Ankylosis spondylosis
Reading File
Finding Sources
Searching PubMed
"ankylosing spondylitis"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from the textbooks with excellent imaging. Let me compile the full answer.
Ankylosing Spondylitis (AS)
Note on terminology: The term "Ankylosing Spondylosis" is a common misnomer. The correct condition is Ankylosing Spondylitis (AS) - spondylosis refers to degenerative disc disease, while spondylitis refers to inflammation. AS is now classified as radiographic axial spondyloarthritis (r-AxSpA) under modern terminology.
Definition
Ankylosing spondylitis is a multisystem inflammatory spondyloarthropathy primarily affecting the axial skeleton. It belongs to the family of spondyloarthritides, which also includes psoriatic arthritis, reactive arthritis, and enteropathic arthritis. The Assessment of SpondyloArthritis international Society (ASAS) classifies it as radiographic axial spondyloarthritis - structural damage visible on plain radiographs of the sacroiliac (SI) joint distinguishes it from non-radiographic axial spondyloarthritis.
- Goldman-Cecil Medicine, 26e, Ch. 244
Epidemiology
- Prevalence parallels that of HLA-B27 in any given population
- Predominantly affects HLA-B27-positive adolescents and young adults
- Male-to-female ratio roughly 2-3:1 (though females are increasingly recognized)
- About 90% of AS patients are HLA-B27 positive
- HLA-B27 prevalence is ~7% in Northern Europeans/North American Whites; virtually absent in Australian aboriginals; ~1% in Japan; up to 50% in some Western Canadian indigenous tribes
- May be as common as rheumatoid arthritis
Pathobiology
Genetic Susceptibility
The strongest genetic association is with HLA-B27 on the short arm of chromosome 6. Over 30 subtypes of B27 exist; B2705 is the primordial subtype. Notably, subtypes B2706 and B2709 do NOT appear to confer susceptibility to AS. Non-HLA genes (ERAP1, IL-23R, IL-17 pathway genes) also contribute.
Mechanism of Inflammation and New Bone Formation
The primary pathological target is the enthesis - the site where tendons, ligaments, and joint capsules attach to bone. Inflammation at entheses (enthesitis) leads to:
- Erosive bone destruction
- Reactive new bone formation (syndesmophytes)
- Progressive ossification and fusion
The IL-17/IL-23 axis and TNF-alpha are key cytokine drivers. Paradoxically, TNF inhibitors suppress inflammation but may not halt new bone formation (syndesmophyte progression), suggesting these two processes are partly uncoupled.
Clinical Features
Hallmark: Inflammatory Back Pain
Distinguishing features from mechanical back pain:
| Feature | Inflammatory (AS) | Mechanical |
|---|---|---|
| Onset | Insidious, <40 yrs | Acute or insidious, any age |
| Morning stiffness | >1 hour | Brief (<30 min) |
| Response to exercise | Improves | Worsens |
| Response to rest | Worsens | Improves |
| Night pain | Yes, wakes patient | Uncommon |
Axial Involvement
- Sacroiliitis - hallmark; bilateral and symmetrical in AS (unlike psoriatic/reactive arthritis which is asymmetrical)
- Lumbar, thoracic, and cervical spine involvement
- Costovertebral joint involvement reducing chest expansion
- Cervical spine fusion in advanced disease
Peripheral Joint Involvement
- Seen in up to 30% of patients
- Hip joint is the second most commonly affected joint after the SI joint
- Lower limb oligoarthritis pattern (similar to other spondyloarthritides)
- Enthesitis - Achilles tendinitis, plantar fasciitis are common
Extra-articular Manifestations
| System | Manifestation |
|---|---|
| Eyes | Acute anterior uveitis - most common extra-articular feature |
| Heart | Aortitis, aortic regurgitation, conduction defects |
| Lungs | Upper lobe bilateral reticulonodular infiltrates with cyst formation (apical fibrobullous disease) - no effective therapy known |
| Kidneys | IgA nephropathy, secondary amyloidosis |
| Bowel | Subclinical gut inflammation in ~60%; frank IBD in some |
Radiological Features
Sacroiliac Joints
MRI detects the earliest change - subchondral bone marrow oedema (active sacroiliitis), before plain radiograph changes.
