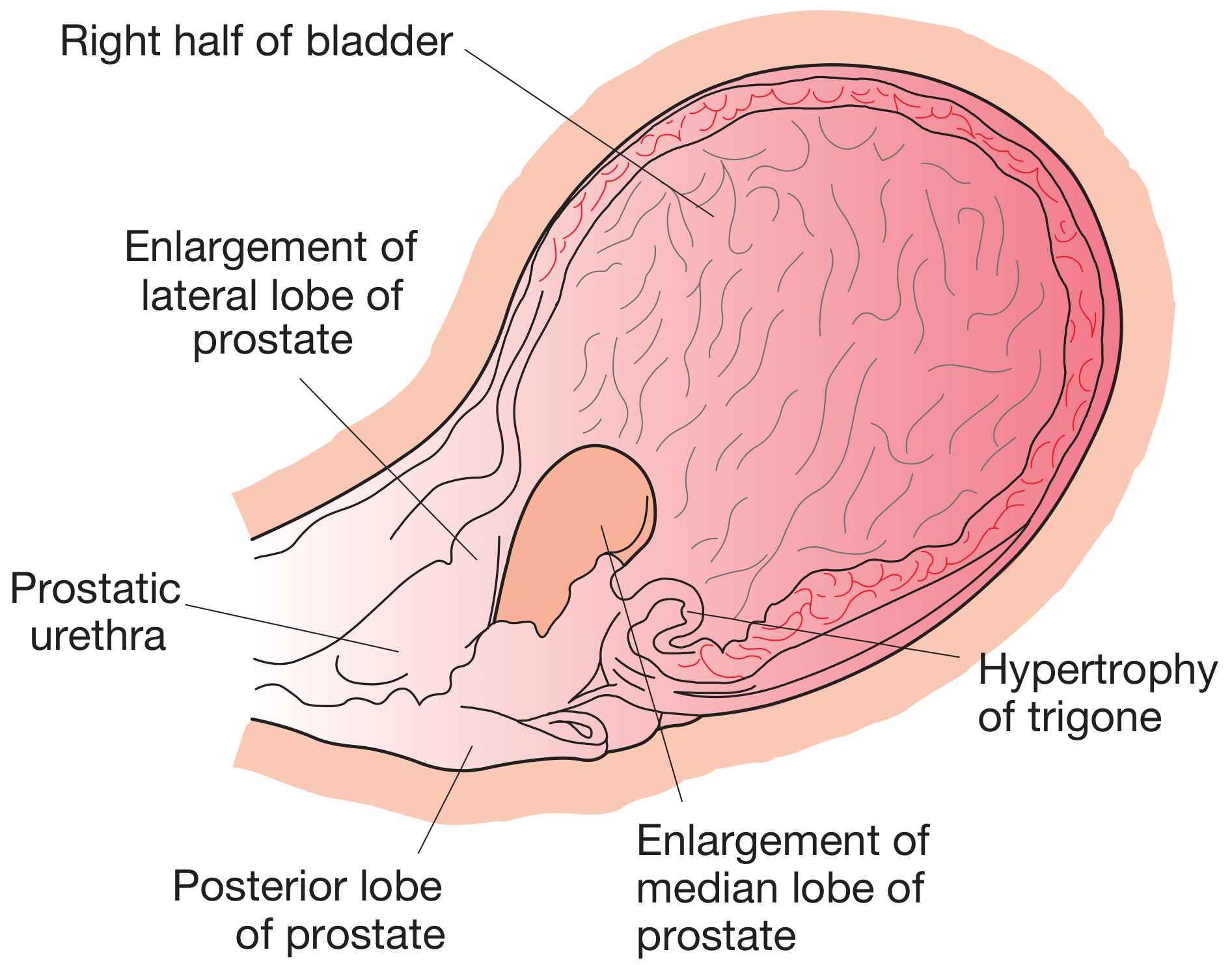
In BPH, the transitional zone enlarges nodularly, compressing the peripheral zone into a "false capsule." When the central zone is involved, a middle lobe projects upward into the bladder.
2. UNDERSTANDING LUTS - Classification
| Category | Symptoms | Mechanism |
|---|---|---|
| Storage (Irritative) | Frequency, urgency, nocturia, urge incontinence | Overactive detrusor / reduced capacity |
| Voiding (Obstructive) | Hesitancy, weak/intermittent stream, straining, terminal dribbling, prolonged voiding | Bladder outlet obstruction (BOO) |
| Post-micturition | Post-void dribble, sensation of incomplete emptying | Residual urine in urethra / bladder |
- BPH can exist with no symptoms and no BOO
- BOO can exist with no symptoms
- LUTS can be present without BPH (other causes)
3. PATHOPHYSIOLOGY
- Static (mechanical) component: Enlarged transitional zone physically narrows the prostatic urethra
- Dynamic component: Alpha-1 adrenoceptors in prostatic smooth muscle and bladder neck increase muscle tone → increased outlet resistance
- Detrusor overactivity → storage symptoms
- Eventually decompensation → large residual volumes → chronic retention
4. HISTORY TAKING
A. Symptom Assessment - IPSS
- Incomplete emptying
- Frequency (voiding <2 hours)
- Intermittency
- Urgency
- Weak stream
- Straining to void
- Nocturia
- 0-7: Mild (watchful waiting)
- 8-19: Moderate (medical therapy)
- 20-35: Severe (consider surgery)
B. Ask Specifically About
- Duration of symptoms and progression
- Haematuria (terminal haematuria can be BPH; frank haematuria needs full evaluation)
- Acute urinary retention episodes
- Urinary tract infections (recurrent UTIs suggest high residual volumes)
- Overflow incontinence or enuresis (suggests chronic retention)
- Sexual function (erectile dysfunction - relevant for medication choice; ejaculatory dysfunction)
C. Medications Review
- Alpha-agonists (nasal decongestants, pseudoephedrine) - increase bladder neck tone
- Anticholinergics (antihistamines, tricyclics, some antipsychotics) - impair detrusor
- Diuretics - worsen frequency/nocturia
D. Past History
- Urethral trauma/instrumentation (stricture)
- Previous pelvic surgery
- Neurological conditions: Parkinson's, multiple sclerosis, diabetes, spinal cord disease (all can cause LUTS mimicking BPH)
- Cerebrovascular disease
E. Frequency-Volume Diary
- Identifying polyuria/nocturnal polyuria
- Establishing functional bladder capacity
- Differentiating overactive bladder from BOO
5. PHYSICAL EXAMINATION
Abdominal Examination
- Palpate/percuss for a distended bladder above the pubic symphysis - may be visible in chronic retention (loss of suprapubic skin crease)
- Identify any renal mass
- Scars from previous surgery
Digital Rectal Examination (DRE)
- Size - rough estimate (normal ~20 mL, enlarged may be 30-100 mL+); only the posterior half is palpated so DRE underestimates size
- Consistency - BPH is rubbery/smooth
- Symmetry - BPH is generally symmetric
- Median sulcus - may be obliterated with enlargement
- Surface - hard/irregular nodule raises suspicion for prostate cancer
- Tenderness - warm, tender, boggy prostate = prostatitis
Neurological Examination
- Lower limb power, tone, reflexes
- Anal sphincter tone
- Mental status
- Any signs of cord compression (retention can be the presenting feature of cauda equina)
6. INVESTIGATIONS
Essential (for every patient)
| Test | Rationale |
|---|---|
| Urinalysis + culture | Rule out UTI (infection can cause/worsen LUTS), haematuria (may indicate cancer, stones) |
| Serum creatinine + electrolytes + haemoglobin | High-pressure chronic retention causes bilateral hydronephrosis and renal impairment |
| Uroflowmetry | Q-max (peak flow rate): >15 mL/s normal, 10-15 equivocal, <10 suggests BOO; void volume must be >150-200 mL to be valid |
| Post-void residual (PVR) | Measured by ultrasound; <50 mL normal, 50-200 mL mild, >200 mL significant |
Additional (based on clinical picture)
| Test | When / Why |
|---|---|
| PSA | All men being considered for treatment (to exclude significant prostate cancer before starting 5-ARIs; PSA also predicts prostate volume and BPH progression) |
| Transrectal or transabdominal ultrasound (TRUS) | Accurate prostate volume measurement; guides drug choice (5-ARIs most beneficial if prostate >30-40 mL); also shows intravesical protrusion of median lobe |
| Renal/bladder ultrasound | If elevated creatinine, recurrent UTI, haematuria; look for hydronephrosis, bladder wall thickening, diverticula, stones |
| Urine cytology + cystoscopy | If haematuria present (must exclude bladder cancer, carcinoma in situ before attributing haematuria to BPH); also before planned surgery to exclude stricture, bladder carcinoma |
| Pressure-flow urodynamics | When diagnosis is uncertain (young patient, neurological disease, previous failed surgery, equivocal flow rates); gold standard for BOO diagnosis |
| CT urography/IVU | If haematuria and upper tract evaluation needed |
- Q-max >15 mL/s with voided volume >200 mL = normal
- Q-max 10-15 mL/s = equivocal
- Q-max <10 mL/s = strongly suggests BOO (but can also be weak detrusor)
- Voiding pressures >80 cmH2O = high; <60 cmH2O = normal
7. DIFFERENTIAL DIAGNOSES TO EXCLUDE
- Prostate cancer - hard/nodular DRE, elevated PSA; biopsy if suspicious
- Urethral stricture - history of STI, urethral trauma, catheterisation; poor stream from young age; diagnosed on urethrogram/cystoscopy
- Bladder cancer - haematuria; urine cytology, cystoscopy
- Overactive bladder (OAB) - dominant storage symptoms, small voided volumes, urgency incontinence; urodynamics shows detrusor overactivity
- Neurogenic bladder - Parkinson's, MS, spinal cord disease, diabetes; neurological examination and history
- Bladder neck dyssynergia - younger men; urodynamics needed
- Detrusor underactivity - elderly men; poor stream + large PVR but low voiding pressure on urodynamics; surgery will not help
