Brachial plexus
Reading File
Finding Sources
Searching the Web
brachial plexus anatomy roots trunks divisions cords branches
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have very comprehensive content. Let me compile the full answer.
Brachial Plexus
The brachial plexus is a somatic nerve plexus formed by the anterior rami (ventral rami) of C5 to C8 and most of T1. It originates in the neck between the anterior and middle scalene muscles, crosses over rib I, and enters the axilla to supply all motor and sensory innervation of the upper limb (except the trapezius and the skin over the axilla and dorsal scapula).
Gray's Anatomy for Students, p. 858
Schematic Overview
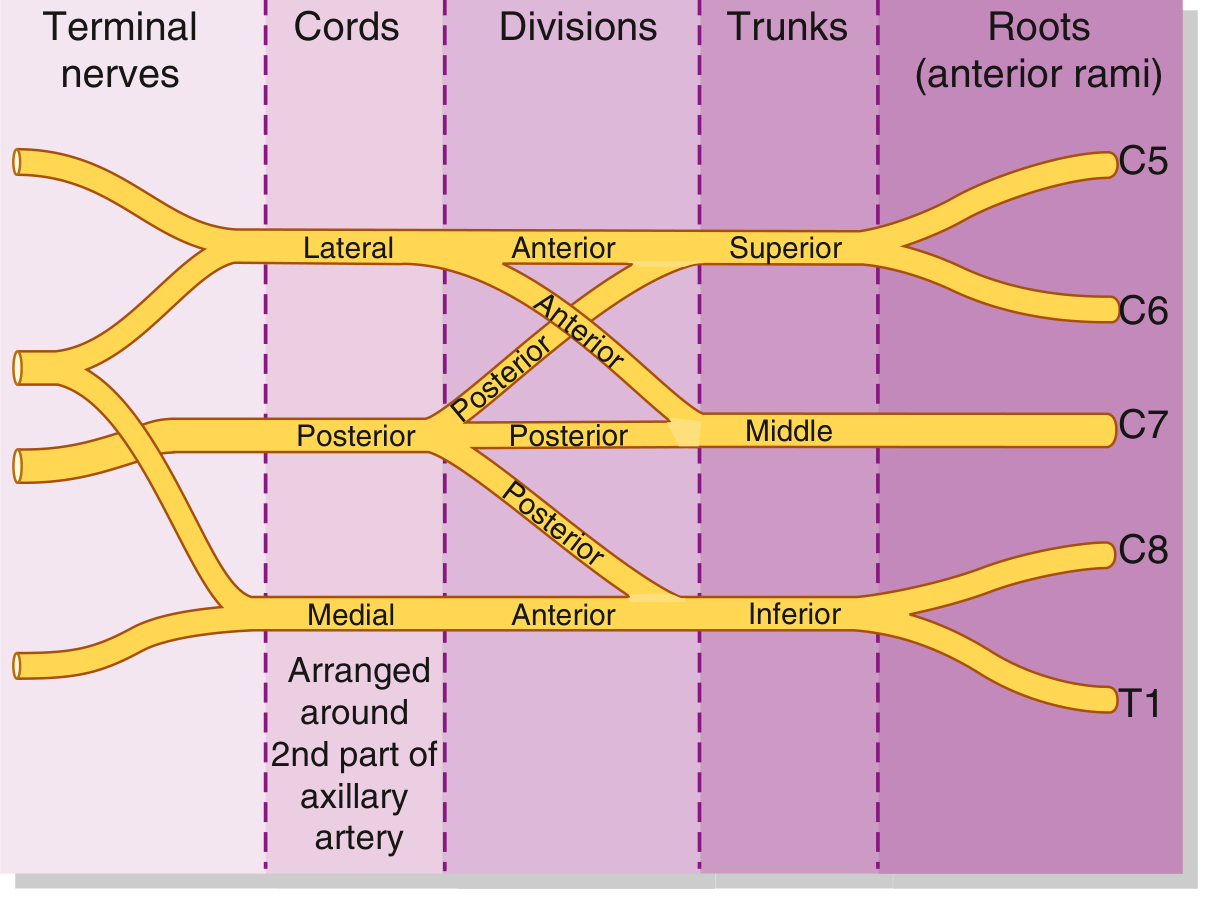
Components: Root to Branch (Mnemonic: Randy Travis Drinks Cold Beer)
Roots → Trunks → Divisions → Cords → Branches
1. Roots (5)
The roots are the anterior rami of C5, C6, C7, C8, and T1. They emerge between the anterior scalene and middle scalene muscles. Each root receives gray rami communicantes from the sympathetic trunk (postganglionic sympathetic fibers for peripheral distribution).
2. Trunks (3)
| Trunk | Formed by |
|---|---|
| Superior (upper) | C5 + C6 |
| Middle | C7 alone |
| Inferior (lower) | C8 + T1 |
The inferior trunk lies on rib I, posterior to the subclavian artery.
3. Divisions (6)
Each trunk splits into an anterior and a posterior division - 6 divisions total. No named peripheral nerves arise directly from divisions.