Plain X-ray/CT progression:
- Erosions + subchondral sclerosis
- Joint space irregularity
- Bony ankylosis (complete fusion)
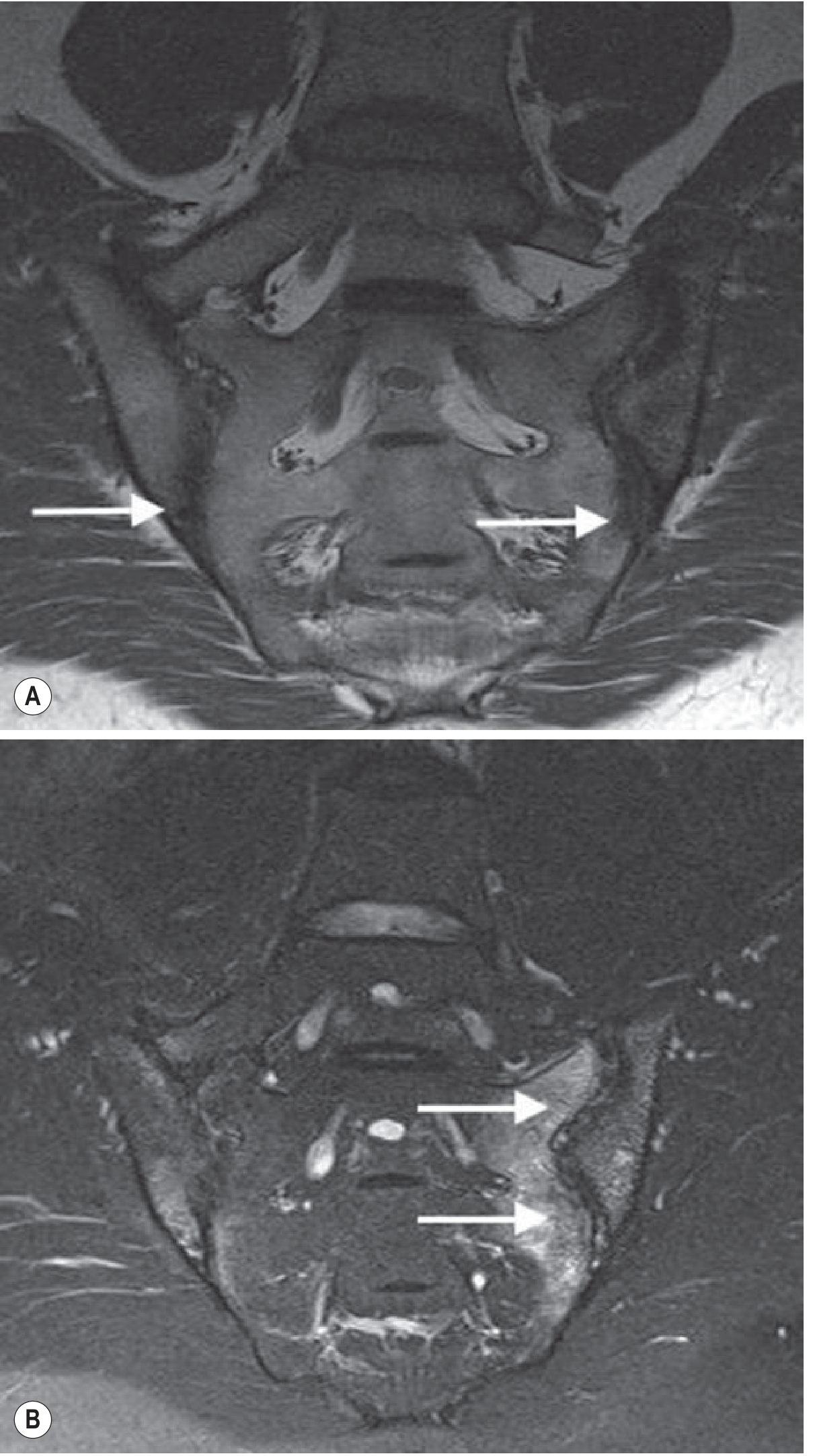
T1 (A): erosions in the SIJ with joint space loss (damage). T2 fat-suppressed (B): extensive subchondral oedema reflecting active disease activity - Grainger & Allison's Diagnostic Radiology
Spine - Sequential Changes
- Romanus lesions - sclerotic "shiny corners" at vertebral body corners (enthesitis at Sharpey fiber insertion). On MRI, this appears as bone oedema at vertebral body corners before sclerosis is visible on plain X-ray.