- Prostatitis - acute or chronic; tenderness, fever, perineal/pelvic pain
8. MANAGEMENT
Step 1 - Assess Severity and Bother
| IPSS Score | Management Path |
|---|---|
| 0-7 (mild) | Watchful waiting + lifestyle advice |
| 8-19 (moderate), low bother | Watchful waiting or medications |
| 8-19 (moderate), high bother | Medical therapy |
| ≥20 (severe) | Medical therapy; surgery if refractory |
Step 2 - Lifestyle Modifications (all patients)
- Reduce fluid intake in evening (reduces nocturia)
- Avoid caffeine and alcohol
- Double voiding technique
- Bladder retraining (timed voiding)
- Treat constipation
- Review and stop offending medications
Step 3 - Medical Therapy
Alpha-1 Adrenoceptor Blockers (Alpha-blockers) - FIRST LINE
| Drug | Dose | Notes |
|---|---|---|
| Tamsulosin | 0.4 mg OD | Uroselective (α1A); fewer BP effects; STOP before cataract surgery (floppy iris) |
| Silodosin | 4-8 mg OD | Highly uroselective; retrograde ejaculation common |
| Alfuzosin | 10 mg OD | Less ejaculatory side effects |
| Doxazosin | 1-8 mg OD | Non-selective; also treats hypertension; more postural hypotension |
| Terazosin | 1-10 mg OD | Similar to doxazosin |
5-Alpha-Reductase Inhibitors (5-ARIs) - For large prostates
| Drug | Dose | Notes |
|---|---|---|
| Finasteride | 5 mg OD | Blocks type 2 5-AR |
| Dutasteride | 0.5 mg OD | Blocks both type 1 and type 2; preferred per current evidence |
Benefits beyond symptoms: Reduce acute urinary retention by ~57%, reduce need for surgery by ~50%
Side effects: Erectile dysfunction, reduced libido, decreased ejaculate volume, gynaecomastia
Important: Reduces PSA by ~50% after 6-12 months; must double the PSA reading to interpret correctly
Combination Therapy (Alpha-blocker + 5-ARI)
- Dutasteride + Tamsulosin (or their combination pill) is the best-evidence combination
- Indicated for men with moderate-severe symptoms AND prostate volume >30-40 mL
- More effective than either drug alone for symptom relief and reducing disease progression
- The alpha-blocker handles the immediate dynamic component; 5-ARI shrinks the prostate over months
Phosphodiesterase-5 Inhibitors (PDE5i)
- Tadalafil 5 mg daily - improves LUTS and IPSS; also treats concomitant erectile dysfunction (very useful in BPH patients)
- Less effective than alpha-blockers for improving flow rates
- Can be combined with alpha-blocker
Antimuscarinics / Beta-3 Agonists - For dominant storage symptoms
- Antimuscarinics: Solifenacin 5-10 mg, Tolterodine, Oxybutynin, Fesoterodine
- Beta-3 agonists: Mirabegron 25-50 mg, Vibegron 75 mg
- Caution: Use with care if PVR >200 mL (risk of precipitating acute retention)
- Can be added to tamsulosin in inadequate responders
Step 4 - Surgical Indications
Absolute / Strong Indications (must operate):
- Acute urinary retention (refractory to trial without catheter, or recurrent)
- Chronic retention with renal impairment - PVR ≥200 mL + hydronephrosis + abnormal creatinine
- Recurrent UTIs secondary to significant PVR
- Bladder stones secondary to BOO
- Recurrent haematuria from vascular BPH not responding to 5-ARI
Elective Indications:
- Severe symptoms (IPSS ≥20) not responding to medications
- Q-max <10 mL/s + PVR 100-250 mL
- Patient preference after failed/refused medical therapy
Surgical Options:
| Procedure | Prostate Size | Notes |
|---|---|---|
| TURP (Transurethral Resection of Prostate) | 30-80 g | Gold standard endoscopic treatment; monopolar or bipolar; bipolar safer (uses saline, avoids TUR syndrome, less transfusion) |
| Holmium Laser Enucleation (HoLEP) | Any size | Gold standard for large prostates; size-independent; less bleeding; same efficacy as open prostatectomy |
| GreenLight PVP (Photoselective Vaporisation) | <80 g | Laser vaporisation; good for anticoagulated patients; less inpatient time |
| Open simple prostatectomy | >80-100 g | Millin's (retropubic) or Freyer's (suprapubic); for very large glands if endoscopic not feasible |
| Robotic/Laparoscopic simple prostatectomy | >80 g | Minimally invasive alternative to open |
| Prostatic Urethral Lift (Urolift) | <80 g, no middle lobe | Preserves ejaculation; transprostatic implants via cystoscope; good for sexually active men |
| Rezum (water vapour therapy) | Convective water vapour | Office-based; delayed coagulation necrosis; preserves ejaculation |
| Prostatic artery embolisation (PAE) | Any | Interventional radiology; evidence still evolving; alternative for high-surgical-risk patients |
9. COMPLICATIONS OF UNTREATED BPH
| Complication | Mechanism |
|---|---|
| Acute urinary retention | Acute decompensation |
| High-pressure chronic retention | PVR >250 mL, elevated bladder pressure → bilateral hydronephrosis, renal failure |
| Recurrent UTIs | Static urine = bacterial culture medium |
| Bladder stones | Urinary stasis |
| Bladder diverticula | Trabeculation from detrusor hypertrophy |
| Detrusor decompensation | Irreversible storage symptoms even after prostatectomy |
| Haematuria | Dilated veins over prostate |
10. FOLLOW-UP PLAN
- At 3 months after starting medical therapy: reassess IPSS, QoL, uroflowmetry, PVR
- PSA recheck at 6-12 months on 5-ARI (expect 50% reduction; if not, suspect cancer)
- Annual review if stable on medical therapy
- Patient education about: drug side effects, timeline of response, signs requiring urgent review (acute retention, worsening renal function, haematuria)
Quick Reference Summary
BPH/LUTS Patient → History (IPSS, voiding diary) → Examination (abdomen, DRE, neurology)
→ Investigations (UA, creatinine, uroflowmetry + PVR, PSA, USS)
→ Exclude: Ca prostate, stricture, bladder Ca, neurogenic, OAB
IPSS 0-7 → Watchful waiting + lifestyle
IPSS 8-19 → Alpha-blocker ± 5-ARI (if prostate >30-40 mL or PSA >1.5)
IPSS ≥20 → Medical therapy; surgery if refractory
Absolute surgical indications → Retention, renal impairment, recurrent UTI/stones, bleeding
- Goldman-Cecil Medicine, Ch. 114 - Benign Prostatic Hyperplasia, pp. 1316-1322
