What's vertigo
Reading File
Searching the Web
vertigo causes symptoms treatment 2025
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a thorough breakdown of vertigo:
What Is Vertigo?
Vertigo is the perceived sensation of motion - usually spinning - of yourself relative to the environment, or of the environment spinning around you. It is a symptom, not a disease, and must be distinguished from other forms of dizziness such as presyncope (feeling faint), lightheadedness, or general disequilibrium (imbalance).
The sense of balance depends on coordinated input from the inner ear, eyes, musculoskeletal system, cardiovascular system, and brain. A disruption to any of these can cause dizziness - but true vertigo specifically points to a problem in the vestibular system.
Types of Vertigo
Vertigo is classified into two main types:
1. Peripheral Vertigo (most common - 38-56% of cases)
Arises from the inner ear (labyrinth) or vestibular nerve. Tends to be episodic rather than constant.
2. Central Vertigo (less than 10% of cases)
Arises from the brain - cerebellum, brainstem, thalamus, or cortex. Tends to be constant and may be accompanied by focal neurological deficits.
The following diagram from Cummings Otolaryngology maps this out clearly:
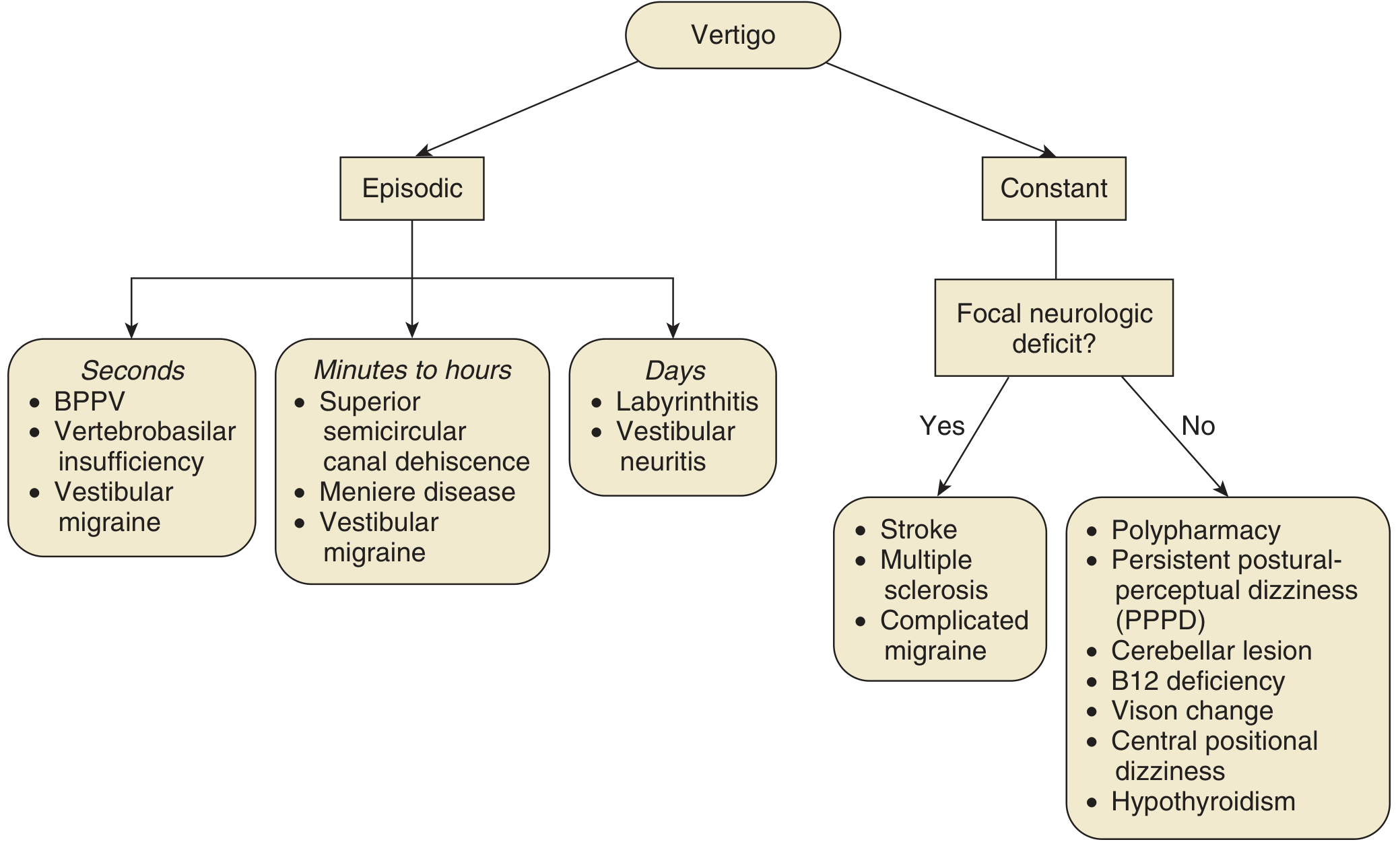
Common Causes
| Category | Duration | Examples |
|---|---|---|
| Peripheral - episodic (seconds) | Seconds | BPPV, vertebrobasilar insufficiency, vestibular migraine |
| Peripheral - episodic (minutes-hours) | Minutes to hours | Meniere's disease, superior semicircular canal dehiscence, vestibular migraine |
| Peripheral - episodic (days) | Days | Labyrinthitis, vestibular neuritis |
| Central - with focal deficit | Constant | Stroke, multiple sclerosis, complicated migraine |
| Central - no focal deficit | Constant | Polypharmacy, cerebellar lesion, B12 deficiency, hypothyroidism, PPPD |
BPPV (Benign Paroxysmal Positional Vertigo) is the single most common cause - caused by calcium carbonate crystals (otoliths) becoming dislodged in the semicircular canals of the inner ear.