- Squared vertebral bodies - erosion + anterior longitudinal ligament ossification
- Syndesmophytes - thin, vertically oriented bone outgrowths (contrast with the bulky, nonmarginal, asymmetrical syndesmophytes of reactive arthritis)
- Bamboo spine - complete fusion of vertebral bodies AND sacroiliac joints in advanced/untreated disease
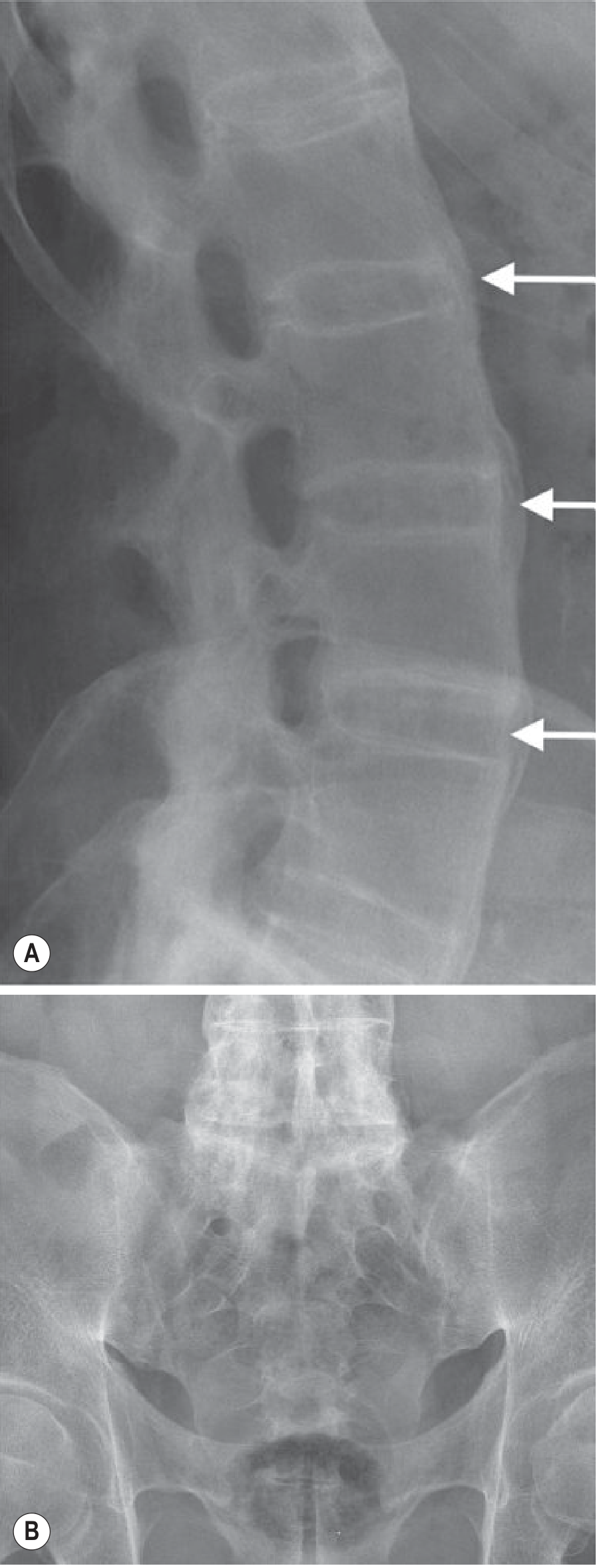
Classic "bamboo spine" - bridging vertical syndesmophytes around intervertebral discs with no facet joint spaces visible, indicating posterior fusion (L3-S1). AP pelvis showing complete bony fusion of both sacroiliac joints - Grainger & Allison's