- Bailey and Love's Short Practice of Surgery (28th ed.), Ch. 84 - BPH, pp. 1543-1548
- Campbell-Walsh-Wein Urology (12th ed.) - BPH chapters
Teach me TURP and make me able to defend every question of examiner
"transurethral resection" AND "prostate" AND outcomes
TURP - Complete Exam-Ready Guide for Urology Residents
1. DEFINITION & CONTEXT
Examiner question: "Why is TURP called the gold standard?" Answer: It has the longest evidence base, most validated outcomes data, best improvement in urinary flow rates and symptom scores, and all newer procedures compare themselves to TURP in trials.
2. ANATOMY CRITICAL TO THE PROCEDURE
| Structure | Relevance to TURP |
|---|---|
| Transitional zone | Site of BPH; tissue to be resected |
| Verumontanum (seminal colliculus) | Distal landmark - never resect distal to it - doing so causes incontinence by damaging the external urethral sphincter |
| External urethral sphincter | Just distal to verumontanum; injury = permanent incontinence |
| Bladder neck | Proximal landmark; resection extends up to but should preserve it |
| Prostatic capsule | Boundary of resection; perforation = capsular breach = risk of fluid absorption and TUR syndrome |
| Surgical capsule | Formed by compressed peripheral zone - the plane of resection; appears as whitish/yellowish fatty fibrous tissue |
| Ejaculatory ducts | Enter at verumontanum; injury = retrograde ejaculation |
| Periprostatic venous plexus (Santorini's plexus) | Breached venous sinuses = entry route for irrigating fluid into circulation |
3. INDICATIONS FOR TURP
Absolute / Strong Indications (must not delay):
- Acute urinary retention - failed trial without catheter (TWOC), or recurrent AUR
- Chronic retention with upper tract obstruction - bilateral hydronephrosis + renal impairment
- Recurrent UTIs due to significant post-void residual (PVR)
- Bladder stones secondary to bladder outlet obstruction
- Recurrent haematuria from BPH unresponsive to 5-ARI therapy
Elective Indications:
- IPSS ≥ 20 with failed/refused medical therapy
- Moderate symptoms (IPSS 8-19) with significant bother after medical failure
- Q-max < 10 mL/s + PVR 100-250 mL
- Patient preference after weighing alternatives
Prostate Size Consideration:
- TURP is ideal for 30-80 g prostates
- For > 80-100 g: consider HoLEP or open/robotic simple prostatectomy
- Very small gland with BOO: consider TUIP (transurethral incision of prostate) instead
Examiner question: "What is the size limit for TURP?" Answer: Conventionally 80 g. Beyond this, resection time increases disproportionately (>1 hour), increasing risk of fluid absorption and TUR syndrome. HoLEP has no size restriction.
4. CONTRAINDICATIONS
Absolute:
- Untreated UTI (risk of bacteraemia/sepsis from irrigant entering venous sinuses)
- Uncorrected coagulopathy
- Urethral stricture preventing passage of resectoscope (treat stricture first)
- Patient unfit for anaesthesia
Relative:
- Prostate > 80-100 g (increased surgical risk)
- Small bladder capacity (risk of perforation)
- Prior pelvic surgery/radiation (anatomy distorted)
- Desire to preserve antegrade ejaculation (counsel about retrograde ejaculation; consider alternatives like Urolift)
5. PRE-OPERATIVE WORKUP
History:
- IPSS score and QoL score
- Sexual function (SHIM questionnaire) - baseline for post-op comparison
- Medications: anticoagulants/antiplatelets (must stop: aspirin 7 days, clopidogrel 5-7 days, warfarin 5 days - bridge with LMWH if high-risk cardiac/AF patient)
- Diabetes (affects healing, infection risk)
Examination:
- DRE - prostate size, consistency (exclude cancer)
- Abdominal exam - palpable bladder
- Focused neurology
Investigations:
| Investigation | Rationale |
|---|---|
| Urine culture (MSU) | Must be sterile before surgery; treat any infection first |
| Serum creatinine + electrolytes | Baseline renal function; hydronephrosis? |
| Full blood count | Baseline haemoglobin; anaemia correction pre-op |
| Coagulation screen (PT/INR/APTT) | Detect coagulopathy |
| PSA | Pre-op baseline; if elevated, consider biopsy to exclude cancer before TURP |
| Uroflowmetry + PVR | Baseline for outcome comparison |
| Prostate volume (USS/TRUS) | Confirm size suitable for TURP |
| Cystoscopy (flexible, prior to OR) | Exclude urethral stricture, bladder neck stenosis, bladder tumour, vesical calculi, assess middle lobe |
| ECG + chest X-ray | Anaesthetic assessment, particularly in elderly patients |
| Group and save | Risk of intraoperative bleeding |
Consent - what to tell the patient (must be comprehensive):
- Retrograde ejaculation (~65-90% of patients)
- Erectile dysfunction (~5-10%)
- Urinary incontinence (temporary stress incontinence ~5%; permanent <1%)
- Urethral/bladder neck stricture (2-4%)
- Bleeding requiring transfusion (~2%)
- TUR syndrome (<1% with bipolar, ~2% with monopolar)
- Risk of re-operation (10-15% at 10 years)
- Continued irritative LUTS post-op (may persist 4-6 weeks)
- Failure to void after catheter removal (~5%)
6. ANAESTHESIA
-
Spinal/regional anaesthesia (preferred) - advantages:
- Patient remains conscious - allows early detection of TUR syndrome (confusion, restlessness are first signs; awake patient communicates symptoms)
- Lower risk of deep venous thrombosis (sympathetic block causes vasodilation)
- Equivalent outcomes to GA
- Block level needed: T10 (level of bladder sensation)
-
General anaesthesia - used when:
- Patient refuses spinal
- Contraindication to spinal (coagulopathy, spinal pathology, patient refusal)
- Anticipated long procedure
- Disadvantage: masks early TUR syndrome signs
Examiner question: "Why is spinal anaesthesia preferred for TURP?" Answer: The conscious patient can report early symptoms of TUR syndrome (confusion, nausea, visual disturbance) before they become severe. Under GA, TUR syndrome may only be detected when cardiovascular or respiratory signs appear, by which time it is more advanced.