- Anterior divisions supply flexor (anterior) compartments
- Posterior divisions supply extensor (posterior) compartments
4. Cords (3)
The cords are named by their position relative to the 2nd part of the axillary artery:
| Cord | Formed from | Spinal levels | Position |
|---|---|---|---|
| Lateral | Anterior divisions of superior + middle trunks | C5, C6, C7 | Lateral to axillary artery |
| Medial | Anterior division of inferior trunk | C8, T1 | Medial to axillary artery |
| Posterior | All 3 posterior divisions | C5-T1 | Posterior to axillary artery |
Gray's Anatomy for Students, p. 859
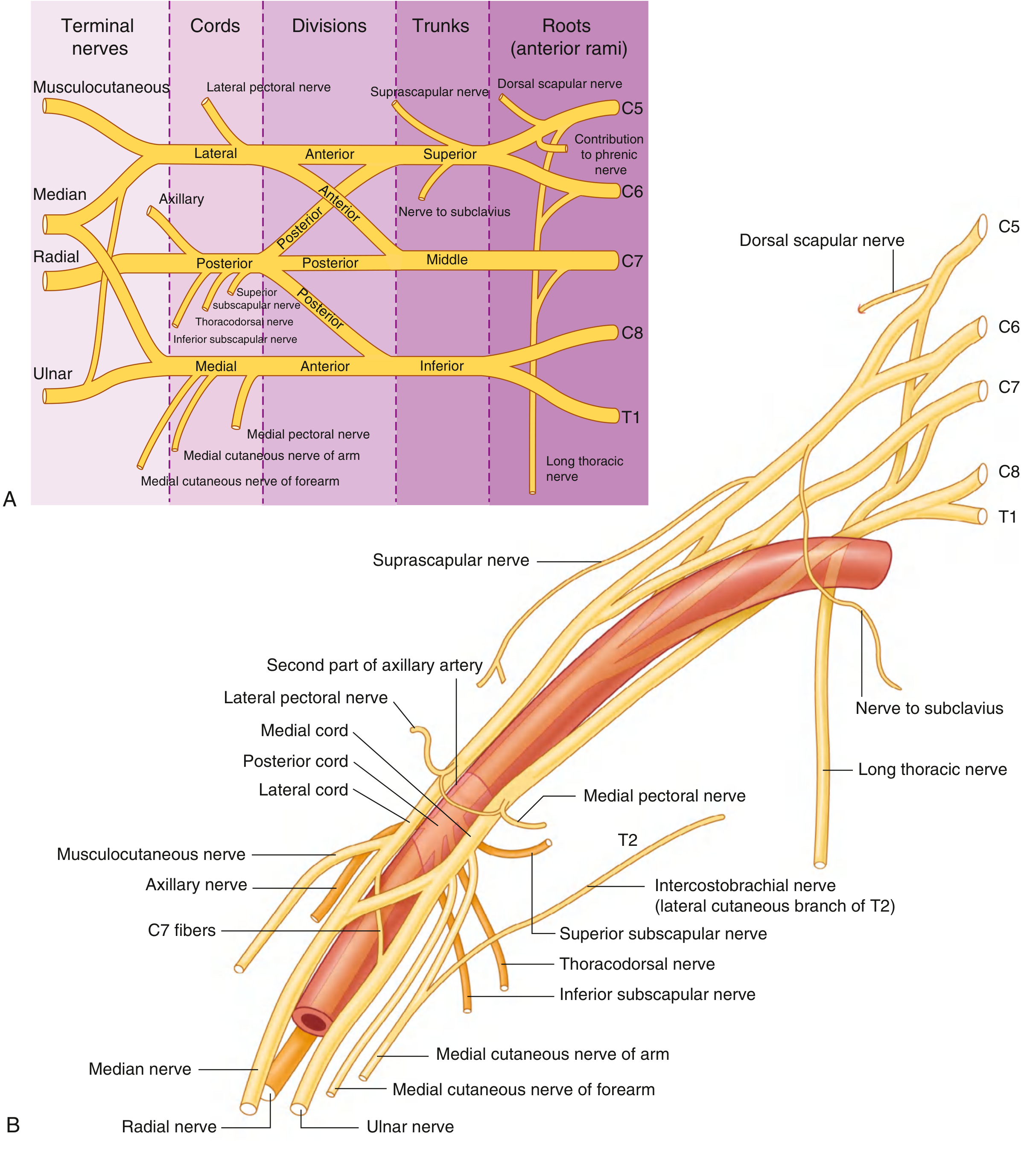
5. Branches (Terminal + Collateral)
From the Roots:
| Nerve | Root | Supplies |
|---|---|---|
| Dorsal scapular | C5 | Rhomboid major, rhomboid minor, levator scapulae |
| Long thoracic | C5, C6, C7 | Serratus anterior |
| Contribution to phrenic | C5 | Diaphragm (minor) |
From the Trunks (Superior trunk only):
| Nerve | Root | Supplies |
|---|---|---|
| Suprascapular | C5, C6 | Supraspinatus, infraspinatus |
| Nerve to subclavius | C5, C6 | Subclavius muscle |
From the Lateral Cord:
| Nerve | Supplies |
|---|---|
| Lateral pectoral nerve | Pectoralis major (clavicular head) |
| Musculocutaneous nerve (C5-C7) | Coracobrachialis, biceps brachii, brachialis; terminates as lateral cutaneous nerve of forearm |
| Lateral root of median nerve | (joins medial root to form median nerve) |
From the Medial Cord:
| Nerve | Supplies |
|---|---|
| Medial pectoral nerve | Pectoralis minor, pectoralis major (sternocostal head) |
| Medial cutaneous nerve of arm | Medial arm skin |
| Medial cutaneous nerve of forearm | Medial forearm skin |
| Ulnar nerve (C8, T1) | Intrinsic hand muscles, medial 1.5 fingers |
| Medial root of median nerve | (joins lateral root) |
From the Posterior Cord:
| Nerve | Supplies |
|---|---|
| Upper subscapular | Subscapularis (upper) |
| Thoracodorsal | Latissimus dorsi |
| Lower subscapular | Subscapularis (lower), teres major |
| Axillary nerve (C5, C6) | Deltoid, teres minor; lateral cutaneous nerve of arm |
| Radial nerve (C5-T1) | All posterior compartment muscles of arm and forearm |
The 5 Terminal Branches (Mnemonic: My Aunt Reads Mad Uncle)
- Musculocutaneous - from lateral cord
- Axillary - from posterior cord
- Radial - from posterior cord
- Median - from lateral + medial cords (both roots)
- Ulnar - from medial cord
A classic anatomical landmark: the median nerve, lateral cord, and ulnar nerve form a distinctive "M" or "W" shape in front of the axillary artery.
Anatomical Course
The plexus passes through the posterior triangle of the neck (roots and trunks), then under the clavicle (divisions), and into the axilla (cords and terminal branches). The cords wrap around the 2nd part of the axillary artery - this is how they get their names (lateral, medial, posterior).
Gray's Anatomy for Students, p. 858-861
Clinical Injuries
