Traimcinolone injection in alopecia areata, and keloid detail procedure and strength of traimcinolone used
Reading File
Finding Sources
Finding Sources
Searching PubMed
triamcinolone intralesional injection alopecia areata
Searching PubMed
triamcinolone intralesional keloid treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive, well-sourced answer.
Triamcinolone Acetonide (TA) Intralesional Injection - Alopecia Areata & Keloid
PART 1: ALOPECIA AREATA
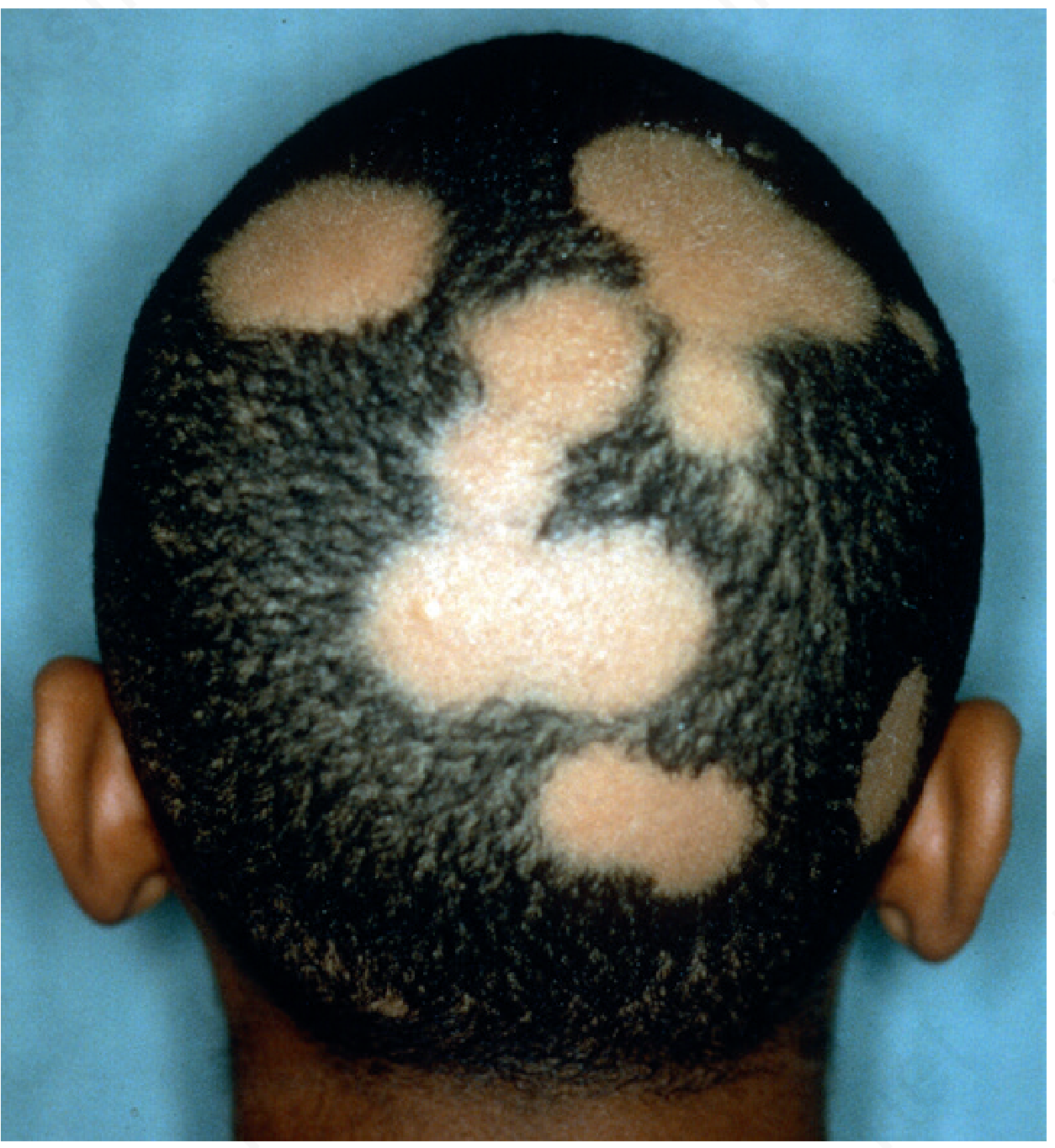
Indication for Injection
Intralesional corticosteroid injection is the treatment of choice for localized, cosmetically conspicuous patches - particularly those at the frontal hairline or involving an eyebrow. It is categorized as "least responsive to topical therapy" and requires intralesional injection for effective results.
Strength (Concentration)
| Setting | Concentration |
|---|---|
| Standard therapeutic range | 2-10 mg/mL |
| Typical clinical use | 5 mg/mL (most common starting point) |
| Higher concentration (more potent) | Up to 10 mg/mL |
Key caution: Large volumes and higher concentrations carry a greater risk of local skin atrophy. Injecting under significant pressure or with a small-bore syringe increases the risk of retinal artery embolization (a rare but serious complication) - this is particularly relevant near the periorbital area.