7. PATIENT POSITIONING
- Lithotomy position - legs in stirrups
- Pressure areas: protect heels, common peroneal nerve at fibular head, popliteal fossa
- Compartment syndrome of the legs (from prolonged lithotomy) - change stirrup position if >2 hours
- Brachial plexus injury (if arms extended)
- DVT prophylaxis: TED stockings, pneumatic compression devices
8. INSTRUMENTS - KNOW EVERY COMPONENT
| Component | Function |
|---|---|
| Outer sheath | Conducts irrigation inflow and outflow; sizes 24-28 Fr are common |
| Inner sheath | Houses the working element |
| Working element | Holds the electrode and connects to diathermy machine |
| Cutting loop (electrode) | Wire loop through which current flows to cut and coagulate tissue |
| Telescope (lens) | 0° for initial survey; 30° for lateral lobes; 70° for bladder inspection |
| Light source cable | Provides illumination |
- Cutting current: High-frequency alternating current causes vaporisation (tissue cutting)
- Coagulation current: Lower frequency; coagulates bleeding vessels without cutting
| Feature | Monopolar TURP (M-TURP) | Bipolar TURP (B-TURP) |
|---|---|---|
| Irrigant | Non-electrolyte (1.5% glycine, sorbitol) | Normal saline (0.9% NaCl) |
| Current path | Active electrode → patient's body → return pad | Active electrode → tissue → return electrode (within resectoscope) |
| TUR syndrome risk | Yes (hypotonic irrigant absorbed) | No (isotonic saline; only volume overload possible) |
| Hyponatremia | Yes | No |
| Diathermy burns from return pad | Possible | No |
| Tissue resection quality | Excellent | Equivalent |
| Cost | Lower | Higher |
Examiner question: "Why can't you use saline with monopolar TURP?" Answer: Saline (NaCl) is an electrolyte conductor. In monopolar diathermy, current must travel from the active electrode through tissue to a return/ground pad. Saline would conduct and disperse the current throughout the irrigating fluid rather than concentrating it at the cutting loop - the loop would not generate enough current density to cut tissue. Bipolar diathermy completes the circuit locally between two electrodes within the resectoscope, so saline works fine.
9. IRRIGATING SOLUTIONS - CRITICAL TOPIC
| Solution | Osmolality (mOsm/L) | Advantages | Disadvantages |
|---|---|---|---|
| 1.5% Glycine | 200 (hypotonic) | Best visibility, standard for monopolar | TUR syndrome; hyperammonemia; transient blindness (glycine is GABA-like inhibitory neurotransmitter in retina); hyperoxaluria |
| 3.3% Sorbitol | 165 (hypotonic) | Less expensive | Hyperglycemia, lactic acidosis, osmotic diuresis |
| 5% Mannitol | 275 (near-isotonic) | Isosmolar, not metabolized, acts as osmotic diuretic | Volume expansion, osmotic diuresis |
| Distilled water | 0 | Excellent visibility | Severe hemolysis, hemoglobinemia, hemoglobinuria, acute renal failure - rarely used now |
| 0.9% Normal Saline | 308 (isotonic) | No hyponatremia, no metabolic side effects | Only usable with bipolar or laser |
10. SURGICAL TECHNIQUE - STEP BY STEP
- Insert 0° telescope through urethra and into bladder
- Inspect urethra for stricture
- Inspect bladder: exclude tumour, stones, diverticula; note ureteric orifices (landmarks)
- Inspect prostate: size, lobe configuration (note middle lobe, lateral lobe enlargement), bladder neck
- Lubricate generously
- Advance resectoscope sheath under vision
- Note verumontanum position (your critical distal landmark)
- Start at 6 o'clock position - create a groove down to the capsule (establishes landmark for depth)
- Proceed to 5 o'clock and 7 o'clock grooves
- Resect lateral lobes (systematic sweeping movements from bladder neck to verumontanum)
- Resect median/middle lobe last (resecting middle lobe first collapses the field and reduces visibility)
- Working within the surgical capsule (whitish, circular fibres) at all times
- Systematically coagulate visible bleeding points
- Reduce irrigation pressure to identify low-pressure bleeders
- Check for arterial bleeders (bright red spurting) - coagulate these immediately
- Check at the end of procedure with reduced irrigation flow to ensure haemostasis
- Resected chips (tissue fragments) are evacuated with an Ellik evacuator (bulb syringe that creates turbulence in the bladder to suction out chips)
- Send all chips for histopathology (unsuspected prostate cancer found in 8-10% of TURP specimens)
- Three-way 22Fr Foley catheter
- Continuous bladder irrigation (CBI) started with normal saline to wash out blood and prevent clot retention
- Catheter removed typically at 24-48 hours post-op (earlier if urine clears)
Examiner question: "Why do you send all TURP chips for histopathology?" Answer: Incidental prostate cancer (pT2 disease) is found in approximately 8-10% of TURP specimens. This has therapeutic implications - if significant cancer is found, the patient needs staging and potentially radical treatment.
11. TUR SYNDROME - THE MOST FEARED COMPLICATION
Definition:
Mechanism of Fluid Entry:
- Open prostatic venous sinuses (primary route) - the periprostatic venous plexus becomes exposed during resection
- Capsular perforation (extravasation into retroperitoneum, then absorbed)
- Bladder perforation into peritoneal space (rarer)
Factors Increasing Risk:
- Prolonged resection (>60 min is critical threshold)
- Large prostate with extensive venous sinus exposure
- High irrigation fluid pressure (height of bag)
- Capsular perforation
- Low venous pressure at irrigation-blood interface (hypotension)
- Large prostate volume resected
Clinical Features by Serum Na+ Level:
| Serum Na+ (mEq/L) | CNS Features | Cardiovascular Features |
|---|---|---|
| 120 | Confusion, restlessness, headache | Mild hypertension |
| 115 | Somnolence, nausea, visual disturbance | Widened QRS, elevated ST |
| 110 | Seizures, coma | Ventricular tachycardia/fibrillation |
- Nausea, vomiting
- Restlessness, confusion
- Visual disturbance (blurred vision, transient blindness - specific to glycine)
- Headache
- Hypertension (early, from volume loading)
- Hypotension
- Bradycardia
- Pulmonary oedema (dyspnoea)
- Cardiovascular collapse
Additional Glycine-Specific Toxicity:
- Transient blindness - glycine structurally similar to inhibitory neurotransmitter GABA → retinal/brainstem inhibition. Pupils minimally reactive. NOT cerebral oedema.
- Hyperammonemia - glycine metabolised to ammonia → encephalopathy, coma lasting 24-48 hours post-op
Treatment of TUR Syndrome:
- Stop surgery immediately - abandon procedure, insert catheter
- Call anaesthesiologist urgently
- Furosemide IV (40-80 mg) - promote water diuresis
- Restrict fluids - stop any hypotonic IV fluids
- Serum electrolytes urgently - check Na+ level
- Oxygen via face mask / consider intubation if severe
- Hypertonic saline (3% NaCl) infusion - ONLY if:
- Na+ < 120 mEq/L, OR
- Symptomatic severe hyponatremia (seizures)
- Rate of correction: max 1-2 mEq/L/hour; target: raise Na+ to 120 mEq/L then allow slow correction
- Never correct faster than 8-10 mEq/L in 24 hours - risk of osmotic demyelination syndrome (central pontine myelinolysis)
- ITU/HDU monitoring if severe
Examiner question: "How do you prevent TUR syndrome?" Answer: (a) Use bipolar TURP with saline - eliminates hyponatremia risk; (b) Limit resection time to <60 minutes; (c) Keep irrigation bag height low (minimise hydrostatic pressure); (d) Achieve rapid haemostasis; (e) Avoid capsular perforation; (f) Use spinal anaesthesia so patient can report early symptoms; (g) Monitor for early signs and stop promptly.