Key Symptoms
- Spinning sensation (you or the room spinning)
- Nausea and vomiting
- Nystagmus (involuntary eye movement)
- Balance problems or tendency to fall
- Tinnitus or hearing loss (when inner ear is involved, e.g., Meniere's)
Important distinguishing feature: Nystagmus in peripheral vertigo is horizontal or rotary; vertical nystagmus occurs only in central vertigo and is a red flag. Neurologic symptoms (weakness, diplopia, memory loss) suggest a central cause.
Head movement almost always worsens peripheral vertigo. If it does not, consider a non-vestibular cause.
Diagnosis
- History accounts for ~85% of the diagnostic workup
- Dix-Hallpike maneuver - gold standard for diagnosing BPPV
- Physical exam - orthostatic BP, cranial nerves, Romberg test, gait, tuning forks (Weber & Rinne)
- Audiogram - if inner ear pathology is suspected
- Electronystagmography (ENG) - objective study of vestibular function
- MRI brain - indicated for unilateral ear symptoms, central signs, or treatment-resistant cases
- Blood tests - CBC, B12, folate, RPR, thyroid function when clinically indicated
Treatment
Treatment is directed at the underlying cause:
| Cause | Treatment |
|---|---|
| BPPV | Epley maneuver (canalith repositioning) - highly effective |
| Vestibular neuritis | Corticosteroids, vestibular suppressants (short-term), vestibular rehabilitation |
| Meniere's disease | Low-sodium diet, diuretics, intratympanic injections, surgery in refractory cases |
| Vestibular migraine | Migraine prophylaxis and acute treatment |
| Central causes (stroke, MS) | Treat the underlying condition |
| Psychogenic / PPPD | Cognitive behavioral therapy, SSRIs, vestibular rehabilitation |
Vestibular suppressants like meclizine or diazepam may provide short-term symptom relief but should not be used long-term as they can impair vestibular compensation.
Sources: Textbook of Family Medicine 9e, p. 393 | Cummings Otolaryngology Head and Neck Surgery
Create a quick reference guide on BPPV diagnosis and Epley maneuver procedure
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.