Procedure - Step by Step
-
Patient selection: Localized patchy alopecia, cosmetically significant sites (frontal hairline, eyebrow, beard). Not first-line for alopecia totalis/universalis.
-
Preparation: Draw up triamcinolone acetonide suspension (dilute commercial 40 mg/mL stock with normal saline or lidocaine to target concentration of 2-10 mg/mL).
-
Syringe and needle: Use a 1 mL tuberculin syringe with a 30-gauge needle (short).
-
Injection plane: Deliver intradermally or in the superficial subcutaneous tissue - NOT deep subcutaneous (to avoid atrophy of deeper tissues and systemic spread).
-
Technique: Multiple small blebs are raised across the patch, spaced ~1 cm apart. Each injection site receives approximately 0.05-0.1 mL.
-
Dose per site: Limit to approximately 1 mg per treatment site (i.e., 0.1 mL of a 10 mg/mL suspension per point) to minimize local atrophy.
-
Total session dose: Keep total dose per session within safe limits to minimize HPA axis suppression.
-
Injection interval: Repeat every 4-6 weeks as needed; hair regrowth is typically seen after 4-8 weeks.
Expected Response
- Regrowth is typically observed in cosmetically significant patches; patchy disease responds best.
- Ophiasic alopecia areata tends NOT to respond.
- High rate of spontaneous recovery must be factored into evaluating treatment success.
Adverse Effects
- Local skin atrophy (most common)
- Hypopigmentation from lymphatic spread of corticosteroid
- Telangiectasia
- Retinal artery embolization (rare, especially near periorbital region)
- HPA axis suppression with excessive use
PART 2: KELOID
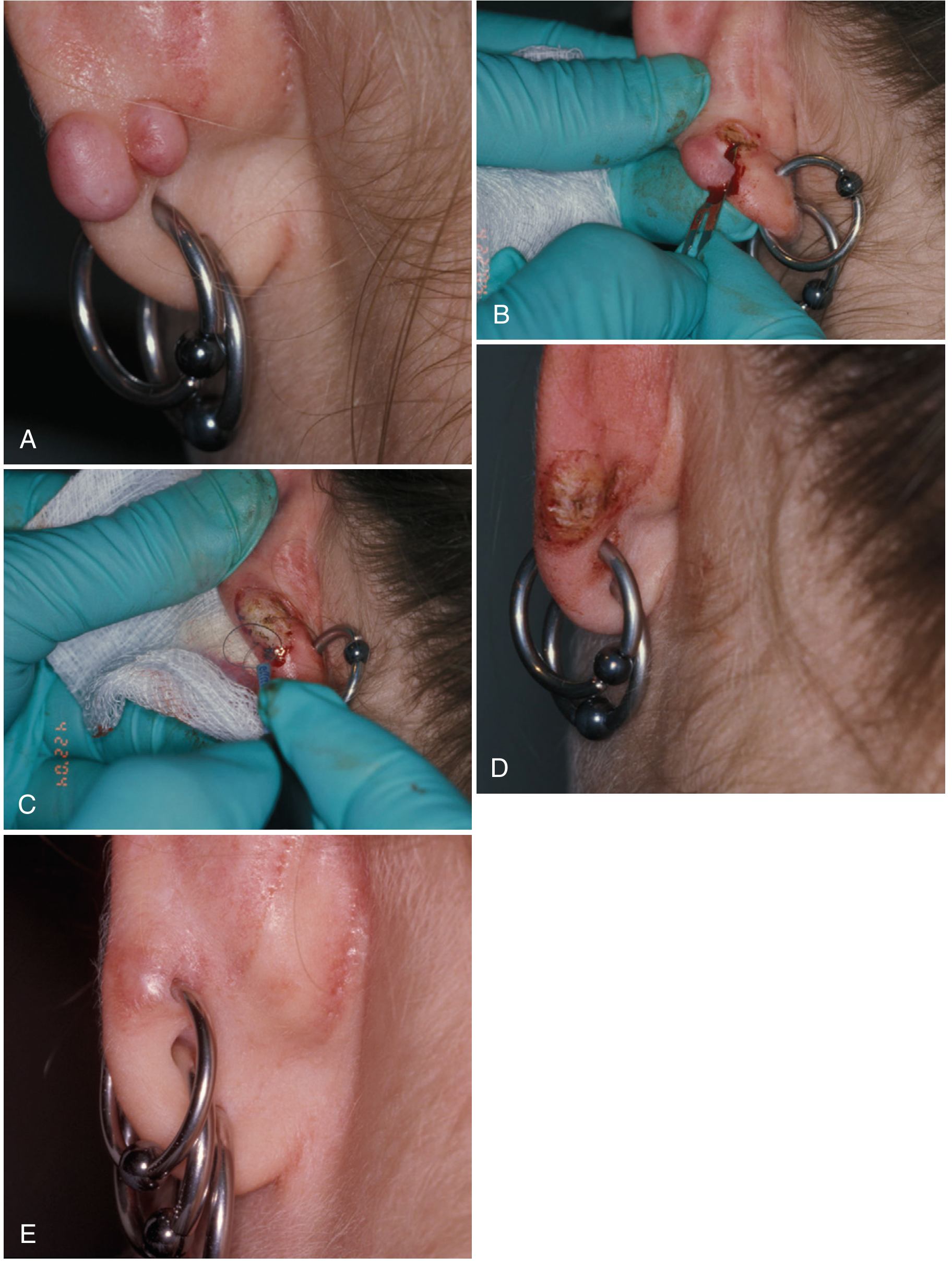
Background
Keloids are benign, fibrous proliferations of collagen that expand beyond the original wound boundaries. They have 20x normal collagen synthesis enzyme levels. Triamcinolone acetonide (TA) reduces keloid fibroblast proliferation and collagen production, partly through a statistically significant decrease in TGF-β1 levels.