Examiner question: "Why does glycine cause visual disturbance but not cerebral oedema?" Answer: Glycine is structurally similar to inhibitory neurotransmitters (GABA, glycine receptors in the retina and brainstem). It inhibits neurotransmission in the retina and optic pathway causing transient blindness and minimally reactive pupils. This reverses as glycine is metabolised. Cerebral oedema would cause raised ICP with papilloedema and slower onset - that is not the mechanism here.
12. ALL COMPLICATIONS OF TURP - CLASSIFIED
Intraoperative:
| Complication | Incidence | Notes |
|---|---|---|
| Haemorrhage | ~2% need transfusion | Controlled with coagulation; if uncontrolled, pack and insert Foley, inflate balloon at bladder neck |
| Capsular perforation | ~1-2% | Minor = prolonged catheterisation; major = convert to open; increases TUR syndrome risk |
| Bladder perforation | Rare | Distended bladder + aggressive resection; extraperitoneal = conservative; intraperitoneal = laparotomy |
| TUR syndrome | <1% bipolar, ~1.4% monopolar | Described in detail above |
| Damage to ureteric orifice | Rare | Middle lobe resection too aggressive |
Immediate Post-operative (within 24-48 hours):
| Complication | Management |
|---|---|
| Clot retention | Bladder irrigation ± manual evacuation with Ellik evacuator; rarely return to OR |
| Failure to void (after catheter removal) | Clean intermittent self-catheterisation (CISC); re-catheterise; assess for detrusor underactivity |
| UTI / Urosepsis | Cultures + antibiotics; may require IV antibiotics + resuscitation (can be life-threatening) |
Early Post-operative (first few weeks):
| Complication | Incidence | Notes |
|---|---|---|
| Haematuria | Common | Usually settles; significant haematuria → return to OR for clot evacuation + haemostasis |
| Dysuria / Irritative LUTS | Very common | Normal healing response; resolves over 4-6 weeks |
| Secondary haemorrhage | ~2% at 10-14 days | Sloughing of necrotic prostatic tissue/eschar; treat with catheterisation and CBI |
Late Complications:
| Complication | Incidence | Notes |
|---|---|---|
| Retrograde ejaculation | 65-90% | Most common sexual side effect; semen goes into bladder instead of out; must be counselled pre-op; causes infertility (can collect urine post-orgasm for sperm retrieval) |
| Erectile dysfunction | ~5-10% | Less than open prostatectomy; likely pre-existing vascular disease in this age group |
| Urethral stricture | ~2-4% | From resectoscope trauma, particularly at meatus or bulbar urethra; treat with urethral dilation or optical urethrotomy |
| Bladder neck contracture | ~2-3% | Fibrosis of bladder neck post-TURP; presents with recurrent LUTS; treat with endoscopic incision of bladder neck |
| Stress urinary incontinence | <1% permanent | External sphincter damage; must counsel; temporary incontinence in ~5% resolves in weeks |
| Re-operation | ~10-15% at 10 years | Most common reason: regrowth of BPH; some cases: bladder neck contracture, stricture |
| Urge incontinence | Common temporarily | Pre-existing detrusor overactivity may persist; treat with antimuscarinics |
Examiner question: "What is the most common complication of TURP?" Answer: Retrograde ejaculation, occurring in 65-90% of patients. It must be specifically discussed in pre-operative counselling.
Examiner question: "A patient returns at 12 days post-TURP with haematuria. What is happening and how do you manage?" Answer: This is secondary haemorrhage due to sloughing of the post-TURP necrotic eschar (similar to a post-tonsillectomy bleed). Management: (1) admit patient; (2) catheterise and start CBI; (3) cross-match blood; (4) most cases settle with irrigation; (5) if haemorrhage continues or bladder fills with clots despite irrigation, return to theatre for cystoscopy, clot evacuation, and formal coagulation.
13. MONOPOLAR vs BIPOLAR TURP - EXAM FAVOURITE
| Parameter | M-TURP | B-TURP |
|---|---|---|
| Irrigant | Glycine 1.5% (non-electrolyte) | Normal saline 0.9% |
| TUR syndrome | Yes (hyponatraemia + volume overload) | Only volume overload possible |
| Serum Na+ change | Decreases | Minimal change |
| Blood loss | Similar | Similar or slightly less |
| Catheter duration | Similar | Similar |
| Tissue quality | Reference standard | Equivalent |
| IPSS improvement | Equivalent | Equivalent |
| Operative time | Similar | Similar |
| Cost | Lower | Higher |
| Evidence level | Decades of data | Growing, now comparable |
| Current recommendation | Being replaced by bipolar | Increasingly preferred |
Examiner question: "What is the advantage of bipolar TURP?" Answer: Normal saline is used as irrigant. Since saline is isotonic, any absorbed fluid causes only volume overload - not dilutional hyponatraemia. This eliminates the metabolic component of TUR syndrome (the hyponatremia, glycine toxicity, hyperammonemia) while only the haemodynamic overload risk remains. Bipolar also eliminates the risk of diathermy burns at the return electrode pad site.