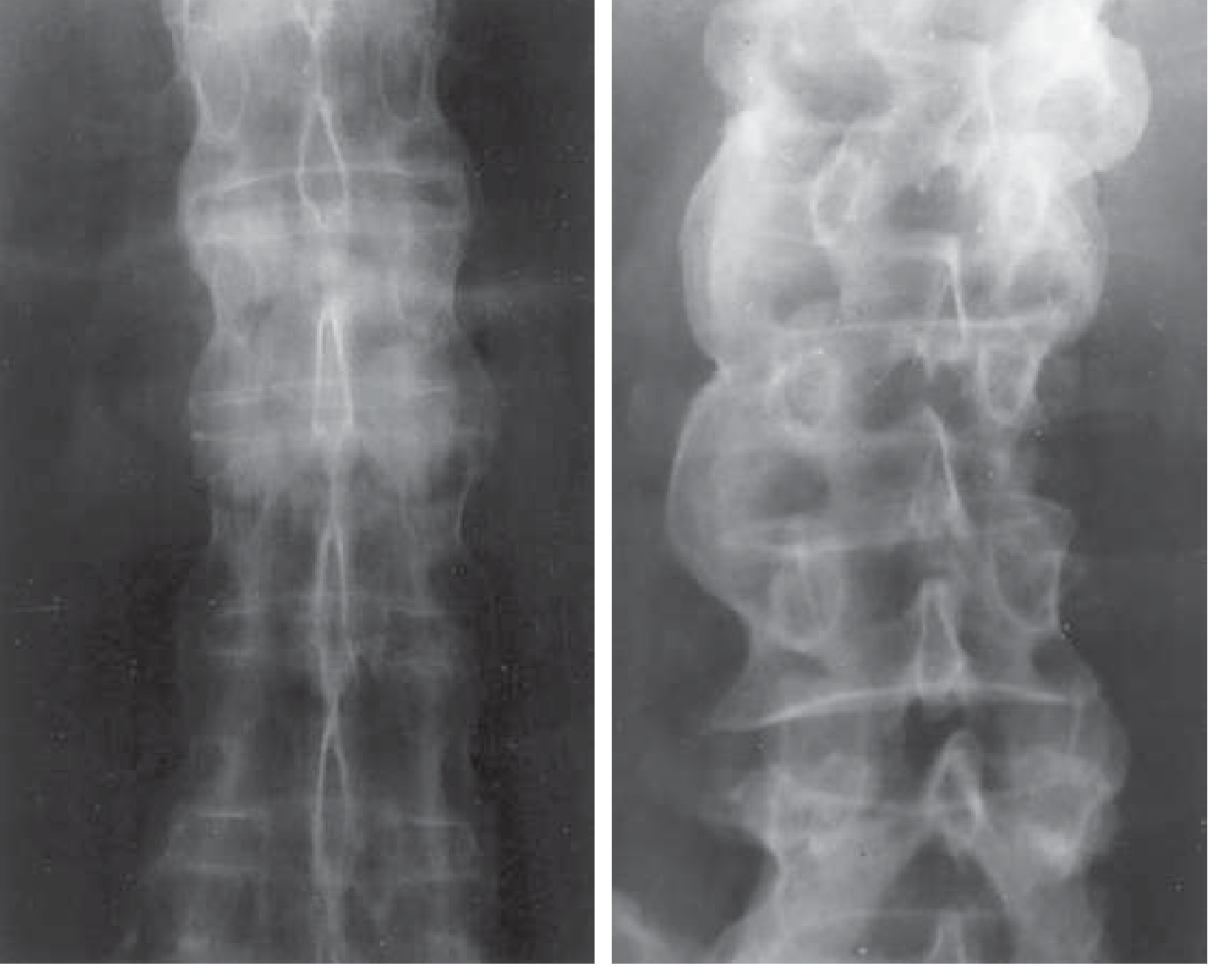
Left: AS showing symmetrical marginal bridging syndesmophytes with spinal ligament calcification. Right: reactive arthritis showing bulky, nonmarginal, asymmetrical syndesmophytes - Goldman-Cecil Medicine
Spinal Fracture Risk
Despite apparent sclerosis, patients are osteopenic. A fused, rigid spine is extremely vulnerable to transverse fractures - these are highly unstable and frequently catastrophic, even from minimal trauma.