Strength (Concentration)
| Setting | Concentration |
|---|---|
| Initial treatment / young keloid | 40 mg/mL |
| As lesion softens (maintenance) | 10-20 mg/mL |
| Starting concentration (some protocols) | 10 mg/mL, titrated up to 40 mg/mL |
| Post-excision maintenance | 10 mg/mL initially |
The higher starting dose of 40 mg/mL is used for keloids because they are dense, fibrous, and highly resistant - unlike alopecia areata which requires much lower concentrations.
Procedure - Step by Step
-
Anesthesia: For large/painful keloids, local anesthesia with lidocaine may be injected first. A dilute steroid can be included in the anesthetic mixture.
-
Syringe and needle: Use a 1 mL tuberculin Luer syringe with a 30-gauge needle. Because keloids are very firm and dense, significant force is needed - use a Luer-lock syringe to prevent the needle from popping off.
-
Technique: Insert the needle directly into the substance of the keloid (intralesional). Inject triamcinolone suspension into various parts of the lesion, distributing it throughout.
-
Blanching endpoint: Inject until the lesion blanches white (indicates adequate tissue saturation and even distribution).
-
Injection interval: Repeat at 6-8 week intervals as required, until the keloid flattens and pruritus ceases.
-
Combination therapy: TA 40 mg/mL may be combined with 5-fluorouracil (5-FU 50 mg/mL mixed with TA 1 mg/mL) for refractory keloids, or combined with long-pulsed Nd:YAG laser, verapamil, or methotrexate.
For Old/Established Keloids
- Excise the keloid first using lidocaine with triamcinolone as the local anesthetic.
- Follow immediately with intralesional TA injections at the wound site.
- Repeat injections at 2-week intervals post-excision.
- Can be combined with postoperative irradiation or topical imiquimod.
- Monitor for recurrence every 3 months for 1-2 years.
Expected Response
- Flattening of the keloid and cessation of itching are reliably achieved.
- The lesion will NOT become narrower with injection alone.
- Hyperpigmentation generally persists.
- Young keloids respond better than old established ones.
Adverse Effects
| Adverse Effect | Notes |
|---|---|
| Skin atrophy | From high concentration or perilesional spread |
| Hypopigmentation | Lymphatic spread of TA, especially dark skin |
| Telangiectasia | Around injection site |
| Ulceration | More common with 5-FU combination |
| Hyperpigmentation | Persists even after treatment |
COMPARISON SUMMARY
| Parameter | Alopecia Areata | Keloid |
|---|---|---|
| Standard concentration | 2-10 mg/mL | 40 mg/mL (initial) |
| Injection plane | Intradermal / superficial subcutaneous | Intralesional (into the body of the lesion) |
| Needle | 30-gauge | 30-gauge (Luer-lock syringe for keloid) |
| Volume per point | 0.05-0.1 mL | Distribute throughout lesion to blanching |
| Interval | Every 4-6 weeks | Every 6-8 weeks |
| Endpoint | Hair regrowth | Blanching of lesion, flattening, itch relief |
| Risk of atrophy | High (use lower concentrations) | Lower (dense tissue) |
Sources:
- Andrews' Diseases of the Skin, Clinical Dermatology - Keloid section & Alopecia Areata section
- Fitzpatrick's Dermatology Vol. 1 - Scar formation section
- Pfenninger & Fowler's Procedures for Primary Care, 3rd ed. - Hypertrophic scars and keloids chapter
- Katzung's Basic and Clinical Pharmacology, 16th ed. - Intralesional corticosteroids section
Recent evidence: A 2024 network meta-analysis (PMID 38285997) confirmed intralesional TA remains one of the most widely used keloid interventions, with combination TA + 5-FU showing improved outcomes compared to either agent alone.
PIED detail
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.