14. OUTCOMES OF TURP
- IPSS improvement: 70-80% reduction in symptom score
- Peak flow rate (Q-max) improvement: Increases by 100-150% (e.g., from 8 mL/s to 16-20 mL/s)
- PVR reduction: Significant
- Patient satisfaction: >80% satisfied
- Re-operation rate: ~10-15% at 10 years (main reason: BPH regrowth, bladder neck contracture)
- Mortality: <0.1% in modern series (historically 0.5-1%)
- Blood transfusion rate: ~2% in modern series
15. POST-OPERATIVE CARE
- CBI with normal saline via 3-way Foley until urine runs clear (usually 12-24 hours)
- Analgesia: NSAIDs (avoid if renal impairment) + paracetamol
- Monitor: urine output, colour, haemoglobin, electrolytes (especially Na+)
- Mobilise early - DVT risk
- Remove catheter at 24-48 hours (when urine clear); ensure adequate void and check PVR
- Discharge home same day or next day in uncomplicated cases
- Avoid strenuous activity for 2-4 weeks
- Avoid sexual intercourse for 4-6 weeks
- Increased fluid intake (dilutes urine, reduces clot risk)
- Expect mild haematuria, frequency, dysuria - normal for 4-6 weeks
- Return immediately if: heavy haematuria, clot retention, fever, inability to void
- Stop anticoagulants can be restarted at 24-48 hours (liaise with haematology for high-risk patients)
- Alpha-blockers: can be stopped post-TURP (obstruction relieved)
- 5-ARIs: stop post-TURP
16. TURP vs ALTERNATIVES - EXAMINER LOVES THIS
| Procedure | Prostate Size | Pros vs TURP | Cons vs TURP |
|---|---|---|---|
| HoLEP | Any size | No size limit; less bleeding; catheter time shorter; same efficacy | Steep learning curve; equipment cost; not widely available |
| GreenLight PVP | <80 g | Outpatient; good for anticoagulated patients; haemostatic | Chips not available for histology; may need re-treatment |
| Open prostatectomy | >80-100 g | Removes large glands completely | Higher morbidity, blood loss, hospital stay; scar |
| Urolift | <80 g, no middle lobe | Preserves ejaculation; day case; no retrograde ejaculation | Lower efficacy; re-treatment rate higher; implants inserted |
| Rezum (water vapour) | Any | Preserves ejaculation; office-based | Delayed response; needs catheter post-op; limited evidence vs TURP |
| TUIP | <30 g, narrow bladder neck | Faster; lower retrograde ejaculation rate; less bleeding | Only suitable for small glands; higher re-operation rate |
| PAE | Any | Interventional radiology; no general anaesthesia; suitable for high-risk patients | Inferior symptom scores vs TURP; post-PAE syndrome; evidence still evolving |
17. QUICK VIVA FIRE-ROUND - Q&A
SUMMARY CARD
TURP = Gold standard endoscopic BPH surgery
Ideal prostate size: 30-80 g
Position: Lithotomy | Anaesthesia: Spinal preferred (detect TUR syndrome early)
Irrigant: Glycine (monopolar) | Saline (bipolar - preferred)
Key landmark: VERUMONTANUM - never resect distal to it
Resection sequence: 6 o'clock groove → lateral lobes → median lobe last
Chip evacuation: Ellik evacuator | Send ALL chips to histology
Post-op: 3-way Foley + CBI until clear → remove 24-48h
MOST COMMON complication: Retrograde ejaculation (65-90%)
MOST FEARED complication: TUR syndrome → hyponatremia → confusion → seizures → VF
Treatment of TUR syndrome: STOP surgery → furosemide → restrict fluids → hypertonic saline if Na <120
Bipolar advantage: Uses saline → no hyponatraemia TUR syndrome
Re-operation rate: ~10-15% at 10 years
What are the techniques of TURP like nesbit mauemayer etc
Nesbit Mauermayer TURP technique differences transurethral resection prostate methods
https://emedicine.medscape.com/article/449781-overview
https://emedicine.medscape.com/article/449781-overview
Barnes Flocks TURP technique transurethral resection prostate methods comparison
Techniques of TURP - Complete Guide
"The actual technique is probably not as important as planning it carefully and executing it precisely so that the operation is complete and the surgeon remains oriented throughout the procedure."
THE THREE UNIVERSAL STAGES IN ALL TECHNIQUES
| Stage | What Happens |
|---|---|
| 1. Establishing landmarks | Identify verumontanum, bladder neck, ureteric orifices, surgical capsule |
| 2. Removing the main bulk | Systematic resection of adenoma (order varies by technique) |
| 3. Tidying up (apical resection) | Remove residual apical tissue around verumontanum; achieve haemostasis |
THE PRINCIPAL TECHNIQUES
1. NESBIT TECHNIQUE (1943/1951) - The Classic Standard
Nesbit's Three Formal Stages:
- Resectoscope positioned at the midpoint of the prostate
- Begin at the 12 o'clock position (anterior, roof of prostate)
- Resect intravesical prostatic tissue, bladder neck, and immediately adjacent proximal prostatic tissue
- Work clockwise from 12 → 3 → 6 → 9 → 12
- This stage removes the anterior (ventral) portions and the proximal adenoma
- Key effect: early control of perforating urethral blood vessels at the roof, devascularising the lateral lobes
- Systematic resection of lateral lobes (3-9 o'clock on each side)
- Because the anterior and proximal tissue was removed in Stage 1, the lateral lobe bulk falls posteriorly under gravity
- This makes the posterior and posterolateral tissue easier to visualise and resect
- Proceed from 12 o'clock down to 6 o'clock on each side
- Resect to the surgical capsule (circular white fibrous tissue - the plane boundary)
- Most critical and delicate stage
- Remove remaining apical tissue around the verumontanum
- Again start at 12 o'clock anteriorly, using the verumontanum as the primary landmark
- Short, controlled strokes to avoid going beyond/distal to verumontanum
- A finger in the rectum (by assistant) can help feel the extent of remaining apex tissue
12 o'clock proximal → clockwise proximal resection → lateral lobes fall back
→ systematic lateral lobe resection → apical resection around verumontanum
- Early devascularisation (roof cut first controls main vessels → less bleeding overall)
- Lateral lobes released and fall posteriorly → easier to resect bulky tissue
- Surgeon always oriented by the intact capsule landmarks
- Widely taught; most urologists trained on this
- Bulk lateral lobe tissue may impede view during capsular bleeding control until removed
- Partially resected lateral lobes (inevitable mid-procedure) tend to bleed
2. MAUERMAYER TECHNIQUE (1985)
Sequence:
- Resect the middle lobe (if present) at the prostatic floor
- Create a channel between 5 and 7 o'clock at the floor of the prostatic urethra
- This opens up the bladder neck drainage, improves irrigation flow and visual clarity immediately
- With good irrigation now established (floor open), resect lateral lobes systematically
- Proceed from floor upward, resecting ventral (anterior) portions as well
- Careful apical resection around verumontanum
Middle lobe (5-7 o'clock channel) → lateral lobes + ventral parts → apical region
- Immediate improvement in irrigation drainage (floor opened first)
- Excellent early visibility
- Particularly suited when there is a prominent middle/median lobe obstructing the bladder neck (the most bothersome obstruction is relieved first)
- If middle lobe is intravesical, removing it first prevents it from flopping over the bladder neck and obstructing vision
- Starting at 6 o'clock without devascularising the roof first → can encounter more bleeding from lateral lobe vessels early on
- Less systematic devascularisation compared to Nesbit
3. MILNER TECHNIQUE (1941)
Sequence:
- If median lobe enlarged, resect it first to open the bladder neck and clear the field
- Begin with a deep full-length groove at the extreme lateral position (9 o'clock for the left lobe, or 3 o'clock for right lobe)
- The groove goes from bladder neck to verumontanum level, full depth to capsule
- This groove runs the entire length of the prostate at the thickest lateral point
- Then systematically resect the entire lobe in sequence - anterior portions first, allowing remaining tissue to fall posteriorly
- Complete the entire lobe before moving on
- Mirror the procedure on the opposite side
- Again, full-length groove first, then systematic completion
- Resected similarly to Nesbit technique
- Dr. Milner used the Stern-McCarthy resectoscope (2-handed instrument) so he could not place a finger in the rectum - he relied on resecting the posterior lobe to a slightly concave surface
- Tissue around verumontanum is resected carefully
- Scope is inverted; remaining tissue 11-1 o'clock resected with straight strokes parallel/proximal to verumontanum
Middle lobe (if present) → full-length groove at 9 or 3 o'clock → complete one entire lateral lobe
→ full-length groove opposite side → complete second lateral lobe → posterior lobe → apex
- Immediate attack on the bulk lateral lobe tissue → faster tissue removal, better irrigation and scope mobility early