Erb-Duchenne Palsy (Upper Brachial Plexus Injury)
- Roots: C5 and C6
- Cause: Excessive widening of the angle between neck and shoulder - birth injury (shoulder dystocia), motorcycle accident, fall on the shoulder
- Muscles affected: Deltoid, biceps, brachialis, brachioradialis, supinator
- Deformity: "Waiter's tip" or "policeman's tip" - limb hangs in internal rotation, elbow extended, forearm pronated
- Sensory loss: Lateral arm and forearm
Klumpke's Palsy (Lower Brachial Plexus Injury)
- Roots: C8 and T1 (T1 more commonly)
- Cause: Forceful hyperabduction of the arm - breech delivery with arms up, grabbing an object while falling
- Muscles affected: Intrinsic hand muscles (both median and ulnar innervated)
- Deformity: Claw hand
- Sensory loss: Medial forearm, medial hand, medial 1.5 fingers
- Associated finding: Horner's syndrome (ptosis, miosis, anhidrosis, enophthalmos) - because T1 preganglionic sympathetic fibers are damaged. Presence of Horner's indicates a preganglionic (avulsion) lesion, which has a worse prognosis.
S Das Manual on Clinical Surgery, p. 140
Complete Brachial Plexus Injury
- Rare, usually from severe trauma
- Total paralysis and anesthesia of the upper limb (except the upper medial arm, supplied by C3-4 via intercostobrachial nerve)
Other Important Injuries
| Nerve | Common Cause | Effect |
|---|---|---|
| Long thoracic (C5-7) | Mastectomy, backpack | Medial winging of scapula (serratus anterior palsy) |
| Suprascapular (C5-6) | Overhead athletes, traction | Weakness of shoulder abduction and external rotation |
| Axillary (C5-6) | Anterior shoulder dislocation | Deltoid weakness, loss of shoulder abduction; patch of sensory loss over deltoid |
| Musculocutaneous (C5-7) | Coracobrachialis penetrating injury | Weak elbow flexion; loss of lateral forearm sensation |
| Radial (C5-T1) | Humeral shaft fracture (spiral groove) | Wrist drop |
| Ulnar (C8-T1) | Medial epicondyle fracture | Claw hand (ring and little fingers), loss of intrinsics |
Preganglionic vs. Postganglionic Injuries
| Feature | Preganglionic (avulsion) | Postganglionic |
|---|---|---|
| Site | Proximal to dorsal root ganglion | Distal to DRG |
| Horner's syndrome | Present (T1 avulsion) | Absent |
| Histamine flare test | Preserved (axon reflex intact) | Absent |
| EMG - paraspinal muscles | Denervated | Normal |
| Prognosis | No spontaneous recovery; nerve graft futile | May recover spontaneously or with repair |
Sympathetic Connection
The roots receive gray rami communicantes from the cervicothoracic (stellate) ganglion and inferior cervical ganglion. This is why lower trunk (C8/T1) injuries often disrupt sympathetic fibers to the eye, producing Horner's syndrome - the sympathetic fibers traveling with T1 to the superior cervical ganglion pathway are disrupted.
Gray's Anatomy for Students, p. 858; S Das Manual on Clinical Surgery, p. 140
This is a shared conversation. Sign in to Orris to start your own chat.