Hip Joint
Diffuse joint space loss with preserved bone density. A cuff of entheseal new bone around the femoral head creates a somewhat flattened appearance that can mimic a cam deformity (femoroacetabular impingement).
Andersson Lesion
In a largely fused spine, movement at unfused levels can cause an inflammatory discovertebral lesion (Andersson lesion) - the irregularity and sclerosis can be mistaken for infection.
Diagnosis
ASAS Classification Criteria for Axial Spondyloarthritis
Age of onset <45 years + chronic back pain ≥3 months, PLUS:
Imaging arm: Sacroiliitis on MRI or X-ray + ≥1 SpA feature
Clinical arm: HLA-B27 positive + ≥2 SpA features
Clinical arm: HLA-B27 positive + ≥2 SpA features
SpA features include: Inflammatory back pain, arthritis, enthesitis (heel), uveitis, dactylitis, psoriasis, Crohn's/UC, good response to NSAIDs, family history of SpA, HLA-B27, elevated CRP.
Laboratory
- HLA-B27: positive in ~90%
- CRP/ESR: elevated (correlates with disease activity but can be normal)
- Rheumatoid factor and ANA: negative (seronegative arthritis)
Imaging Summary
- Plain X-ray: First-line; shows late changes (sclerosis, erosions, syndesmophytes, bamboo spine)
- MRI: Best for early disease - detects active bone marrow oedema (sacroiliitis) before X-ray changes
- CT: Best for assessing bony detail, erosions, and ankylosis but involves radiation
- Scintigraphy: Historical role; now superseded by MRI (lower sensitivity/specificity)
Treatment
Non-pharmacological
- Physiotherapy and exercise - maintain spinal mobility and posture
- Swimming, hydrotherapy
- Smoking cessation (smoking accelerates structural damage)
Pharmacological
Step 1 - NSAIDs
- First-line therapy (Grade A evidence - Cochrane review)
- Continuous NSAIDs may slow radiographic progression (unlike in RA)
- Options: indomethacin, naproxen, diclofenac, celecoxib
Step 2 - Biologics (for inadequate NSAID response)
| Class | Agents | Notes |
|---|---|---|
| TNF inhibitors | Etanercept, adalimumab, infliximab, certolizumab, golimumab | First biologic class proven effective; rapidly reduce inflammation |
| IL-17A inhibitors | Secukinumab, ixekizumab | Effective in TNF-naive and TNF-inadequate responders; preferred if IBD absent (may worsen IBD) |
| IL-12/23 inhibitor | Ustekinumab | Less robust evidence for AS vs PsA |
| JAK inhibitors | Tofacitinib, upadacitinib | Oral options; evidence accumulating |
Step 3 - Local therapy
- Intra-articular corticosteroid injections (peripheral joints, SI joints under imaging guidance)
- Systemic corticosteroids are generally NOT effective for axial disease
Note on conventional DMARDs
Sulfasalazine and methotrexate have limited efficacy for axial disease but may help peripheral arthritis.
Surgical
- Total hip replacement - for severe hip disease
- Spinal surgery (osteotomy) for severe fixed kyphosis
- No role for surgery in axial disease prophylactically
Prognosis and Complications
The clinical course is highly variable. Key points:
- The strongest predictor of new syndesmophyte formation is the presence of syndesmophytes at baseline
- Osteoporosis is a significant complication (both local chronic inflammation and abnormal biomechanical loading)
- Late complications: cauda equina syndrome, osteoporotic compression fractures, spondylodiscitis, restrictive lung disease
- Intervertebral fracture can occur after minimal trauma in late disease
- Patients with refractory new spinal pain need urgent imaging to exclude fracture
Sources:
- Goldman-Cecil Medicine, International Edition (26e), Chapter 244 - Spondyloarthritis
- Grainger & Allison's Diagnostic Radiology, Chapter 44 - Ankylosing Spondylitis
- Murray & Nadel's Textbook of Respiratory Medicine - Pulmonary manifestations of AS
This is a shared conversation. Sign in to Orris to start your own chat.