- One-lobe-at-a-time approach: can stop surgery midway (after one lobe) if needed (bleeding, time limit, TUR syndrome developing) - the completed side is already fully haemostatic
- Full-length groove at thickest point (9 or 3) means any inadvertent early capsular perforation occurs at minimal clinical risk (thickest point of capsule)
- Less bleeding in practice because perpendicular resection to capsule gives rapid access to main vessels for immediate coagulation
- Avoids problem of bulk lateral lobe tissue impeding vision
- Appears to "violate" Nesbit devascularisation principle (no early 12 o'clock cut)
- Requires skill - the speed of resection is key to controlling bleeding
- Steeper learning curve to master
4. BARNES TECHNIQUE
Sequence:
- Begin resection at the posterior lobe (6 o'clock)
- This immediately establishes good irrigation flow into the bladder (floor open)
- Ensures thorough posterior lobe resection (which can be difficult later when floor fills with chips and clots)
- Then proceed to lateral lobes and ventral portions
- Apex last
5. ALCOCK TECHNIQUE
Sequence:
- Resect along the floor and sides to undermine the base of each lateral lobe
- The undermined lateral lobes then fall into the prostatic fossa
- Resect the fallen lobe tissue
- Works on principle of gravity-assisted prolapse of tissue into the field
6. FLOCKS TECHNIQUE
- Creates a posterior sulcus first, exposing the capsule posterolaterally
- Proceeds to remove lateral lobe tissue working anteriorly
- Establishes posterior capsule landmark early
COMPARISON TABLE - AT A GLANCE
| Technique | Where to Start | Order of Resection | Best For | Eponymous Advantage |
|---|---|---|---|---|
| Nesbit | 12 o'clock (anterior/roof) | Anterior → lateral lobes fall back → apex | Standard; any size prostate | Early devascularisation; gravity assists |
| Mauermayer | 5-7 o'clock (floor/middle lobe) | Middle lobe → side lobes → ventral → apex | Prominent middle lobe; improves irrigation early | Immediate drainage; best for middle lobe |
| Milner | 9 or 3 o'clock (extreme lateral) | One complete lobe at a time → second lobe → posterior → apex | Large lateral lobes; ability to stop early | Complete one-lobe-at-a-time; stop midway safely |
| Barnes | Posterior lobe (6 o'clock) | Posterior → lateral → ventral → apex | Larger prostates | Posterior lobe secured early; good irrigation |
| Alcock | Undermine lateral base | Undermining → fall → resect | Large heavy lateral lobes only | Gravity-assisted prolapse of lobe |
| Flocks | Posterior lateral sulcus | Posterolateral groove → lateral → anterior → apex | Systematic capsule identification | Early posterior capsule landmark |
UNIVERSAL PRINCIPLES APPLYING TO ALL TECHNIQUES
- Cystoscopy first - inspect urethra, bladder, note ureteric orifices, assess prostate configuration
- Verumontanum = absolute distal boundary - never resect distal to it
- Ureteric orifices - identify and protect during bladder neck/middle lobe resection
- Surgical capsule = endpoint of resection (circular white fibrous tissue)
- Haemostasis at each stage - do not leave active bleeders and proceed
- Resection time ≤60 minutes - if not complete, stage the procedure
- Ellik evacuator for chip clearance before each new stage (improves visibility)
- Systematic approach - always have a plan; disorientation is the surgeon's greatest enemy
APICAL RESECTION - SPECIAL MENTION
- It is the most critical step for functional success - inadequate apex resection = persistent obstruction
- It is the most dangerous step - external sphincter lies just distal to verumontanum
- Resect with short controlled strokes at the apex
- Use verumontanum as constant reference - the loop should never go distal to its distal edge
- The scope can be inverted (rolled) to reach the anterior apex (11-1 o'clock tissue above the verumontanum) using short straight strokes parallel to the veru
- Rectal finger by assistant: the finger can guide depth of remaining tissue at the apex
- Some urologists use the cold-cut technique (cut current only, no coagulation) for the very last apical tissue to avoid thermal spread to the sphincter
EXAMINER Q&A ON TECHNIQUES
Give me table of this technique with pros and cons and also tell me about blandy technique
Blandy TURP technique transurethral resection prostate steps method
Blandy TURP technique "6 o'clock" "12 o'clock" prostate resection sequence British urology
https://emedicine.medscape.com/article/449781-overview
https://www.baus.org.uk/_userfiles/pages/files/Museum/Transu…
"Blandy technique" TURP "6 o'clock" groove prostate resection sequence hemostasis
TURP Techniques - Complete Table + Blandy Technique in Detail
WHO WAS JOHN BLANDY?
THE BLANDY TECHNIQUE - Full Detail
BLANDY'S THREE UNIVERSAL STAGES (applies to his whole technique)
"In all methods there are three stages: 1. Establishing the landmarks. 2. Removing the main bulk of tissue. 3. Tidying up." - Blandy
STAGE 1: ESTABLISHING LANDMARKS
- Ureteric orifices (bilateral) - must be visualised and protected throughout
- Verumontanum - the sacred distal landmark; never cut distal to it
- Bladder neck - proximal limit
- Anterior commissure (12 o'clock) - reference for orientation
- Surgical capsule - circular fibres; endpoint of resection
STAGE 2: REMOVING THE MAIN BULK
STEP 1 - Resect the Middle Lobe First
- The middle/median lobe is resected first (if present)
- Take systematic, even cuts to reduce the mound of the middle lobe flat
- The correctly resected middle lobe shows a "cobweb appearance" under the bladder neck - this is the endpoint
- After resecting the middle lobe, specifically control Badenoch's arteries at 5 and 7 o'clock (these are the main arterial feeders to the floor of the prostate at the bladder neck level - named after A.J. Badenoch, a British urologist)
STEP 2 - First Method for Lateral Lobes (standard-sized prostate)
- Rotate resectoscope to bring the anterior commissure to 12 o'clock
- Take one or two careful chips at 1 o'clock - the object is to liberate the lateral lobe from the capsule anteriorly
- Remember: the prostate is very thin anteriorly at 12 o'clock - only 1-2 chips expose the capsule here
- Deepen the trench laterally - as you proceed, the left lateral lobe falls backwards into the space vacated by the resected middle lobe (gravity-assisted)
- At this point you will encounter the "arteries of Flocks" at 2 o'clock (Rubin Flocks first described the arterial anatomy of the prostate in 1937 - the main arterial supply enters at the 2 and 10 o'clock positions at the bladder neck). These must be carefully coagulated before proceeding further
- Once the lateral lobe has fallen inwards, resect the fallen lump of tissue - it is now free of the capsule and easier to remove
- Repeat mirror procedure on the opposite side
- For a really bulky prostate, begin with prophylactic coagulation of the main prostatic arteries at 10, 2, 5 and 7 o'clock using the rollerball electrode before taking any tissue
- This pre-emptive devascularisation reduces bleeding during the subsequent bulk resection
- Then proceed to resect middle lobe, followed by lateral lobes as above
STAGE 3: TIDYING UP (THE APICAL RESECTION)
- The apical tissue at 2 and 10 o'clock (anterolateral apex) is trimmed carefully
- A finger in the rectum by the assistant can lift the apical tissue up toward the resectoscope loop - making it easier to resect without going distal to the verumontanum
- Trim the tissue adjacent to the verumontanum with great care
"In removing the tissue adjacent to the verumontanum, err on the side of caution. A gram or two of adenoma in this situation does not cause outflow obstruction, and a damaged sphincter can never be restored."
KEY BLANDY ANATOMICAL FEATURES TO KNOW
| Eponym | What it is | Significance |
|---|---|---|
| Badenoch's arteries | Paired vessels at 5 and 7 o'clock at bladder neck floor | Control after middle lobe resection to stop floor bleeding |
| Arteries of Flocks | Vessels at 2 and 10 o'clock at bladder neck | Main lateral arterial supply; must be coagulated when lateral lobe falls back |
| Anterior commissure | Thin anterior prostate at 12 o'clock | Capsule exposed after just 1-2 chips here; starting point for lateral lobe liberation |
BLANDY'S TECHNIQUE FOR VERY LARGE PROSTATES (>50 g)
"Thanks to the instruments of today there is virtually no limit to the size of prostate that can be resected transurethrally so long as the surgeon can keep clearly orientated and maintain concentration and patience... it is hardly more difficult to remove 100 g than 40 g, since the steps of the operation are the same even though they take a little longer."
- Prophylactic rollerball coagulation at 10, 2, 5, 7 o'clock first (devascularise before cutting)
- Resect very bulky middle lobe - keep the mound flat and even
- Proceed with lateral lobes systematically as above
- Consider staged TURP if time limit approaching (>60 min rule)
COMPLETE COMPARISON TABLE OF ALL TURP TECHNIQUES
| Technique | Eponymist & Year | Starting Point | Sequence of Resection | Core Concept | Pros | Cons | Best For |
|---|---|---|---|---|---|---|---|
| Nesbit | Reed Nesbit, USA, 1943 | 12 o'clock (anterior roof) | 12 o'clock proximal → clockwise around bladder neck → lateral lobes fall back → apex last | Devascularise roof first; gravity causes lateral lobes to fall posteriorly | ✅ Gold standard; most widely taught ✅ Early vascular control at 12 o'clock ✅ Gravity assists lateral lobe resection ✅ Best evidence base ✅ Systematic orientation maintained | ❌ Bulk lateral tissue impedes view until removed ❌ Partial resection of lateral lobes mid-procedure causes bleeding ❌ Can't easily stop half-way | Any prostate size; standard choice for trainees |
| Mauermayer | W. Mauermayer, Germany, 1985 | 5-7 o'clock (floor / middle lobe) | Middle lobe → floor channel (5-7 o'clock) → side lobes → ventral → apex last | Open the floor first to establish immediate drainage and irrigation flow | ✅ Best for prominent middle lobe ✅ Immediate irrigation improvement ✅ Most obstructive tissue removed first ✅ Good visibility from outset | ❌ No early devascularisation of lateral vessels → more bleeding early ❌ Less logical for glands without middle lobe | Prominent/intravesical middle lobe; obstructing bladder neck |
| Milner | William A. Milner, USA, 1941 | 9 or 3 o'clock (extreme lateral) | Median lobe (if present) → full-length groove at 9 or 3 → complete one entire lateral lobe → opposite lobe → posterior → apex | One complete lobe at a time; direct perpendicular attack on bulk tissue | ✅ Can safely stop mid-procedure (one complete haemostatic lobe done) ✅ Immediate attack on bulk obstruction ✅ Capsular groove at thickest point (safest place for accidental breach) ✅ Better irrigation and scope mobility early | ❌ No early devascularisation ❌ Requires speed and skill to control bleeding ❌ Steeper learning curve ❌ 2-handed resectoscope required (as originally described) | Large lateral lobes; when staged procedure anticipated |
| Blandy | John Blandy, UK, 1971 | Middle lobe (5-7 o'clock), then 1 o'clock for lateral lobes | Middle lobe resection → control Badenoch's arteries (5,7 o'clock) → anterior commissure (12) → liberate lateral lobe → falls back → control Flocks' arteries (2,10) → resect fallen lobe → repeat opposite side → careful apex | Systematic landmark-based approach; specific named arterial control at each stage; extreme apical caution | ✅ Highly systematic and teachable ✅ Named arterial landmarks (Badenoch, Flocks) built into technique ✅ Rollerball pre-coagulation option for large glands ✅ Emphasises apical safety above all ✅ Ideal for training (Blandy's textbook is reference standard) | ❌ More steps = longer operative time for beginners ❌ Requires knowledge of specific anatomical arterial landmarks ❌ Technique described primarily for monopolar | Standard glands; UK/Commonwealth training; all sizes with modification |
| Barnes | Robert Barnes, USA | Posterior lobe (6 o'clock) | Posterior lobe first → lateral lobes → ventral portions → apex | Secure posterior lobe early; establish immediate irrigation drainage | ✅ Posterior lobe secured early (hardest when floor is full of chips) ✅ Immediate irrigation flow | ❌ Only practical for larger prostates ❌ In small glands, lateral lobes may rise superiorly | Large prostates with bulky posterior lobe |
| Alcock | Nathaniel Alcock, USA | Lower lateral lobe base (undermining) | Undermine lower lateral lobe → lobe falls into fossa → resect fallen tissue → repeat other side → apex | Use gravity to prolapse lobe into field after undermining | ✅ Gravity-assisted prolapse of lobe ✅ Logical for heavy lateral lobes | ❌ Only works for large/heavy lateral lobes ❌ In small glands, lobes rise upward instead of falling → makes resection harder ❌ Rarely used today | Large prostates with heavy lateral lobes only |
| Flocks | Rubin H. Flocks, USA, 1937 | Posterior lateral sulcus | Posterior sulcus → expose capsule posterolaterally → work anteriorly → apex | Establish posterior capsule landmark early via the sulcus | ✅ Early posterior capsule identification ✅ Systematic posterior-to-anterior approach | ❌ Less commonly taught ❌ Posterior sulcus can be difficult to visualise in small glands | Moderate-large glands |
HOW THE TECHNIQUES RELATE TO EACH OTHER
WHERE TO START
│
┌─────────────┼──────────────┐
12 o'clock 5-7 o'clock 9/3 o'clock Post sulcus
(Anterior) (Floor/Middle) (Extreme lat) (Posterior lat)
│ │ │ │
NESBIT MAUERMAYER MILNER FLOCKS
BLANDY* BLANDY* (one lobe
(step 2) (step 1) at a time)
│
6 o'clock
(Posterior)
│
BARNES
│
Undermine base
│
ALCOCK
*Blandy = hybrid: starts with middle lobe (like Mauermayer/Barnes),
then uses anterior commissure approach (like Nesbit) for lateral lobes
COMMON THREAD - THE ARTERIES YOU MUST KNOW
| Artery Name | Position | When to Control |
|---|---|---|
| Badenoch's arteries | 5 and 7 o'clock at bladder neck | After completing middle lobe resection |
| Arteries of Flocks | 2 and 10 o'clock at bladder neck | When lateral lobe falls back after anterior commissure cut |
Examiner question: "What are Badenoch's arteries and when do you encounter them?" Answer: Badenoch's arteries are paired vessels entering the prostate at 5 and 7 o'clock at the level of the bladder neck. They are the main blood supply to the floor of the prostate. In Blandy's technique, they are specifically coagulated after the middle lobe resection is complete to secure haemostasis of the floor before proceeding to lateral lobe resection.
Examiner question: "What are Flocks' arteries?" Answer: Described by Rubin Flocks in his 1937 paper on prostatic arterial distribution. They enter at 2 and 10 o'clock at the bladder neck and are the dominant arterial supply to the lateral lobes. In Blandy's technique, as the anterior commissure cut is made and the lateral lobe falls backwards, these vessels are encountered and must be coagulated before resecting the fallen lobe tissue.
QUICK MEMORY AID
| Technique | Remember By |
|---|---|
| Nesbit | "Noon first" - starts at 12 o'clock |
| Mauermayer | "Middle lobe first" - 5-7 o'clock floor |
| Milner | "Mono-lobe" - completes one lobe at a time |
| Blandy | "British, Badenoch, Be careful at apex" |
| Barnes | "Back first" - posterior lobe |
| Alcock | "All about gravity" - undermine and let fall |
| Flocks | "Fossa sulcus" - posterior lateral groove |